




















Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
A comprehensive overview of atherosclerosis, a condition characterized by the buildup of plaque inside arteries. It covers the underlying mechanisms, risk factors (modifiable and non-modifiable), and strategies for prevention and management. The document also discusses coronary heart disease, angina, and related diagnostic evaluations and treatments, offering valuable insights into cardiovascular health and disease prevention. It is useful for medical students and healthcare professionals.
Typology: Lecture notes
1 / 89

This page cannot be seen from the preview
Don't miss anything!
Atherosclerosis by the Numbers
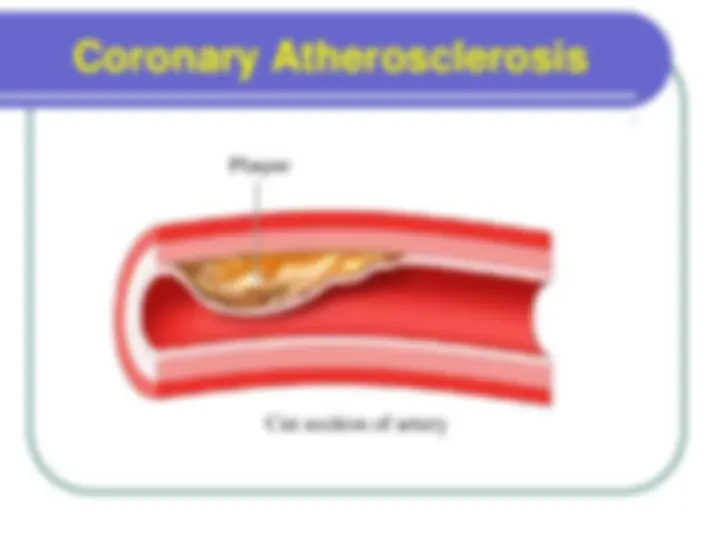
Coronary Heart Disease The major underlying cause is atherosclerosis.
Pathogenesis Response to injury hypothesis , Atherosclerosis is considered to be a chronic inflammatory response of the arterial wall initiated by the injury to the endothelium.
Endothelial Injury (^) One hypothesis of plaque formation suggests that injury to the endothelial vessel layer is the initiating factor in the development of atherosclerosis. (^) Possible injurious agents are: Products associated with smoking; Immune mechanisms; Mechanical stress, such as that associated with hypertension. (^) Hyperlipidemia, particularly LDL with its high cholesterol content, is also believed to play an active role in the pathogenesis of the atherosclerotic lesion
Deregulation of cholesterol levels results in the existence of more LDL in the blood than can be taken up by LDL receptors. Excess LDL is oxidized becoming oxidized (ldl-ox) by oxygen free radicals (^) Oxygen free radicals are a type of harmful body metabolism by-products. Normally free radicals are removed by anti-oxidants In the vascular endothelial, the deficiency of Nitric Oxide (NO) antioxidant aids oxidized LDL to cause Endothelial disruption leading to platelet adhesion and fibrin deposition Role of Lipids in Plaque Development cont’d
(^) An injury to the endothelial lining allows LDL particles, monocytes, and platelets to enter the smooth muscle tissue (^) Inflammation at the injury site triggers the conversion of monocytes to microphages, which scavenge the LDL particles and cholesterol to form enlarged foam cells. Under the microscope, the lesion appears as a fatty streak. Foam cells eventually die, and further propagate the inflammatory process. (^) There is also smooth muscle proliferation and migration from tunica media to intima responding to cytokines secreted by damaged endothelial cells. This would cause the formation of a fibrous capsule covering the fatty streak. (^) Smooth muscle cells, foam cells, platelets, and LDL particles form fibrous plaque Lipids and Inflammation in Plaque Development
Fatty Streaks Injury or infection can disrupt normal endothelial function and initiate formation of atherosclerotic lesions known as fatty streaks. Fatty streaks are thin, flat yellow intimal discolorations that progressively enlarge by becoming thicker and slightly elevated as they grow in length Fatty streaks typically consist of macrophages and smooth muscle cells that have become distended with lipid to form foam cells.
Age A dominant influence Atherosclerosis begins in the young, but does not precipitate organ injury until later in life Gender Men more prone than women, but by age 60- 70 about equal frequency Family History Familial cluster of risk factors Genetic differences Non Modifiable Risk Factors in Atherosclerosis
Modifiable Risk Factors (potentially controllable) Elevated Homocysteine: Homocysteine inhibits elements of the anticoagulant cascade and is associated with endothelial damage. Infections: Herpes virus; Chlamydia pneumoniae: The organisms may play a role in atherosclerotic development by initiating and enhancing the inflammatory response (^) Obesity, sedentary lifestyle, stress: lack of activity can worsen other risk factors for atherosclerosis.
Modifiable risk factors