
Prepare for your exams
Study with the several resources on Docsity

Earn points to download
Earn points by helping other students or get them with a premium plan

Guidelines and tips


Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
Calcium Antagonists: Mechanisms, Types, and Clinical Applications, Lecture notes of Pharmacognosy
An overview of calcium antagonists, also known as calcium channel blockers. It explains how they work by blocking calcium influx through voltage-dependent calcium channels in smooth muscles, resulting in coronary and peripheral artery dilation and reduced heart afterload. The document also covers the different types of calcium channels and calcium antagonists, their regulatory roles, and their therapeutic uses in various conditions such as hypertension, coronary heart disease, and ischemic cerebral stroke.
Typology: Lecture notes
2018/2019
1 / 14

This page cannot be seen from the preview
Don't miss anything!






Related documents
Partial preview of the text
Download Calcium Antagonists: Mechanisms, Types, and Clinical Applications and more Lecture notes Pharmacognosy in PDF only on Docsity!
Calcium antagonists
(Summary)
Dr Ivan Lambev
Calcium antagonists
(calcium channel blockers)
They block calcium influx through voltage-
dependant calcium channels in the smooth
muscles. They dilate
coronaries and
peripheral arteries
and reduce
heart afterload.
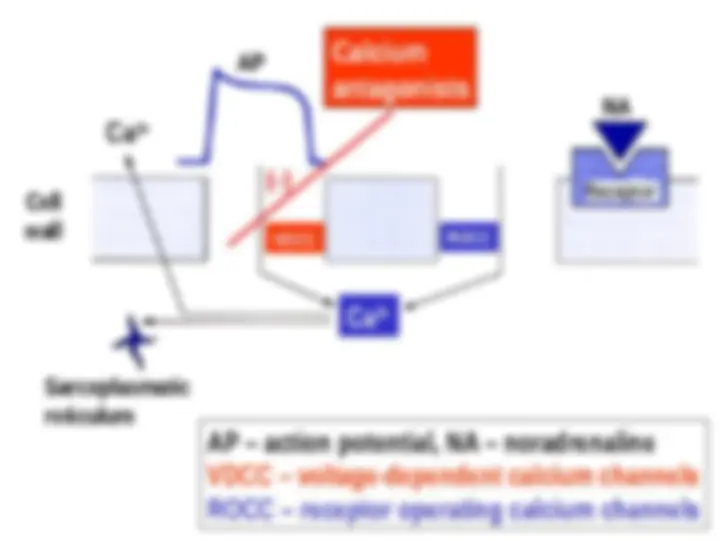
Regulation of intracellular calcium
Calcium antagonists block predominantly L-type
calcium channels, localized in the myocardium
and myocytes
of blood
vessels.
L-type channels
are connected
to the plateau
of the AP.
Plateau phase of AP
Calcium antagonists reduce coronary and
peripheral vascular resistance, decrease
blood pressure and myocardial oxygen
consumption.
Dihydropyridines (nifedipine, amlodipine,
etc) don’t have cardionegative inotropic,
chronotropic, and dromotropic effect in
comparison with verapamil and diltiazem.
Arterial hypertension
a) Dihydropyridines
b) Verapamil and Diltiazem
Coronary heart disease
a) Dihydropyridines
b) Verapamil and Diltiazem
Ischemic cerebral stroke
Cinnarizine, Flunarizine, Nimodipine
SV tachyarrhythmias: Verapamil, Diltiazem (i.v.)
Migraine (in remission periods)
Flunarizine, Verapamil
Beta-blockers + dihydropyridines: YES (OK)
Beta-blockers + Verapamil or Diltiazem = NO
Main indications
Calcium antagonists
Amlodipine
norm frequent dihydropyridine
t
1/
31–47 h, 55–91% p.o. bioavailability
5–10 mg/24 h p.o. (once daily)
Nifedipine (tachycardia!)
- effective in vasospastic angina
Diltiazem (in SR dosage forms)
Verapamil (Isoptin SR
®
- tabl. 240 mg)
(22% p.o. bioаvailability, first pass effect –
extensive liver metabolism)
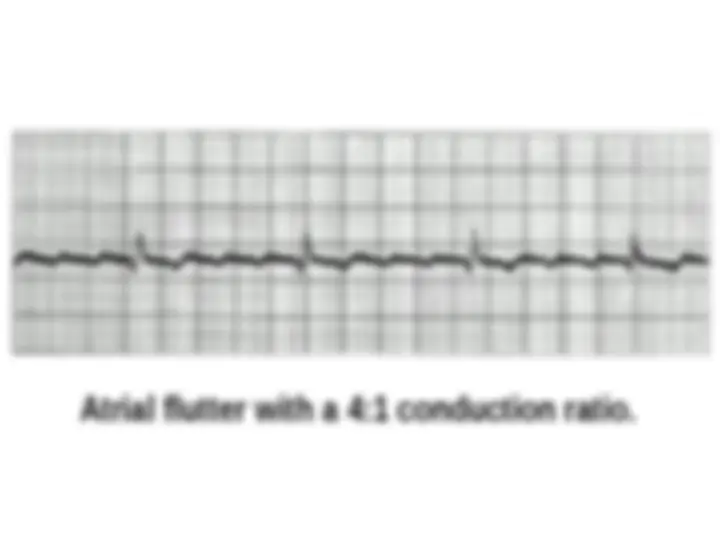
Atrial flutter with a 4:1 conduction ratio.
ARs of calcium antagonists
Arterial dilation: headache, flush, dizziness,
ankle swelling (resistant to treatment with
diuretics but not with ACE inhibitors).
Bradycardia and AV block (verapamil).
Verapamil + beta-blockers: potentiate
cardiodepression.
Tachycardia (nifedipine, nisoldipine).
Constipation (verapamil 8%; nifedipine 3%)
Haemorrhagic gingivitis