Download Alcohol and Medication Interactions and more Exercises Medicine in PDF only on Docsity!
Alcohol and Medication
Interactions
Ron Weathermon, Pharm.D., and David W. Crabb, M.D.
Many medications can interact with alcohol, thereby altering the metabolism or effects of alcohol and/or the medication. Some of these interactions can occur even at moderate drinking levels and result in adverse health effects for the drinker. Two types of alcohol- medication interactions exist: (1) pharmacokinetic interactions, in which alcohol interferes with the metabolism of the medication, and (2) pharmacodynamic interactions, in which alcohol enhances the effects of the medication, particularly in the central nervous system (e.g., sedation). Pharmacokinetic interactions generally occur in the liver, where both alcohol and many medications are metabolized, frequently by the same enzymes. Numerous classes of prescription medications can interact with alcohol, including antibiotics, antidepressants, antihistamines, barbiturates, benzodiazepines, histamine H 2 receptor antagonists, muscle relaxants, nonnarcotic pain medications and anti-inflammatory agents, opioids, and warfarin. In addition, many over-the-counter and herbal medications can cause negative effects when taken with alcohol. K EY W ORDS : moderate AOD use; prescription drug; adverse drug interaction; drug metabolism; ethanol metabolism; cytochromes; liver; alcohol dehydrogenases; antibiotics; antidepressants; histamine H1 receptor blockaders; barbiturates; benzodiazepines; histamine H2 receptor blockaders; anti-inflammatory agents; opioids; warfarin; over-the-counter drug; literature review
M
ost people who consume alcohol, whether in moderate or large quantities, also take medications, at least occasionally. As a result, many people ingest alcohol while a medication is present in their body or vice versa. A large number of medications—both those available only by prescription and those avail- able over the counter (OTC)—have the potential to interact with alcohol. Those interactions can alter the meta- bolism or activity of the medication and/or alcohol metabolism, resulting
in potentially serious medical consequences. For example, the sedative effects of both alcohol and sedative medications can enhance each other (i.e., the effects are addi- tive), thereby seriously impairing a person’s ability to drive or operate other types of machinery. Most studies assessing alcohol- medication interactions focus on the effects of chronic heavy drinking. Relatively limited information is avail- able, however, on medication interac- tions resulting from moderate alcohol consumption (i.e., one or two standard drinks 1 per day). Researchers, physi- cians, and pharmacists must therefore infer potential medication interactions at moderate drinking levels based on
observations made with heavy drinkers. In addition, moderate alcohol consump- tion may directly influence some of the disease states for which medications are taken (see sidebar, pp. 52–53, for further discussion of alcohol’s influ- ences on various disease states). This
40 Alcohol Research & Health
R ON WEATHERMON , PHARM.D., is an assistant professor at the School of Pharmacy and Pharmaceutical Sciences, Purdue University, Indianapolis, Indiana.
DAVID W. CRABB , M.D., is a professor in the Departments of Medicine and Biochemistry and Molecular Biology, Indiana University School of Medicine, Indianapolis, Indiana.
(^1) A standard drink is defined as one 12-ounce can of beer or bottle of wine cooler, one 5-ounce glass of wine, or 1.5 ounces of distilled spirits and is equivalent to approximately 0.5 ounce, or 12 grams (g), of pure alcohol.
article discusses alcohol absorption, distribution, and metabolism within the body; the sites where potential alcohol-medication interactions can occur; and possible adverse effects from various alcohol-medication combinations, including OTC or herbal products.
Alcohol Absorption, Distribution, and Metabolism
Gastrointestinal Absorption and Metabolism
When alcohol is ingested through the mouth, a small amount is immediately broken down (i.e., metabolized) in the stomach. Most of the remaining alcohol is then absorbed into the bloodstream
from the gastrointestinal tract, primar- ily the stomach and the upper small intestine. Alcohol absorption occurs slowly from the stomach but rapidly from the upper small intestine. Once absorbed, the alcohol is transported to the liver through the portal vein. A portion of the ingested alcohol is metabolized during its initial passage through the liver; the remainder of the ingested alcohol leaves the liver, enters the general (i.e., systemic) cir- culation, and is distributed through- out the body’s tissues. Alcohol metabolism (or the meta- bolism of any other substance) that occurs in the gastrointestinal tract and during the substance’s initial passage through the liver is called “first-pass metabolism” (see figure 1). For exam- ple, the mucosa lining the stomach contains enzymes that can metabolize
alcohol as well as other substances; some of those enzymes, including alcohol dehydrogenase (ADH) and cytochrome P450 are described in more detail in the section “Alcohol Metabolism in the Liver.” The contribution of stomach (i.e., gastric) enzymes to first-pass alcohol metabolism, however, is controversial. Whereas some researchers have pro- posed that gastric enzymes play a major role in first-pass metabolism (Lim et al. 1993), other investigators consider the liver to be the primary site of first- pass metabolism (Levitt and Levitt 1998). Furthermore, some gender dif- ferences appear to exist in the overall extent of, and in the contribution of, gastric enzymes to first-pass meta- bolism. For example, the extent of first-pass metabolism is less in women than in men and some studies also
What Is Moderate Drinking?
Vol. 23, No. 1, 1999 41
Alcohol and Medication Interactions
Figure 1 Schematic representation of first-pass metabolism. (A) Alcohol ingested through the mouth reaches the stomach, where a portion is metabolized by the enzyme alcohol dehydrogenase (ADH). The remaining alcohol enters the intestine, where most of the remainder is absorbed into the bloodstream and enters the portal vein that leads to the liver. In the liver, part of the alcohol is metabolized by ADH or cytochrome P450. The remaining alcohol enters the general (i.e., systemic) circulation and eventually is transported back to the liver and metabolized there. The metabolism of alcohol in the stomach or during the first passage through the liver after absorption from the intestine is called first-pass metabolism. (B) Changes in blood alcohol levels (BALs) after oral alcohol ingestion and after intravenous administration of the same alcohol dose. The difference in BALs achieved with both administration routes (i.e., the amount by which the BAL is lower after oral ingestion) represents that portion of the ingested alcohol that has been broken down by first-pass metabolism before reaching the systemic circulation.
Hepatic metabolism of alcohol (possibly blocked by some medications)
Stomach
Increased gastric emptying (stimulated or inhibited by some medications)
Alcohol absorption into bloodstream
Portal Vein
Transgastric metabolism (possibly blocked by some medications)
Alcohol to systemic circulation
Liver
Alcohol
0
10
20
30
40
50
1 2 3 4 Hours
BAL (mg %)
Intravenous alcohol
Oral alcohol
Intestine
Panel A Panel B
aldehyde dehydrogenase (ALDH). (The function of ALDH is discussed in more detail in the following sec- tion.) Several ADH variants (i.e., isozymes) exist, which differ in their activity when studied in the labora- tory. In humans, however, the effect of different ADH isozymes on alcohol elimination is small (Thomasson 1995). Although different ADH variants are associated with different risks of devel- oping alcoholism, no studies to date have researched the effects of these isozymes on a person’s susceptibility to alcohol-medication interactions. In contrast to ADH, the alcohol- metabolizing enzyme cytochrome P450—also called microsomal ethanol oxidizing system (MEOS) (Lieber 1994)—plays a central role in alcohol-medication interactions. Cytochrome P450 actually is a system consisting of two enzymes, one called cytochrome P450 reductase and another one called CYP2E1, which
are both embedded in the membrane of a cell component called the endoplas- mic reticulum.^3 In addition to alcohol, CYP2E1 can metabolize numerous compounds, including acetaldehyde, the pain medication acetaminophen, the antibiotic isoniazid, and the barbiturate phenobarbital. Accordingly, CYP2E plays an important role in many alco- hol-medication interactions. In people consuming alcohol only occasionally, CYP2E1 metabolizes only a small fraction of the ingested alcohol. Chronic heavy drinking, however, can increase CYP2E1 activ- ity up to tenfold, resulting in a sub- stantial increase in the proportion of alcohol that is metabolized by this enzyme rather than by ADH (figure
- (Lieber 1994). The effect of lower levels of alcohol consumption on CYP2E1 activity is unknown. Because CYP2E1 also metabolizes several medi- cations, alcoholics, in whom CYP2E activity is enhanced, exhibit increased metabolic rates for those medications when they are sober. When those alcoholics are intoxicated, however, the alcohol in their system competes with the medication for metabolism by CYP2E1. As a result, the break- down of the medication is slowed. With many medications, increased or decreased metabolic rates can have adverse or even fatal consequences. With increased metabolic rates, the medication’s concentration in the body may be too low or may decline too fast for it to be effective. Con- versely, decreased metabolic rates may result in the accumulation of higher drug concentrations over longer periods of times, which may result in harmful overdoses.
What Is Moderate Drinking?
Vol. 23, No. 1, 1999 43
Alcohol and Medication Interactions
(A) In the absence of alcohol, CYP activity is relatively low. CYP breaks down the medication, and the resulting products (i.e., metabolites) are excreted.
(B) After moderate alcohol consumption, CYP metabo- lizes alcohol in addition to the medication. As a result of competition for CYP between alcohol and the medication, the medication’s metabolism is reduced, and the production of metabolites as well as their excretion declines, resulting in higher medi- cation levels in the body. In addition, interactions between alcohol and the medication may occur in the central nervous system (CNS).
(C) In chronic heavy drinkers who are sober, CYP activity is enhanced. As a result, the breakdown of medications metabolized by CYP increases, and metabolite levels as well as their excretion are elevated, possibly resulting in insufficient medication levels in the body. Furthermore, toxic metabolites may accumulate.
(D) In chronic heavy drinkers who are intoxicated, CYP is activated, but most of the enzyme is involved in alcohol metabolism. Consequently, the CYP-dependent metabolism of other medications is reduced, and metabolite levels and their excretion decline. Alcohol- medication interactions also can occur in the CNS.
Figure 3 Potential alcohol-medication interactions involving cytochrome P450 enzymes (CYP) in the liver.
CYP
Drug Drug metabolite Excretion
Interaction with alcohol in CNS
Drug Drug metabolite ( )^ Excretion ( )
Alcohol
Drug Drug metabolite ( )^ Excretion ( )
Drug metabolite toxicity
CYP
CYP
Interaction with alcohol in CNS
Drug Drug metabolite ( )^ Excretion ( )
Alcohol
CYP
(^3) The endoplasmic reticulum is an extensive net- work of membrane-enclosed tubules within the cell that is involved in the production of proteins and fat molecules and in the transport of those molecules within the cell.
Wide variation exists among people in both CYP2E1 activity and metabolic rates for medications broken down by this enzyme (e.g., acetaminophen and chlorzoxasone, a medication used to relieve muscle pain). Some of this vari- ation may be genetically determined, although the specific underlying mecha- nism is unknown (Carriere et al. 1996). A person’s CYP2E1 activity level, however, could influence his or her susceptibility to alcohol-medication interactions involving this enzyme. For example, in a person with innately low metabolic rates, a further decrease in metabolism when alcohol is consumed would affect medication levels (and thus the potential for adverse effects or interactions with alcohol) to a greater extent than in a person with innately high metabolic rates. In addition to CYP2E1, at least two other cytochrome enzymes that metabolize various medications (i.e., CYP3A4 and CYP1A2) also can break down alcohol (Salmela et al. 1998). Moreover, the amounts of var- ious enyzmes of the cytochrome CYP3A family (including CYP3A4) can increase from alcohol consump- tion (Niemela et al. 1998). Thus, potential interactions also exist between alcohol and medications metabolized by these cytochromes.
Acetaldehyde Metabolism in the Liver
As mentioned in the previous section, alcohol breakdown by ADH generates acetaldehyde, which, in turn, is metab- olized further by ALDH. Two major types of ALDH (i.e., ALDH1 and ALDH2) exist, which are located in different regions of the cell. ALDH requires relatively high acetaldehyde concentrations in the cell to be active, whereas ALDH2 is active at extremely low acetaldehyde levels. Accordingly, ALDH2 may play a particularly impor- tant role in acetaldehyde breakdown after moderate alcohol consumption. The significance of ALDH2 activity in alcohol and acetaldehyde metabolism is further supported by an inborn variation in alcohol metabolism that occurs primarily in people of Asian heritage but which is rare among
Caucasians. After consuming alcohol, many Asian people experience an unpleasant “flushing” reaction that can include facial flushing, nausea, and vomiting. These symptoms are caused by acetaldehyde accumulation in the body. Thus, following alcohol consumption, acetaldehyde levels in people susceptible to the flushing reaction may be 10 to 20 times higher than in people who do not experience flushing. Researchers have noted that approximately 40 percent of Asians lack ALDH2 activity because they have inherited one or two copies of an inactive variant of the gene that produces ALDH2 (Goedde et al. 1989). Most of these individuals flush
when they consume alcohol. These observations imply that ALDH plays a crucial role in maintaining low acetaldehyde levels during alcohol metabolism. Consequently, even inad- vertent alcohol administration to peo- ple of Asian heritage (who may have inherited an inactive ALDH2 gene) can cause unpleasant reactions. Thus, the potential flushing response should be an important concern for physi- cians and patients, because many prescription and OTC medications contain substantial amounts of alco- hol (see table 1). Physicians and phar- macists therefore must be alert to the possibility that Asian patients may be intolerant of these medications.
44 Alcohol Research & Health
Table 1 Alcohol Content of Prescription and Over-the-Counter Medications
Product Alcohol Content (%)
Betadine (mouthwash, gargle) 8. Cepacol (mouthwash, gargle) 14. Cheracol Sore Throat 12. Chlortrimeton syrup 7. Cimetidine Oral Solution 2. Cyclosporine Oral Solution 9.5–12. Cyproheptadine 5. DentSure (denture rinse, peppermint) 14. Dr. Tichenor’s Antiseptic 70* Digoxin Elixir 10. Entex 5. Furosemide Liquid 11. Intensol (diazepam) 19. Listerine 26. Listerine Cool Mint or Freshburst 21. Lomotil Liquid 15. Mellaril/Thioridiazine 3.0–4. Mentadent Mouthwash 10. Oral-B Anti-Plaque Rinse 8. Plax-Advanced Formula 8. Peri-colace 10. Phenobarbital Elixir 14. Promethazine/Phenergan 7. Ranitidine 7. Scope, Baking Soda 9. Scope, Cool Peppermint 14. Senokot Syrup 7. Targon Smokers’ Mouth Wash, Clean Taste 15.6* Targon Smokers’ Mouth Wash, Original 16.0* Tavist Oral Solution 5. Theophylline Elixir 20. Viadent Oral Rinse 10.
*Specifically denatured alcohol (SDA) 38B content. SOURCE: Knodel, L.C., ed. Nonprescription Products: Formulations and Features. 1998–1999. Washington, DC: American Pharmaceutical Association, 1999.
46 Alcohol Research & Health
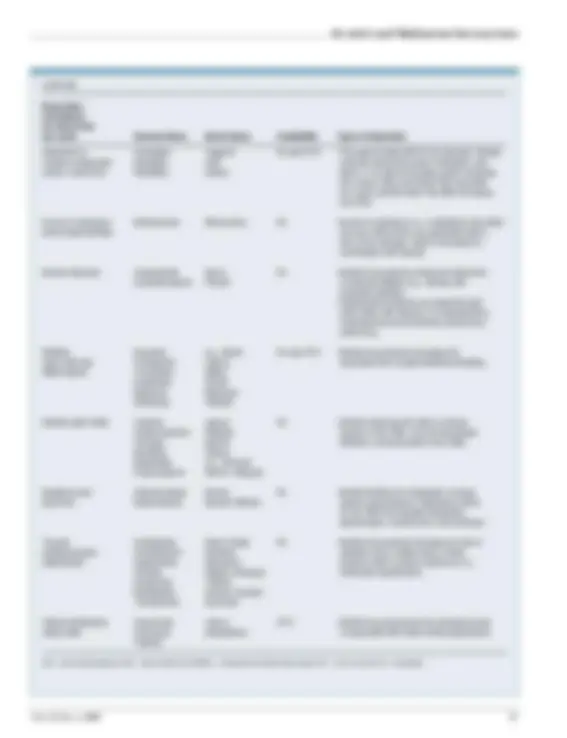
Table 3 Interactions Between Alcohol and Various Classes of Medications
Drug Class (Conditions for which they are used) Generic Name Brand Name Availability Type of Interaction Analgesics Aspirin various Rx and OTC • Aspirin increases gastric emptying, leading to (pain relief) Acetaminophen e.g., Tylenol faster alcohol absorption in the small intestine; may also inhibit gastric ADH.
- Alcohol enhances acetaminophen metabolism into a toxic product, potentially causing liver damage.
Antibiotics Erythromycin various Rx • Erythromycin may increase gastric emptying, (microbial infections) Isoniazid Nydrazid, leading to faster alcohol absorption in the Rifamate, Rifater small intestine.
- Alcohol increases the risk of isoniazid-related liver disease.
Anticonvulsants Phenytoin Dilantin Rx • Chronic alcohol consumption induces (seizure disorders) phenytoin breakdown.
Antihistamines Diphenhydramine e.g., Benadryl Rx and OTC • Alcohol enhances the effects of these agents (allergies, colds) Chlorpheniramine various on the central nervous system (CNS), such as Clemastine drowsiness, sedation, and decreased motor skills. Hydroxyzine Atarax, Vistaril • The interactions are more pronounced in Promethazine Phenergan elderly people. Cyproheptadine Periactin • No documented interactions exist with nonsedating antihistamines (i.e., certrizine, hismanal, loratidine).
Anticoagulants Warfarin Coumadin Rx • Acute alcohol intake may increase anticoagulation (prevention of blood clots) by decreasing warfarin metabolism; chronic alcohol ingestion decreases anticoagulation by increasing warfarin metabolism.
Antidiabetic agents Chlorpropamide Diabinese Rx • Alcohol consumption by diabetic patients taking (blood sugar Glipizide Glucotrol these medications increases the risk of lower- regulation) Glyburide DiaBeta, Glynase, than-normal blood sugar levels (i.e., hypoglycemia). Micronase • Chlorpropamide, glyburide, and tolbutamide can Tolbutamide Orinase cause disulfiram-like interactions after alcohol Metformin Glucophage ingestion.
- Metformin may cause increased levels of lactic acid in the blood after alcohol consumption.
Barbiturates Phenobarbital various Rx • Chronic alcohol intake increases barbiturate (anesthesia, pain relief) metabolism by cytochrome P450.
- Alcohol enhances the sedative and hypnotic effects on the CNS.
Benzodiazepines Alprazolam Xanax Rx • Alcohol enhances the effects of these agents (sedative agents) Chlordiazepoxide Librium on the CNS, such as drowsiness, sedation, and Clonazepam Klonopin decreased motor skills. Clorazepate Tranxene Diazepam Valium Lorazepam Ativan Midazolam Versed Oxazepam Serax Temazepam Restoril Triazolam Halcion
What Is Moderate Drinking?
Vol. 23, No. 1, 1999 47
Alcohol and Medication Interactions
continued
Drug Class (Conditions for which they are used) Generic Name Brand Name Availability Type of Interaction Histamine H 2 Cimetidine Tagamet Rx and OTC • The agents inhibit ADH in the stomach, thereby receptor antagonists Nizatidine Axid reducing alcohol first-pass metabolism (see (ulcers, heart burn) Ranitidine Zantac figure 1), as well as increase gastric emptying. As a result, BALs are higher than expected for a given alcohol dose; this effect increases over time.
Immune modulators Methotrexate Rheumatrex Rx • Immune modulators (i.e., medications that affect (rheumatoid arthritis) immune cell function) are associated with a risk of liver damage, which is increased in combination with alcohol.
Muscle relaxants Carisoprodol Soma Rx • Alcohol consumption enhances impairment Cyclobenzaprine Flexeril of physical abilities (e.g., driving) and increases sedation.
- Carisoprodol produces an opiate-like high when taken with alcohol; it is metabolized to meprobamate and sometimes abused as a street drug.
NSAIDs Ibuprofen e.g., Motrin Rx and OTC • Alcohol consumption increases the (pain relief and Flurbiprofen various associated risk of gastrointestinal bleeding. inflammation) Fenoprofen Nalfon Ketoprofen Orudis Naproxen Naprosyn Diclofenac Voltaren
Opioids (pain relief) Codeine various Rx • Alcohol enhances the effects of these Hydromorphone Dilaudid agents on the CNS, such as drowsiness, Fentanyl generic sedation, and decreased motor skills. Morphine various Meperidine e.g., Demerol Propoxyphene Darvon, Wygesic
Sedatives and Chloral hydrate Noctec Rx • Alcohol inhibits the metabolism of these hypnotics Meprobamate Equanil, Miltown agents and produces a depressant effect on the CNS that includes sleepiness, disorientation, incoherence, and confusion.
Tricyclic Amitriptyline Elavil, Endep Rx • Alcohol consumption increases the risk of antidepressants Clomipramine Anafranil sedation and a sudden drop in blood (depression) Desipramine Norpramin pressure when a person stands up (i.e., Doxepin Adapin, Sinequan orthostatic hypotension). Imipramine Tofranil Nortriptyline Aventyl, Pamelor Trimipramine Surmontil
Herbal medications Chamomile various OTC • Alcohol may accentuate the drowsiness that (sleep aids) Echinacea preparations is associated with these herbal preparations. Valerian
ADH = alcohol dehydrogenase; BAL = blood alcohol level; NSAIDs = nonsteroidal anti-inflammatory drugs; OTC = over the counter; Rx = prescription.
What Is Moderate Drinking?
Vol. 23, No. 1, 1999 49
Alcohol and Medication Interactions
phenelzine and tranylcypromine) can induce severe high blood pressure if they are consumed together with a substance called tyramine, which is present in red wine. Accordingly, peo- ple taking MAO inhibitors should be warned against drinking red wine. The atypical antidepressants (i.e., nefazodone and trazodone) may cause enhanced sedation when used with alcohol.
Antihistamines. These medications, which are available both by prescription and OTC, are used in the management of allergies and colds. Antihistamines may cause drowsiness, sedation, and low blood pressure (i.e., hypotension), especially in elderly patients (Dufour et al. 1992). Through pharmacody- namic interactions, alcohol can substan- tially enhance the sedating effects of these agents and may thereby increase, for example, a person’s risk of falling or impair his or her ability to drive or operate other types of machinery. As a result of these potential interactions, warning labels on OTC antihistamines caution patients about the possibility of increased drowsiness when consum- ing the medication with alcohol. Newer antihistamines (i.e., certrizine and loratidine) have been developed to minimize drowsiness and sedation while still providing effective allergy relief. However, these newer medica- tions may still be associated with an increased risk of hypotension and falls among the elderly, particularly when combined with alcohol. Consequently, patients taking nonsedating antihis- tamines still should be warned against using alcohol.
Barbiturates. These medications are sedative or sleep-inducing (i.e., hyp- notic) agents that are frequently used for anesthesia. Phenobarbital, which is probably the most commonly pre- scribed barbiturate in modern prac- tice, also is used in the treatment of seizure disorders. Phenobarbital acti- vates some of the same molecules in the CNS as does alcohol, resulting in pharmacodynamic interactions between the two substances. Consequently, alcohol consumption while taking phenobarbital synergistically enhances
the medication’s sedative side effects. Patients taking barbiturates therefore should be warned not to perform tasks that require alertness, such as driving or operating heavy machinery, particularly after simultaneous alcohol consumption. In addition to the pharmacodynamic interactions, pharmacokinetic interac- tions between alcohol and phenobar- bital exist, because alcohol inhibits the medication’s breakdown in the liver. This inhibition results in a slower meta- bolism and, possibly, higher blood
levels of phenobarbital. Conversely, barbiturates increase total cytochrome P450 activity in the liver and accelerate alcohol elimination from the blood (Bode et al. 1979). This acceleration of alcohol elimination probably does not have any adverse effect.
Benzodiazepines. Like barbiturates, benzodiazepines (BZDs) are classified as sedative-hypnotic agents and act through the same brain molecules as do barbiturates. Accordingly, as with bar- biturates, concurrent consumption of BZDs and moderate amounts of alcohol can cause synergistic sedative effects, leading to substantial CNS impairment. It is worth noting that both barbitu- rates and benzodiazepines can impair memory, as can alcohol. Consequently, the combination of these medications with alcohol would exacerbate this memory-impairing effect. In fact, this effect sometimes is exploited by mix- ing alcoholic beverages with BZDs, such as the rapid-acting flunitrazepam (Rohypnol®), an agent implicated in
date rape (Simmons and Cupp 1998). In addition, the metabolism of certain BZDs involves cytochrome P450, leading to the alcohol-induced changes in metabolism described earlier in this article.
Histamine H 2 Receptor Antagonists (H 2 RAs). As mentioned earlier in this article, H 2 RAs (e.g., cimetidine, rani- tidine, nizatidine, and famotidine), which reduce gastric acid secretion, are used in the treatment of ulcers and heartburn. These agents reduce ADH activity in the stomach mucosa (Caballeria et al. 1991), and cimeti- dine also may increase the rate of gas- tric emptying. As a result, alcohol consumed with cimetidine undergoes less first-pass metabolism, resulting in increased BALs. For example, in a study of people who consumed three or four standard drinks over 135 min- utes while taking cimetidine, BALs rose higher and remained elevated for a longer period of time than in people not taking cimetidine (Lieber 1997; Gupta et al. 1995). Not all H 2 RAs, however, exert the same effect on BALs when taken with alcohol. Thus, cime- tidine and ranitidine have the most pronounced effect, nizatidine has an intermediate effect, and famotidine appears to have no effect (i.e., appears not to interact with alcohol).^5 In addi- tion, because women generally appear to have lower first-pass metabolism of alcohol, they may be at less risk for adverse interactions with H 2 RAs.
Muscle Relaxants. Several muscle relax- ants (e.g., carisoprodol, cyclobenzaprine, and baclofen), when taken with alcohol, may produce a certain narcotic-like reaction that includes extreme weakness, dizziness, agitation, euphoria, and confusion. For example, carisoprodol is a commonly abused and readily available prescription medication that is sold as a street drug. Its metabolism in the liver generates an anxiety-reducing agent that was previously marketed as
(^5) Another class of medications, which prevent gastric acid production through a different mechanism from the H 2 RAs (i.e., omeprazole and lansoprazole), also do not appear to interact with alcohol.
Pharmacodynamic
interactions can
occur with
intermittent alcohol
consumption and
even after a single
episode of drinking.
a controlled substance (meprobamate). The mixture of carisoprodol with beer is popular among street abusers for creating a quick state of euphoria.
Nonnarcotic Pain Medications and Anti-Inflammatory Agents.
Many people frequently use nonnarcotic pain medications and anti-inflamma- tory agents (e.g., aspirin, acetaminophen, or ibuprofen) for headaches and other minor aches and pains. In addition, arthritis and other disorders of the mus- cles and bones are among the most common problems for which older people consult physicians (Adams 1995). Nonsteroidal anti-inflammatory drugs (NSAIDs) (e.g., ibuprofen, naproxen, indomethacin, and diclofenac) and aspirin are commonly prescribed or recommended for the treatment of these disorders and are purchased OTC in huge amounts. Several poten- tial interactions exist between alcohol and these agents, as follows:
- NSAIDs have been implicated in an increased risk of ulcers and gas- trointestinal bleeding in elderly people. Alcohol may exacerbate that risk by enhancing the ability of these medications to damage the stomach mucosa (Adams 1995). 6
- Aspirin, indomethacin, and ibupro- fen cause prolonged bleeding by inhibiting the function of certain blood cells involved in blood clot formation. This effect also appears to be enhanced by concurrent alco- hol use (Deykin et al. 1982).
- Aspirin has been shown to increase BALs after small alcohol doses, possibly by inhibiting first-pass metabolism (Roine et al. 1990).
An important pharmacokinetic interaction between alcohol and aceta-
minophen can increase the risk of acetaminophen-related toxic effects on the liver. Acetaminophen break- down by CYP2E1 (and possibly CYP3A) results in the formation of a toxic product that can cause poten- tially life-threatening liver damage. As mentioned earlier, heavy alcohol use enhances CYP2E1 activity. In turn, enhanced CYP2E1 activity increases the formation of the toxic acetamino- phen product. To prevent liver damage, patients generally should not exceed the maximum doses recommended by the manufacturers (i.e., 4 grams, or up to eight extra-strength tablets of acetaminophen per day). In people who drink heavily or who are fasting (which also increases CYP2E1 activ- ity), however, liver injury may occur at doses as low as 2 to 4 grams per day. The specific drinking levels at which acetaminophen toxicity is enhanced are still unknown. Because acetaminophen is easily available OTC, however, labels on the packages warn people about the potentially dangerous alcohol-acetaminophen combination. Furthermore, people should be aware that combination cough, cold, and flu medications may contain aspirin, acetaminophen, or ibuprofen, all of which might con- tribute to serious health consequences when combined with alcohol.
Opioids. Opioids are agents with opium-like effects (e.g., sedation, pain relief, and euphoria) that are used as pain medications. Alcohol accentuates the opioids’ sedating effects. Accord- ingly, all patients receiving narcotic prescriptions should be warned about the drowsiness caused by these agents and the additive effects of alcohol. Overdoses of alcohol and opioids are potentially lethal because they can reduce the cough reflex and breathing functions; as a result, the patients are at risk of getting foods, fluids, or other objects stuck in their airways or of being unable to breathe. Certain opioid pain medications (e.g., codeine, propoxyphene, and oxycodone) are manufactured as combination products containing acetaminophen. These combinations
can be particularly harmful when combined with alcohol because they provide “hidden” doses of acetamin- ophen. As described in the previous section, alcohol consumption may result in the accumulation of toxic breakdown products of acetamino- phen. Therefore, patients using opioid-acetaminophen combination products should be cautioned about restricting the total amount of acetamin- ophen they ingest daily (i.e., they should not take regular acetaminophen in addition to the combination product).
Warfarin. The anticoagulant warfarin is used for the prevention of blood clots in patients with irregular heart rhythms or artificial heart valves; it is also used to treat clots that form in extremities such as legs, arms, or some- times the lungs. Its anticoagulant effect is acutely altered by even small amounts of alcohol. In people taking warfarin and ingesting a few drinks in one sitting, anticlotting effects may be stronger than necessary for medical purposes, placing these people at risk for increased bleeding. This excessive warfarin activity results from alcohol- related inhibition of warfarin metab- olism by cytochrome P450 in the liver (Lieber 1994). Conversely, in people who chronically drink alcohol, long- term alcohol consumption activates cytochrome P450 and, consequently, warfarin metabolism. As a result, war- farin is broken down faster than nor- mal, and higher warfarin doses are required to achieve the desired antico- agulant effect. Thus, alcohol con- sumption can result in dangerously high or insufficient warfarin activity, depending on the patient’s drinking pattern. Therefore, patients taking warfarin generally should avoid alcohol.
Moderate Alcohol Consumption and OTC or Herbal Medications
Use of OTC medications is widespread among the general population. Accord- ing to a recent survey, 85 percent of adults ages 18 and older have used OTC pain relievers at least once, and
50 Alcohol Research & Health
(^6) Moderate alcohol use by itself, however, does not appear to be associated with an increased risk of ulcers or gastrointestinal bleeding and also is unlikely to cause a certain type of inflammation of the stomach lining (i.e., hemorrhagic gastritis) that has been observed after heavy alcohol use.
52 Alcohol Research & Health
M
any people who are being treated for chronic health problems, such as diabetes and high blood pressure (i.e., hypertension), consume alcohol, whether occasionally or regularly. As described in the main article, alcohol consumption, even at mod- erate levels, may interfere with the activities of many medications prescribed for such conditions. In addi- tion, however, alcohol use may contribute to or exac- erbate certain medical conditions.
Diabetes
In people with diabetes, control of the levels of the sugar glucose in the blood is severely impaired, either because these people lack the hormone insulin, which plays a central role in blood sugar regulation, or because their body does not respond appropriately to the insulin they produce. Alcohol consumption in dia- betics can result either in higher-than-normal blood sugar levels (i.e., hyperglycemia) or in lower-than-nor- mal blood sugar levels (i.e., hypoglycemia), depending on the patient’s nutritional status (Emanuele et al. 1998). Thus, long-term (i.e., chronic) alcohol consump- tion in well-nourished diabetics can lead to hyper- glycemia. Conversely, alcohol consumption in diabetics who have not eaten for a while and whose glucose resources are exhausted (i.e., who are in a fasting state) can induce hypoglycemia. Both hyperglycemia and hypoglycemia can have serious health consequences. Diabetes medications that substitute for or stimulate the body’s own insulin production (e.g., insulin or sul- fonylureas) also may lead to hypoglycemia. Alcohol-induced hypoglycemia occurs in the fasted state, when the diabetic’s blood sugar levels are already low and the body depends on the production of new glucose molecules (i.e., gluconeogenesis) to maintain sufficient blood glucose levels. Gluconeogenesis, which occurs in the liver, requires certain compounds whose levels are regulated by a substance called reduced nicotinamide adenine dinucleotide (NADH). Alcohol metabolism in the liver generates excessive NADH levels and thus reduces the levels of the compounds needed for gluconeogenesis, thereby contributing to
a further drop in blood sugar levels. This response is particularly critical in diabetics taking medications that can cause hypoglycemia. Consequently, these patients should be advised to drink alcohol only with or shortly after meals. Diabetics who consume alcohol also must be alert to the fact that the symptoms of mild intoxication closely resemble those of hypoglycemia. Accordingly, diabetics should check their blood glucose levels when- ever they are uncertain about whether their symptoms are caused by hypoglycemia or alcohol intoxication (for additional recommendations for diabetics who consume alcohol, see the textbox). Finally, patients using certain diabetes medications (e.g., chlorpropamide) should be cautioned that the medications can cause a disulfiram-like reaction when alcohol is consumed.
Hyperlipidemia
In people with hyperlipidemia, the levels of fat molecules in the blood—particularly molecules called triglycerides—are higher than normal. This condition can be associated with an increased risk of various health problems, the most serious of which is cardiovascular disease. Alcohol consumption may exacerbate hyper- lipidemia, because the same metabolic alcohol effects that inhibit gluconeogenesis also inhibit fat metabolism. As a result, the production of certain molecules called very low density lipoprotein (VLDL) particles is increased. Thus, people with elevated triglyceride lev- els in the blood should probably abstain from alcohol to determine if alcohol consumption is contributing to their elevated lipid levels.
Hypertension Elevated blood pressure is a risk factor for cardiovas- cular disease, including heart attacks. Alcohol is known to cause a dose-dependent elevation in blood pressure (Beilin 1995). Researchers do not yet know exactly what levels of alcohol consumption cause hypertension (for more information, see the article by Klatsky, pp. 15–23). However, all patients who
Alcohol’s Influences on
Various Disease States
What Is Moderate Drinking?
Vol. 23, No. 1, 1999 53
Alcohol and Medication Interactions
are diagnosed with high blood pressure should be questioned regarding their alcohol intake before being started on antihypertensive therapy. In some of those patients, cessation of drinking alone may reduce blood pressure and thus obviate the need for pharmacological treatment. Furthermore, patients taking certain kinds of cardiac medications (e.g., isosorbide [Isordil^ and Ismo], terazosin [Hytrin], doxazosin [Cardura]) should be warned that alco-
hol consumption in combination with those medi- cations may cause lower-than-normal blood pres- sure. These important potential risks associated with even moderate alcohol consumption (i.e., one or two standard drinks 1 per day) must be consid- ered when discussing the cardiovascular benefits associated with moderate drinking (e.g., reduced risk of heart attacks and certain kinds of strokes.)
Hepatitis C Infection
Infection with the hepatitis C virus, which can result in serious and even fatal liver damage, is common in the United States and around the world. The only effective treatment to date involves a substance called interferon-α, often in combination with an agent called ribavirin, and has a cure rate of approximately 40 percent. Heavy alcohol use in patients infected with hepatitis C accelerates the rate of liver damage and increases the risk of cirrhosis. Moreover, heavy alcohol use appears to reduce the number of hepati- tis C-infected people who respond to treatment with interferon-α. Researchers do not yet know how alcohol consumption exacerbates disease progression and interferes with treatment. Nevertheless, people infected with the hepatitis C virus probably should avoid using alcohol, particularly during interferon-α treatment.
—Ron Weathermon and David W. Crabb
References BEILIN , L.J. Alcohol and hypertension. Clinical and Experimental Pharmacology and Physiology 22:185–188, 1995. EMANUELE , N.V.; S WADE , T.F.; AND EMANUELE , M.A. Consequences of alcohol use in diabetics. Alcohol Health & Research World 22(3):211–219, 1998.
Preventing Alcohol-Induced
Hypoglycemia
Alcohol-consuming diabetic patients should consider the following general suggestions for preventing alcohol-induced hypoglycemia:
- Never consume alcohol without food or while in a fasting state.
- Consume only moderate amounts of alcohol (i.e., one or two bottles of beer, glasses of wine, or mixed drinks at one sitting), and drink no more than once or twice weekly.
- Allow 1.5 to 2 hours between drinks.
- Avoid sugar-containing drinks, and consume only light beer, dry wine, or drinks mixed with diet sodas.
- Check blood sugar levels if unsure whether certain body sensations (e.g., light-headedness) result from hypo- glycemia or alcohol effects.
- Be on the alert for alcohol hidden in prescription and over-the-counter medications.
(^1) A standard drink is defined as one 12-ounce can of beer or bottle of wine cooler, one 5-ounce glass of wine, or 1.5 ounces of distilled spirits and is equivalent to approximately 0.5 ounce, or 12 grams (g), of pure alcohol.