


Physical Assessment
Part One
Lisa Moore DNP, RN









Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
A structured overview of physical assessment techniques in nursing. It covers essential components such as health history, physical examination techniques (inspection, auscultation, percussion, palpation), and specific assessments for various body systems (skin, heent). The guide emphasizes the importance of a systematic, head-to-toe approach and includes practical tips for conducting thorough and respectful patient assessments. It is designed to equip nursing students with the foundational knowledge and skills necessary for effective patient evaluation and care planning, ensuring they can accurately identify patient needs and health status.
Typology: Assignments
1 / 38

This page cannot be seen from the preview
Don't miss anything!
Nursing Assessment
Identify needs, preferences, and ability of the patient
Nursing assessment includes: Interview, observation, symptoms, verbal and nonverbal communication, medical and social history, other info about patient
Nursing Assessment
Physical Vital signs, skin color and condition, consciousness, motor and sensory nerve function, nutrition, sleep, elimination
Psycho/Social Family and support, occupation, mood and emotional tone, health beliefs, and religion or spiritual views
Comprehensive - Admission H & P
Ongoing - usually once per shift
Focused – evaluate specific problem
Emergency - ABC’s, ensure survival
Components of the health assessment
Health history - subjective
Physical assessment - objective
Health History (^) Chief concern or reason for seeking healthcare Demographic information (^) History of present health concern (^) Health history - (^) medical hx, meds, allergies, effect of illness on lifestyle/ADL’s (^) Family history (^) Psychosocial & Lifestyle history (^) support network, coping mechanisms, smoking, drinking, nutrition, sleep habits, exercise, mental health, etc) (^) Spiritual health Review of systems (ROS)
Enter the room and wash your hands before gloves
Use standard precautions for all patients
Make sure patient is comfortable
Two patient identifiers
Name
Medical Record Number
Respect privacy
Organized approach to exam
Hello Mr (s)________. My name is _________________ and I am an ACC nursing student. I am here to do a physical assessment. How are you feeling this morning?
Look Listen Touch
Looking or observing
Color, shape, size, symmetry, position and movement
Good lighting is very important
Stethoscope Tips (^) Earpieces tilted towards nose (^) Diaphragm for high pitched sounds: (^) normal heart, lung, & bowel sounds (^) Bell for low pitched sounds: (^) Heart murmurs (^) Clean between patients! (^) Warm it up for patient comfort
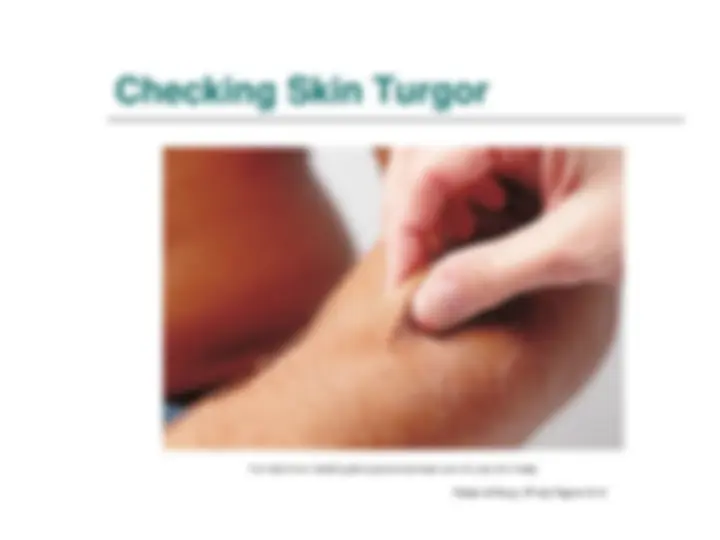
Checking Skin Turgor Potter & Perry, 9th^ ed, Figure 31-
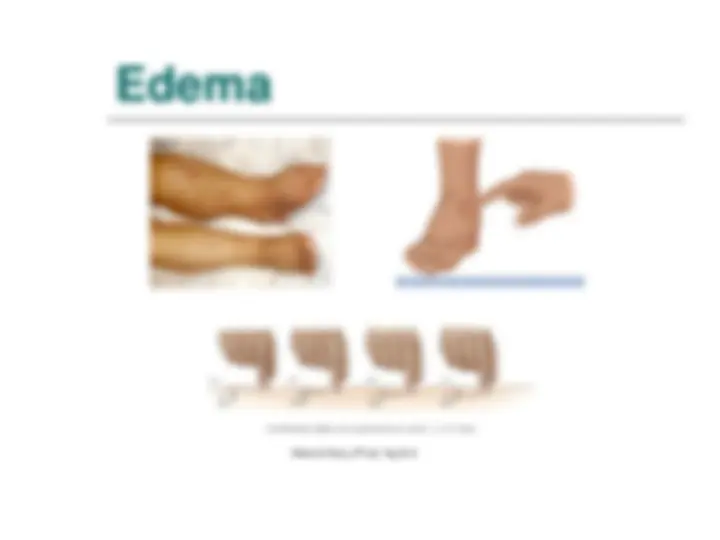
Potter & Perry, 9th^ ed, Fig 31-