Download HIV-AIDS: Etiology, Transmission, Pathogenesis, and Clinical Manifestations and more Lecture notes Pathophysiology in PDF only on Docsity!
HIV - AIDS
DEFINITION:
Acquired Immunodeficiency Syndrome (AIDS) is a disease caused by human
immunodeficiency virus (HIV), a retrovirus (RNA) and is characterized by
profound immunosuppression that leads to opportunistic infections, secondary
neoplasms and neurologic manifestations.
EPIDEMIOLOGY:
AIDS is pandemic (widespread)
Incidence has decreased from 11.2% in the year 2000 to 4.6% in 2018.
37.9 million people live with AIDS globally ( as per 2018 report)
Globally, death rate has decreased, in 2018 estimated death was 770,
The burden of AIDS in India is estimated at 2.1 million cases; prevalence is
high in states of Maharashtra, Andhra Pradesh, Karnataka, Telangana, West
Bengal, Tamil Nadu, etc.
ETIOLOGY:
- AIDS is caused by RNA (retrovirus) virus called human immunodeficiency virus (HIV)
- HIV which cause AIDS are the cytopathic viruses (structural changes in the host cells), namely (i) HIV- (ii) HIV-
- HIV-1 is common
- HIV-2 is noted in West Africa and parts of India
HIV-1 and -2 differ in their genes
ROUTES OF TRANSMISSION:
Sexual contact
- 75% cases of HIV transmission
- transmission from male-to-male and male-to-female is more potent than female-to-male
- Transmission via blood and blood products
- accounts for 25% of the HIV transmission
- Injection drug abusers
- Haemophiliacs (who receive large amounts of clotting factor concentrates from pooled blood components)
- Recipients of HIV infected blood
PATHOGENESIS (or) LIFE CYCLE OF HIV:
Selective tropism for CD4 molecule receptor
- glycoprotein envelop of HIV has selective tropism for cells containing CD4 receptor like CD4+T-cells (T-helper cells), monocyte macrophages, microglial cells
- these cells are present in cervix, Langerhans cell of skin, and follicular dendritic cells
- HIV enter through any route and it affect the CD4+T cells Internalisation
- the glycoprotein (gp 120) combines with CD4 receptor along with chemokine co-receptor
- then, gp41 present in the envelop internalise with CD4+T cell membrane
- Uncoating and viral DNA formation
- reverse transcriptase enzyme of the viral RNA forms a single- and double-stranded DNA and the original RNA strands are destroyed
- Viral integration
- after sometime, the viral integrase protein inserts the viral DNA into the nucleus of the host T cell and integrates in the host cell DNA.
- it is termed asHIV provirus
- Viral replication
- the host DNA transcripts for viral RNA with presence oftat gene (enhances the efficiency of viral replication)
- release of cytokines from T helper cells facilitates the multiplication of HIV (cytokines IL-2, INF-γ, IL-4, IL-5)
- virus particles fill the cytoplasm and acquire protein coating.
- release cytokines spread infection to CNS by TNF-α.
- Latent period and immune attack
- infection remains latent for a long time in an inactive infected T-cell.
- immune system produce antibodies with participation of CD4+, CD8+ and macrophages
- period is short and virus overpowers the host immune system
- CD4+T cell destruction
- replicated viral particles form buds in the walls of CD4+T cell
- cell membrane of CD4+T cells are damaged during detachment of virus and leads to apoptosis of CD4+T cells
Mechanism of T-Cell Depletion in HIV Infection:
Direct cytopathic effects of replicating virus cause loss of CD4+ T cells.
Approximately 100 billion new viral particles are produced and simultaneously about
1 to 2 billion CD4+T cells die each day causing immunodeficiency.
To an extend, the immune system replace the dying T cells, and with progression of
disease, the renewal of CD4+T cells is reduced.
Other factors responsible for loss (or) function of CD4+T cell:
Chronic activation of uninfected cells
HIV infection of cells in lymphoid organs
Fusion of infected and uninfected cells
Qualitative defects in T cell function
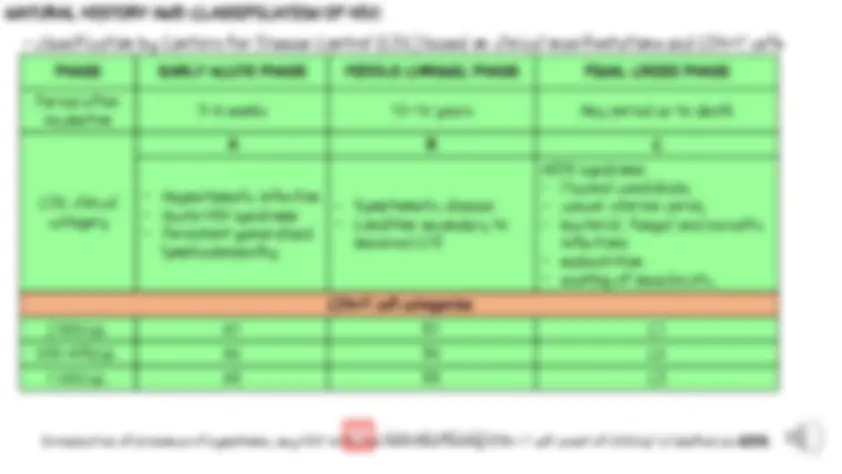
NATURAL HISTORY AND CLASSIFICATION OF HIV:
- classification by Centers for Disease Control (CDC) based on clinical manifestations and CD4+T cells PHASE EARLY ACUTE PHASE MIDDLE CHRONIC PHASE FINAL CRISIS PHASE Period after incubation 3-6 weeks^ 10-12 years^ Any period up to death
CDC clinical category
A B C
Asymptomatic infection Acute HIV syndrome Persistent generalized lymphadenopathy
Symptomatic disease Condition secondary to impaired CMI
AIDS syndrome Mucosal candidiasis, cancer uterine cervix, bacterial, fungal and parasitic infections malnutrition wasting of muscles etc.
CD4+T cell categories
500/μL A1 B1 C 200-499/μL A2 B2 C < 200/μL A3 B3 C
Irrespective of presence of symptoms, any HIV-infected individual having CD4+ T cell count of <200/μl is labelled as AIDS.
CLINICAL MANIFESTATIONS AND
PATHOLOGICAL LESIONS OF HIV:
All organs / systems are affected Mechanisms causing pathologic lesions
- direct viral infection to immune cells, CNS and lymph nodes
- opportunistic infections
- secondary tumours, mainly in the end-stage characterized by certain secondary malignant tumours
- drugs used to treat HIV infection produce toxic effect (or) tumours (or) opportunistic infection
a) b) c) d)
Major abnormalities of immune system in
AIDS:
T-cell B-cell Natural killer cell Monocyte-macrophage
a.
b.
c.
Renal lesions and manifestations Hepatobiliary lesions and manifestations Cardiovascular lesions and manifestations Ophthalmic lesions Musculoskeletal lesions Endocrine lesions
Other lesions and manifestations
Secondary opportunistic infections – fungal (candidiasis), bacterial (tuberculosis), viral (CMV) and protozoal Secondary neoplasms – Kaposi sarcoma, primary CNS lymphoma, non-Hodgkins and Hodgkins lymphoma Neurologic disease – AIDS dementia complex, meningoencephalitis, aseptic meningitis, peripheral neuropathy