Download 206679Orig1s000 and more Exams Pharmacology in PDF only on Docsity!
CENTER FOR DRUG EVALUATION AND
RESEARCH
APPLICATION NUMBER:
206679Orig1s
CLINICAL PHARMACOLOGY AND
BIOPHARMACEUTICS REVIEW(S)
CLINICAL PHARMACOLOGY REVIEW
NDA 206-679 Serials 000; 003; 0011
Submission Dates June 22, 2015; October 6, 2015; February 26, 2016
Brand Name Not determined
Generic Name Simvastatin
Reviewer S.W. Johnny Lau, R.Ph., Ph.D.
Team Leader Jayabharathi Vaidyanathan, Ph.D.
OCP Division Clinical Pharmacology 2
OND Division Metabolism and Endocrinology Products
Sponsor Perrigo Pharmaceuticals
Formulation; Strength Suspension; 40 mg/5 mL and 20 mg/5 mL
Indication Adjunct therapy to diet to reduce elevated lipid
concentrations
Table of Contents Page
1 Executive Summary 1
1.1 Recommendations 1
1.2 Post Marketing Requirement 2
1.3 Summary of Important Clinical Pharmacology Findings 2
2 Question Based Review
2.1 Background 3
2.2 General Attributes 3
2.3 General Clinical Pharmacology 4
2.4 Bioanalytical 16
3 Label Recommendations 17
4 Appendix
4.1 Individual Study Synopsis 18
1 Executive Summary
The sponsor seeks approval of the 40 mg/5 mL and 20 mg/5 mL simvastatin oral suspension as an adjunct
therapy to reduce elevated lipid concentrations via the regulatory 505(b)(2) pathway. The innovator 10,
20, 40, and 80 mg simvastatin tablets (Zocor) have the indication to treat hyperlipidemia (NDA 19-
approved on December 23, 1991).
1.1 Recommendations
The Office of Clinical Pharmacology/Division of Clinical Pharmacology 2 (OCP/DCP2) has reviewed
NDA 206-679’s Clinical Pharmacology data submitted on June 22, 2015, October 6, 2015, and February
26, 2016. The data are acceptable to support approval. Due to the significant effect of food on the
exposure of simvastatin suspension, the product label needs to carry the following statement:
The recommended usual starting dose is 10 or 20 mg once a day in the evening on an empty
stomach.
2 Question-Based Review
2.1 Background
The sponsor is developing the oral 40 mg/5 mL and 20 mg/5 mL simvastatin suspension to treat
hypercholesterolemia via the regulatory 505(b)(2) pathway. The innovator 10, 20, 40, and 80 mg
simvastatin tablets have the indication to treat hypercholesterolemia.
The sponsor conducted the following 3 studies to support NDA 206-679:
PRG-NY-14-010: Bioequivalence between 80 mg simvastatin oral suspension (10 mL of 40
mg/5mL) and 80 mg simvastatin tablet (Zocor) under fasting
PRG-NY-14-011: Relative bioavailability of 80 mg simvastatin suspension (10 mL of 40
mg/5mL) in the presence of a high fat meal and under fasting
SC02806: Relative bioavailability study between 20 mg/5 mL of simvastatin suspension and 20
mg Zocor tablet
Because the 20 mg Zocor tablets used in Study SC02806 were the 20 mg Zocor marketed in the UK (Page
23 of 954 on Study SC02806’s report) and not the United States reference listed drug, this reviewer did
not review Study SC02806 for the support of NDA 206-679.
Besides simvastatin’s product label, the following publication details simvastatin’s clinical pharmacology:
Neuvonen P et al. Pharmacokinetic comparison of the potential over-the-counter statins
simvastatin, lovastatin, fluvastatin and pravastatin. Clin Pharmacokinet 2008;47:565463-74.
For simplicity, this reviewer refers the simvastatin metabolite, -hydroxyacid simvastatin, as simvastatin
acid in this review.
2.2 General Attributes
2.2.1 What are simvastatin’s key physicochemical properties?
Figure 1 shows the chemical structure of simvastatin, which has a molecular weight of 418.57 and
empirical formula of C 25 H 38 O 5.
Figure 1. Simvastatin’s molecular structure.
Source: Module 3.2.S.1.
2.2.2 What is the formulation for the to-be-marketed simvastatin oral suspension?
Tables 1 and 2 detail the formulations of the to-be-marketed immediate release simvastatin oral
suspension.
Table 1. Composition of the to-be-marketed simvastatin oral suspension 40 mg/5 mL.
Component
Compendial
Quality
Function
mg/5 mL
Dose
Formulation
%w/w
Simvastatin USP Active ingredient 40 0. Propylene Glycol USP Methylparaben NF Ethylparaben NF Propylparaben NF Magnesium Aluminum Silicate NF Carboxymethylcellulose Sodium NF Simethicone Emulsion USP Sodium Lauryl Sulfate NF Acesulfame Potassium NF Citric Acid Monohydrate USP Sodium Phosphate, Dibasic, Anhydrous USP Strawberry Flavoring NA Flavor
Water USP N/A NA NA = not applicable *Strawberry flavor contains % propylene glycol; specific amounts of the remaining ingredients are proprietary information. Source: Module 3.2.P.1.2 Table P.1.2-
Table 2. Composition of the to-be-marketed simvastatin oral suspension 20 mg/5 mL.
Component
Compendial
Quality
Function
mg/5 mL
Dose
Formulation
%w/w
Simvastatin USP Active ingredient 20 0. Propylene Glycol USP Methylparaben NF Ethylparaben NF Propylparaben NF Magnesium Aluminum Silicate NF Carboxymethylcellulose Sodium NF Simethicone Emulsion USP Sodium Lauryl Sulfate NF Acesulfame Potassium NF Citric Acid Monohydrate USP Sodium Phosphate, Dibasic, Anhydrous
USP
Strawberry Flavoring (^) NA Flavor
Water USP N/A NA NA = not applicable *Strawberry flavor contains % propylene glycol; specific amounts of the remaining ingredients are proprietary information. Source: Module 3.2.P.1.2 Table P.1.2-
2.3 General Clinical Pharmacology
2.3.1 What are simvastatin’s clinical pharmacokinetic (PK) characteristics?
The following is extracted from Neuvonen P et al. Clin Pharmacokinet 2008;47:565463-74.
(b) (4) (b) (4)
(b) (4) (b) (4)
(b) (4)
(b) (4)
(b) (4) (b) (4)
(b) (4) (b) (4)
(b) (4)
(b) (4)
validated bioanalytical method. Figure 2 shows the schematic of Study PRG-NY-14-010.
Figure 2. Schematic of Study PRG-NY-14-010.
The sponsor prospectively designed Study PRG-NY-14-010 via the reference scaled bioequivalence
approach. If the 90% confidence intervals (CIs) of the ratio estimates for Cmax, AUC0-t, and AUC 0 -∞
were within 80.00 to 125.00%, then the Test treatment would be concluded as bioequivalent to
the Reference treatment.
For any log-transformed pharmacokinetic parameter, where the within-subject variability of the
Reference product ( σWR) was at least 0.294, bioequivalence was to be evaluated via the Scaled
Average Bioequivalence approach. Through this approach, the 95% upper confidence bounds of
the Reference-scaled criterion were computed.
Scaled Average Bioequivalence for the log-transformed pharmacokinetic parameters was evaluated via
testing the following null hypothesis:
H0: (μT- μR)
2
2
WR >^ θ
Versus the alternative hypothesis
H1: (μT- μR) 2 / σ^2 WR ≤ θ
where μT and μR were the averages of the log-transformed pharmacokinetic parameters Cmax, AUC0-t,
and AUC 0 -∞ for the Test and Reference products, respectively; θ was the Scaled Average Bioequivalence
limit which was calculated via the following formula:
= (ln Δ)^2 /^2 WO
Where Δ was 1.25, the usual average BE upper limit for t he untransformed Test/Reference ratio of
geometric means, and σW0=0.25.
If the following 2 conditions were satisfied, then the Test Product would be considered bioequivalent to
the Reference Product for the parameter:
The 95% upper confidence bound for (μT- μR) 2 / σ^2 WR ≤ θ, or equivalently, the 95% upper
confidence bound for (μT- μR)
2
2
WR ≤^ 0.
The point estimate of the Test/Reference geometric mean ratio falls within 80.00% to
Figure 3. Mean plasma simvastatin concentration-time profiles for the simvastatin suspension (test, T)
and simvastatin tablet (reference, R).
Source: Study PRG-NY-14-010 study report Figure 14.2.1.
Figure 4. Mean plasma simvastatin acid concentration-time profiles for the simvastatin suspension (test,
T) and simvastatin tablet (reference, R).
Source: Study PRG-NY-14-010 study report Figure 14.2.1.
Table 5. Statistical analysis of simvastatin pharmacokinetic parameters of 80 mg simvastatin suspension
(test) to 80 mg simvastatin tablet (reference).
Least Squares Geometric PK Parameter Means of Treatment: Test (T) N=
Reference (R) N=
Ratio (%)
Intra- subject %CV
90% CI of Ratio
Cmax (ng/mL) 38.8401 45.2347 85.86 37.14 ( 75.97 , 97.05 )
AUC0-t (ng hr/mL) 189.5880^ 210.5749^ 90.03^ 27.79^ (82.05 , 98.79^ )
AUC0-∞ (ng hr/mL) 195.1368 218.9752 89.11 28.13 (81.13 , 97.89)
Source: Study PRG-NY-14-010 study report Table 11.4-
Table 6. Reference scaled approach to assess bioequivalence of simvastatin between 80 mg simvastatin
suspension (test) and 80 mg simvastatin tablet (reference).
Parameters (Simvastatin)
Reference Variability(swr) 95% Upper Bound
Cmax (ng/mL) 0.3684899 -0.
Source: Study PRG-NY-14-010 study report Table 11.4-
Table 7. Statistical analysis of simvastatin acid pharmacokinetic parameters of 80 mg simvastatin
suspension (test) to 80 mg simvastatin tablet (reference).
Least Squares Geometric PK Parameter Means of Treatment: Test (T) N=
Reference (R) N=
Ratio (%)
Intra- subject %CV
90% CI of Ratio
Cmax (ng/mL) 8.6543 6.9238 124.99 30.33 ( 112.98 , 138.28 )
AUC0-t (ng hr/mL) 81.2358 75.1157 108.15 27.13 (98.76 , 118.42 )
AUC0-∞ (ng hr/mL) 83.4556 79.7169 104.69 27.86 (95.38 , 114.91)
Source: Study PRG-NY-14-010 study report Table 11.4-
Table 8. Reference scaled approach to assess bioequivalence of simvastatin acid between 80 mg
simvastatin suspension (test) and 80 mg simvastatin tablet (reference).
Parameters
(Simvastatin Acid)
Reference Variability (swr) 95% Upper Bound
Cmax (ng/mL) 0.3009861 0.
Source: Study PRG-NY-14-010 study report Table 11.4-
The sponsor stated the following for the test and reference treatments:
“There are no differences between the formulation of the submission batches, clinical batch, and
proposed commercial formulation.” (Page 28 of 82 in the Drug Product Summary (Section 2.3.P)).
“The submission batches were manufactured at full scale-up (commercial) size. All process
parameters used for the submission batches are the same as those proposed for use in commercial
production.” (Product Quality Summary, Section 2.3.P, Page 35 of 82).
The sponsor confirmed on the February 26, 2016 that the simvastatin tablet lot number J
used in Study PRG-NY-14-010 is the same product approved in the United States and marketed as
80 mg Zocor® tablets under Merck’s NDA 19-766.
Study PRG-NY-14-010’s report (Page 30/589) states that “The sponsor supplied the investigational
products. These materials were placed in the control of a qualified pharmacist at for receipt,
storage, dispensing as per the randomization schedule created by biostatistician using SAS® 9.
Enterprise Guide 4.2, and for subsequent retention after completion of the study, along with necessary
documents for the purpose.” Study PRG-NY-14-010’s report also cites the sponsor’s SOP No:22/81for
the receipt, storage, dispensing retention and dispatch of investigational products as well as the web
address for the reference of 21CFR320.38 and 21CFR320.63 for the retention of
bioavailability/bioequivalence samples.
Reviewer’s Comments
NDA 206-679 does not have an associated IND submission. However, the Division of Metabolism and
Endocrinology Products (DMEP) granted the sponsor’s pre-NDA submission meeting request (February
24, 2014) via correspondence. The meeting package contained the bioequivalence study protocol PRG-
NY-14-010. OND QA Biopharmaceutics group reviewed Protocol PRG-NY-14-010 because OND QA
Biopharmaceutics group reviewed bioequivalence studies and protocols at that time period. See meeting
minutes dated March 21, 2014 in DARRTS.
The sponsor prospectively used reference scaled bioequivalence approach to assess bioequivalence
between simvastatin suspension (test) and simvastatin tablet (reference) in the pivotal bioequivalence
study. The Office of Clinical Pharmacology previously used the regular 2 one-sided tests procedure to
assess simvastatin containing fixed dose combination tablets (Vytorin [NDA 21-687], Simcor [NDA 22-
078], and Juvisync [NDA 202-343]). The Office of Generic Drugs published product specific guidances
for simvastatin tablets and simvastatin orally disintegrating tablets. These guidances recommend the use
of the regular 2 one-sided tests procedure to assess simvastatin bioequivalence, whereas the reference
scaled bioequivalence approach is used to assess bioequivalence of generic drugs such as progesterone.
This reviewer’s statistical analyses results are consistent with the sponsor’s analyses. This reviewer used
the SAS codes for reference scaled bioequivalence approach recommended by the “Draft Guidance on
Progesterone” to assess the bioequivalence between simvastatin suspension and simvastatin tablet
(http://www fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm209294.pdf). This
reviewer observed only slight differences after the decimal point for the following:
estimated GMR ratios and 90% CI for simvastatin Cmax, AUC0-t, and AUC0- (Table 5)
Reference Variability (swr) and 95% Upper Bound for simvastatin Cmax (Table 6)
estimated GMR ratios and 90% CI for simvastatin acid Cmax, AUC0-t, and AUC0- (Table 7)
Reference Variability (swr) and 95% Upper Bound for simvastatin acid Cmax (Table 8)
This reviewer’s estimated the Reference Variability (swr) for simvastatin AUC0-t and AUC0- is
0.2743289733 and 0.2721163008, respectively. Because these estimated values are less than 0.294, the 2
one-sided tests procedure to determine bioequivalence for simvastatin AUC0-t and AUC0- is valid as used
by the sponsor. Also, this reviewer’s estimated the Reference Variability (swr) for simvastatin acid
AUC0-t and AUC0- is 0.2617861203 and 0.2609779863, respectively. Because these estimated values
are less than 0.294, the 2 one-sided tests procedure to determine bioequivalence for simvastatin acid
AUC0-t and AUC0- is valid as used by the sponsor.
Because the 95% upper bound of simvastatin Cmax is -0.023961 ( 0) and the ratio of test/reference
geometric mean ratio is within 80 – 125% (85.86%) as well as the 90% confidence intervals for
simvastatin AUC0-t and AUC0- are within 80 – 125%, the test simvastatin suspension is bioequivalent to
the reference 80 mg Zocor tablets under fasting.
(b) (4) (b) (4)
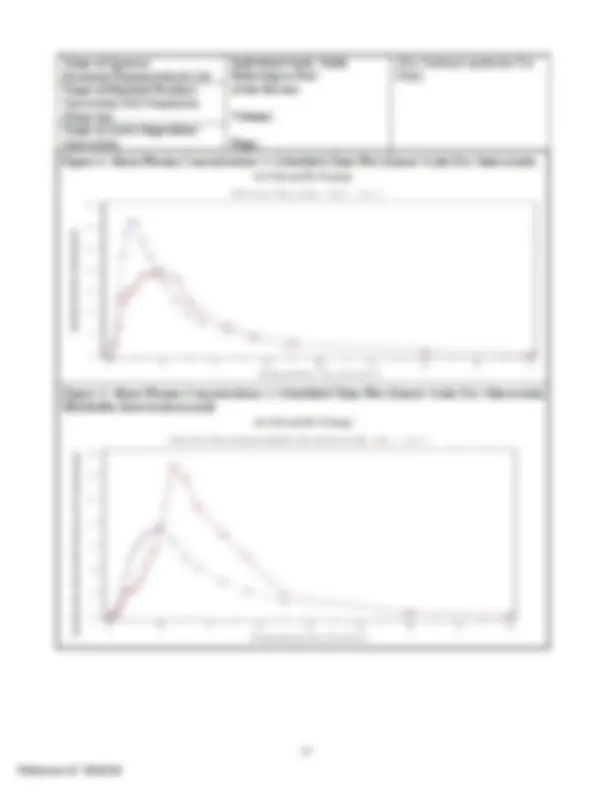
Figure 6. Mean plasma simvastatin concentration-time profiles for 80 mg simvastatin suspension under
fed (A) and fasting (B) conditions.
Source: Study PRG-NY-14-011 study report Figure 14.2.1.
Figure 7. Mean plasma simvastatin acid concentration-time profiles for 80 mg simvastatin suspension
under fed (A) and fasting (B) conditions.
Source: Study PRG-NY-14-011 Figure 14.2.1.
Table 9. Simvastatin pharmacokinetic parameters of 80 mg simvastatin suspension under fed and fasting
conditions.
Summary Simvastatin Statistics Cmax (ng/mL)
AUC0-t (ng hr/mL)
AUC0-∞
(ng.hr/mL)
Tmax (Hour)
t1/ (Hour)
Kel (1/hr)
AUC_Ratio (%) Test Treatment (Fed state): (N=52) Mean (SD)* 26. (14.5492)
GM 23.522 130.802 133.676 3.10 4.406 0.157 97.
(Min, Max) (6.154, 64.438)
%CV 54.01 54.73 53.91 47.25 31.36 40.87 1.
Reference Treatment (Fasting state): (N=52) Mean (SD)* 38. (26.0720)
(133.3935) 1.^
GM 32.003 155.686 161.484 1.69 6.076 0.114 96.
(Min, Max) (7.863, 115.369)
%CV 67.07 68.58 67.84 43.94 33.54 36.48 2.
Source: Modified from Study PRG-NY-14-011 study report Table 11.4-1 (A)
Table 10. Simvastatin acid pharmacokinetic parameters of 80 mg simvastatin suspension under fed and
fasting conditions.
Simvastatin Metabolite (beta-hydroxyacid) Summary Statistics Cmax (ng/mL)
AUC0-t (ng hr/mL)
AUC0-∞
(ng.hr/mL)
Tmax (Hour)
t1/ (Hour)
Kel (1/hr)
AUC_Ratio (%) Test Treatment (Fed state): (N=52) Mean (SD)* 14. (7.7785)
GM 12.723 84.997 86.099 5.71 3.800 0.182 98.
(Min, Max) (3.446, 39.777)
%CV 53.28 52.92 53.01 19.89 32.73 36.24 1.
Reference Treatment (Fasting state): (N=52) Mean (SD)* 8. (5.1502)
(39.1279) 4.^
GM 7.337 56.877 59.774 3.46 5.804 0.119 95.
(Min, Max) (1.560, 32.143)
%CV 60.63 56.08 56.98 32.45 53.82 46.50 5.
Source: Modified from Study PRG-NY-14-011 study report Table 11.4-1 (B)
Table 11. Statistical analysis of simvastatin pharmacokinetic parameters of 80 mg simvastatin suspension
under fed (test) and fasting (reference) conditions (N=52).
PK Parameter
Least Squares Geometric Means of Treatment: Ratio (%)
Intra- subject %CV
90% CI of Test Ratio Treatment (Fed State)
Reference Treatment (Fasting State)
Cmax (ng/mL) 23.4610 31.8528 73.65 45.16 ( 63.92 , 84.87 )
AUC0-t (ng hr/mL) 130.4119 155.6543 83.78 27.18 ( 76.74 , 91.47 )
AUC0-∞ (ng.hr/mL) 133.2920 161.4601 82.55 27.05 ( 75.65 , 90.09 )
Source: Study PRG-NY-14-011 study report Table 11.4-3 (A)
13
Because the significant effect of food on the exposure of simvastatin suspension cannot be related
to that of the label for the reference listed product and simvastatin suspension is a new dosage
form, Option 1 may not be appropriate.
Even though the simvastatin suspension is a new dosage form but on its own merit, Option 3 may
not be appropriate because:
o Niacin increases simvastatin Cmax and AUC 8 and 40%, respectively, as well as increases
simvastatin acid Cmax and AUC 84 and 60%, respectively, without the need to adjust the
dose of simvastatin per the Zocor label. Also, fenofibrate decreases simvastatin Cmax and
AUC 17 and 11%, respectively, as well as decreases simvastatin acid Cmax and AUC 11
and 36%, respectively, without the need to adjust the dose of simvastatin per the Zocor
label.
o The Zocor label has cautionary statement on dosing simvastatin and niacin specific to
Chinese. However, this caution for Chinese patients is not due to the pharmacokinetic
interaction between niacin and simvastatin. Non-Chinese patients do not have restriction
to use this combination of simvastatin and niacin. This cautionary restriction is due to the
outcome trial which the increase in myopathy in Chinese was observed; the Zocor label
also indicates that it is unknown if the risk applies to other patients.
Thus, Option 2 seems to be the most appropriate recommendation for this submission.
2.4 Bioanalytical
Are the bioanalytical methods properly validated to measure simvastatin and simvastatin acid in
plasma samples?
The sponsor used a liquid chromatography with tandem mass spectrometry (LC/MS/MS) assay to
determine the simvastatin and simvastatin acid concentrations in plasma samples. Table 15 details the
validation of the bioanalytical assay.
Table 15. Validation of the bioanalytical assay to measure simvastatin and simvastatin acid in plasma
samples for Studies PRG-NY-14-010 and PRG-NY-14-011.
Analyte Simvastatin Simvastatin Acid
Matrix Plasma Plasma
Anticoagulant K 2 EDTA K 2 EDTA
Sample volume, mL 0.3 0.
Lower limit of quantitation, ng/mL 0.2 0.
Linear range, ng/mL 0.2 – 50.01 0.051 – 15.
Average recovery (%) 86.22 77.
Assay precision (%CV of QC samples)
Inter-batch 4.36 – 7.17 3.6 – 13.
Intra-batch 0.27 – 10.19 0.84 – 17.
Assay accuracy (% bias of QC samples)
Inter-batch 91.99 – 97.57 96.23 – 107.
Intra-batch 88.05 – 101.73 91.71 – 117.
Bench-top stability (9 hrs.), % 102.02 – 110.98 106.25 – 108.
Freeze-thaw stability (3 cycles), % 103.43 – 110.46 106.58 – 108.
Source: This reviewer’s compilation of the sponsor’s Bioanalytical and Validation Reports for Studies PRG-NY-14-010 and PRG-NY-14-
Validations for the LC/MS/MS bioanalytical assay of simvastatin and simvastatin acid appear acceptable
with reasonable precision and accuracy.
3. Label Recommendations
Study No.: 12192/13-14; Protocol No.: /086/13- Version No.: 01
Date: 10 Apr 2014 Confidential
Name of Sponsor:
Rosemont Pharmaceuticals Ltd.
Individual Study Table
Referring to Part
of the Dossier
Volume:
Page:
(For National Authority Use
Only)
Name of Finished Product:
Simvastatin Oral Suspension
40mg/5mL
Name of Active Ingredient:
Simvastatin
Methodology:
All study related procedures, restrictions, duration, dates and timings, information on the study
formulation and confidentiality of participant data were explained clearly to the volunteers by clinical
personnel at the time of obtaining informed consent and also the process of informed consent was
video recorded. Volunteers who signed the consent form and showed their willingness to participate
in the study were enrolled. Volunteers who satisfied the inclusion and exclusion criteria and were
found to be healthy on physical examination with laboratory investigation values within reference
limits were considered eligible to be admitted into the study. Volunteers whose pre-study laboratory
values were outside the reference range were considered for participation provided these values were
considered clinically non-significant by the Medical Investigator. The eligible volunteers reported to
the study site for Period I on 28 Dec 2013, between 09:30 hours to 10:41 hours, for Period II on 07
Jan 2014, between 11:45 hours to 19:59 hours (participant 19 checked in to the facility at 21:57 hrs
and was withdrawn from the study due to protocol non-compliance) and for Period III on 17 Jan 2014,
between 11:57 hours to 19:28 hours.
Study Participants and Study Activities:
Study participants were served dinner at 20:00 to 20:31 hours at check-in to ensure a minimum of
10.0 hours fasting prior to dose administration. On the day of dosing in each period, a single dose of
either the Test or Reference product was administered with 240 mL of room temperature drinking
water. Dosing was conducted as per the randomization schedule in each period under fasting
conditions. Following dosing in each period, a total of 20 blood samples were collected over 19 time
points from 0-32 hours post-dose. Study participants were discharged from the clinical pharmacology
unit (CPU) at 36 hours post-dose. A washout period of at least 07 days was observed between the
periods. Study restrictions with respect to fluid intake and physical activity were implemented
throughout their stay in the CPU.
Number of Study Participants Planned:
The planned sample size was 42.
Number of Study Participants Analyzed:
Plasma samples from 38 participants (excluding participants 12, 19, 21 & 41) were analyzed and
pharmacokinetic analysis was performed on this data. Reference-Scaled Average Bioequivalence
results were based on the data from the 36 participants who completed all three periods (excluding
participants 05, 12, 19, 21, 29 & 41). Reference variability (swr) calculations were based on data from
38 subjects (excluding participants 12, 19, 21 & 41) who received the Reference drug in at least two
periods.
Participants were withdrawn / excluded from the analyses above due to adverse events or non-
compliance to protocol requirements.
(b) (4)