Download Caring for Patients with Preeclampsia in a Community Hospital and more Study notes Nursing in PDF only on Docsity!
Development and Evaluation of a Protocol: Caring for Patients with Preeclampsia in a Community Hospital By Christy A. Evers, BSN, RN University of Kansas School of Nursing 2019 Submitted to the School of Nursing and The Graduate Faculty of the University of Kansas in partial fulfillment of the requirements for the degree of Doctor of Nursing Practice. Dr. Cara Busenhart
Faculty Project Committee, Chair Dr. JoAnn Peterson
Faculty Project Committee, Member January 7, 2019
Date Project Proposal Accepted
The DNP Project committee for Christy Evers certifies that this is the approved version of the following DNP Project:
Development and Evaluation of a Protocol: Caring for Patients with
Preeclampsia in a Community Hospital
Dr. Cara Busenhart Chair Dr. JoAnn Peterson Member Date Approved: March 8 , 2019
Contents
- 1: Introduction
- 2: Problem and Significance
- Patient Education after Diagnosis
- 3: Project Details
- Design
- Theoretical Framework
- Setting
- Methodology
- Quality Improvement Determination.
- Review of Literature.
- Development of Protocol.
- Evaluation of Protocol.
- Analysis of Protocol.
- 4: Results
- Survey Results
- Revised Protocol
- Implications for practice
- 5: Conclusion
- References
- Appendix A
- Appendix B
- Appendix C
- Appendix D
1: Introduction Maternal mortality and morbidity are a worldwide concern. In 2000, the United Nations presented the Millennium Development Goals (MDG) which were intended as a health blueprint for all countries. Of the eight goals, one was to decrease worldwide maternal mortality and morbidity by 75% by 2015 (Jacobsen, 2019). From 2000 to 2014, maternal mortality and morbidity trended the opposite direction in the continental United States, while being reduced 44% worldwide (MacDorman et al., 2016; Jacobsen, 2019). “The well-being of mothers, infants, and children determines the health of the next generation and can help predict future public health challenges for families, communities, and the medical care system” (Office of Disease Prevention and Health Promotion, 2018, para 1). The maternal mortality and morbidity rate in the United States is staggering. According to the Central Intelligence Agency, the United States ranks 49th^ out of 184 countries for maternal mortality, higher than any other developed country, and it is still on the rise (Central Intelligence Agency, 2018). This concerning fact has caught the attention of many influential practice leaders in women’s health including the American Congress of Obstetrics and Gynecologists (ACOG), American College of Nurse-Midwives (ACNM), Association of Women’s Health, Obstetric, and Neonatal Nurses (AWHONN), and the California Maternal Quality Care Collaborative (CMQCC). The use of protocols, triggers, bundles, and checklists have led to improved outcomes for women when implemented to address practice concerns (Arora et al., 2016). The goal of implementing an evidenced-based protocol is to improve the outcomes for women, improve the readiness of the unit to care for patients at risk for or diagnosed with a complication, and to
HELLP (hemolysis, elevated liver enzymes, low platelets) syndrome, organ failure, disseminated intravascular coagulation, and death (ACOG, 2013; August & Sibai, 2018; Supplee, Bingham, & Kleppel, 2017; Sutton, Harper, & Tita, 2018). Hypertensive disorders of pregnancy encompass several diagnoses. More than 10% of pregnancies are affected by a hypertensive disorder (Sutton, Harper, & Tita, 2018). Classically, hypertension is defined as a systolic blood pressure of greater than or equal to 140 mm Hg and/or a diastolic blood pressure of greater than or equal to 90 mm Hg (ACOG, 2013). But, hypertension may develop during the pregnancy and may lead to maternal morbidity and/or mortality. Hypertensive disorders of pregnancy include preeclampsia, eclampsia, gestational hypertension, chronic hypertension with superimposed preeclampsia, and HELLP Syndrome. For this project, there will be a focus on differentiating gestational hypertension from preeclampsia. See Figure 1 for diagnostic criteria for those hypertensive disorders reviewed below. Chronic Hypertension (^) • BP of ≥ 140 mm Hg systolic or ≥ 90 mm Hg prior to conception
- Identified prior to 20 weeks gestation
- Continues after 12 weeks gestation
- Use of antihypertensive medications prior to pregnancy Preeclampsia • BP of ≥ 140 mm Hg systolic or ≥ 90 mm Hg or higher on 2 occasions greater than 4 hours apart
- Occurring after 20 weeks gestation
- Proteinuria Severe Features of Preeclampsia One or more of the following:
- BP of ≥ 160 mm Hg systolic or ≥ 110 mm Hg
- Thrombocytopenia
- Renal insufficiency
- Impaired liver function
- Pulmonary edema
- Cerebral or visual symptoms Chronic Hypertension with Superimposed Preeclampsia
- BP of ≥ 140 mm Hg systolic or ≥ 90 mm Hg
- Sudden increase or new-onset of proteinuria
- Worsening of hypertension
- Any of the severe features of preeclampsia Gestational Hypertension (^) • BP of ≥ 140 mm Hg systolic or ≥ 90 mm Hg after 20 weeks gestation
- No proteinuria or other signs of preeclampsia
- Resolves by 12 weeks postpartum Figure 1. Hypertensive disorders of pregnancy diagnostic criteria table. Adapted from ACOG, 2017. BP= Blood pressure, measured in mmHg.
Preeclampsia is one of the hypertensive disorders of pregnancy and is a common cause of maternal morbidity, and occasionally mortality (ACOG, 2013). Preeclampsia is categorized as either preeclampsia without severe features or preeclampsia with severe features. Preeclampsia is defined as a blood pressure of greater than or equal to 140 mm Hg systolic and/or 90 mm Hg diastolic on 2 occasions at least 4 hours apart in a patient in a previously normotensive patient that is greater than 20 weeks gestation and proteinuria of greater than or equal to 300 mg per 24- hour urine collection or protein/creatinine ratio of greater than 0.3 mg/dL. In the absence of proteinuria, preeclampsia can also be diagnosed by the patient having thrombocytopenia with platelet count of less than 100,000/microliter, serum creatinine concentrations of greater than 1. mg/dL in the absence of other renal disease, elevated blood concentrations of liver transaminases to twice normal concentration, pulmonary edema, and/or cerebral or visual symptoms. Preeclampsia with severe features is when any of the following criteria are met: (a) blood pressure of 160 mm Hg systolic or higher or 110 mm Hg diastolic or higher on two occasions at least 4 hours apart while the patient is on bedrest; (b) oliguria with urine output of less than 500 mL in 24 hours; (c) persistent headache unrelieved by analgesics or with visual disturbances; (d) pulmonary edema; (e) epigastric or right upper quadrant pain; (f) impaired liver functions greater to or equal to twice the upper limits of normal; (g) thrombocytopenia; or (h) renal insufficiency (ACOG, 2013; August & Sibai, 2018; Sutton, Harper, & Tita, 2018). Gestational hypertension is defined as hypertension, in the absence of proteinuria, beginning after 20 weeks gestation in a pregnant woman. Chronic hypertension is elevated blood pressures diagnosed prior to 20 weeks gestation, although this is more accurately diagnosed when a patient is not pregnant. Additionally, women that are prescribed, and taking,
include risk of pre-term birth, cerebral complications, and long-term cardiovascular disease in women (Sutton et al., 2018). With the use of an evidenced-based protocol, facilities have been able to reduce blood pressures in a timely fashion leading to a decrease in cerebral complications (Bernstein et al., 2017). Women that have been diagnosed with preeclampsia are at a greater risk, a relative risk of 7.6 times, to have preeclampsia in subsequent pregnancies (Dhariwal & Lynde, 2018). Standardized Policies The California Maternal Quality Care Collaborative (CMQCC) is comprised of key stakeholders from a variety of healthcare disciplines with one purpose in mind, improve the maternal mortality and morbidity in California (CMQCC, 2018). CMQCC has published toolkits for healthcare professionals to adopt for use in their own facilities. CMQCC has standardized care for patients and has provided the information in resources, print and online. This willingness to share resources and knowledge is important because the use of standardized policies is essential to ensure that mothers are getting proper and timely care (Arora et al., 2016). Complications in pregnancy, those situations that lead to maternal mortality and morbidity, may occur without any warning. Using evidenced-based protocols can ensure that the women that experience a complication are cared for in a manner that improves outcomes (Arora et al., 2016). Protocols are very helpful to clinicians because it is a reminder of the baseline expectation for providers and of the actions that are expected (Arora et al., 2016). Patient Education after Diagnosis Nurses are often unprepared to offer self-care education to postpartum mothers upon discharge from the hospital (Suplee, Bingham & Kleppel, 2017). Patients may not be receiving evidenced-based information and education throughout their stay and at discharge, including the
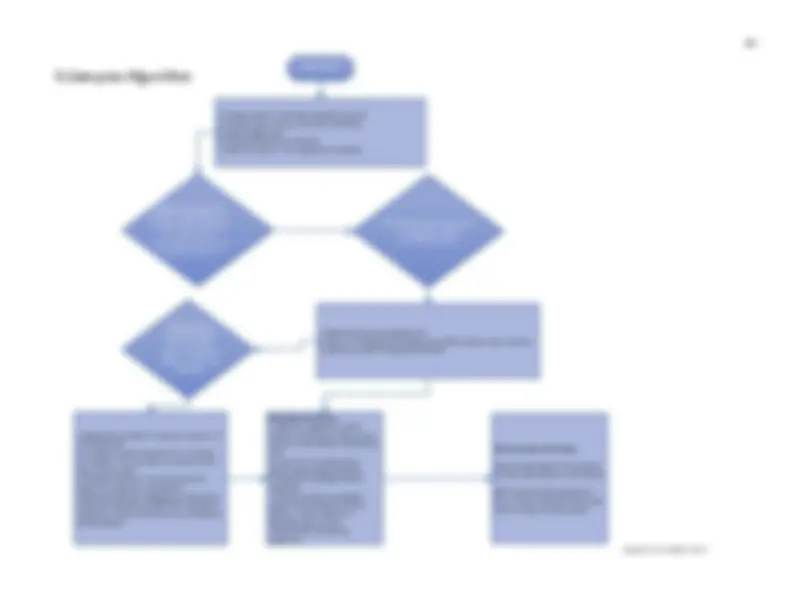
precautions, signs and symptoms of emerging or worsening conditions, and appropriate follow- up (Suplee, Bingham, & Kleppel, 2017). Since nurses provide a majority of postpartum discharge instructions to patients, it is important that nurses are able to give high-quality and succinct information to patients that covers any and all key points to reduce maternal mortality and morbidity (Suplee, Kleppel, Santa-Donato, & Bingham, 2016). Standardizing the discharge teaching for postpartum women has been effective in reducing readmissions and postpartum mortality (Bingham, Suplee, Morris, & McBride, 2018). 3 : Project Details Design The aim of this Doctor of Nursing Practice project was to develop an evidence-based, standardized policy and protocol for the care of women with hypertensive disorders of pregnancy during intrapartum and postpartum hospital care in a community hospital, including written discharge instructions for women diagnosed with hypertensive disorders of pregnancy. This protocol will help not only the providers, but also the frontline nurses, in providing timely care to patients that present with hypertension in pregnancy. Theoretical Framework The theoretical framework used for this project was the Iowa model, a framework used for implementation of evidenced-based practice that was first introduced in 1994 and has been revised since (Titler et al., 2001). The Iowa model starts with the premise that a change is necessary and a priority for the organization (see Figure 2 ). This model uses triggers, either problem- or knowledge-focused, to engage nurses in thinking about ways to improve efficiency or effectiveness of care. The model uses a team approach and will be modified slightly for this quality improvement project. The first step in the process is to determine a priority topic. A
term ventilator for breathing support. Many women choose the facility they deliver in based on the anticipated care for their newborn (March of Dimes, 201 5 ). The implication is that pregnant women with moderate risk are seen at this facility. There was no standardized protocol for the care of women diagnosed with hypertensive disorders, including preeclampsia, at this facility. The care of these women is dependent on nursing knowledge and physician orders. Physician preference drives the type of diagnostic evaluation or work-up, use of antihypertensive medication, and even how often blood pressure readings were obtained. Methodology This project is a quality improvement project for evidenced based practice which is defined as a formal and systematic method to improve the processes of a healthcare system (Batalden & Davidoff, 2007). The project begins with a matrix review of the literature to determine what research pertains to the phenomenon of preeclampsia and medications used in the hospital setting. A thorough review of the literature, development of a protocol and evaluation of the protocol by an interprofessional team are discussed here. Quality Improvement Determination. A determination of quality improvement was requested, and approved, for this project from the KUMC Human Subjects Committee/Institutional Review Board. The project qualified due to the project evaluating or improving the local implementation of widely-accepted clinical or educational standards that have been proven effective at other locations. Review of Literature. An initial search using CINAHL, PubMed, MEDline, and Google Scholar was performed. The search terms were “maternal mortality and morbidity”, “preeclampsia”, “preeclampsia protocol”, “preeclampsia management”, “preeclampsia AND protocol”, “preeclampsia AND management”, “clinical practice guidelines”, and “preeclampsia
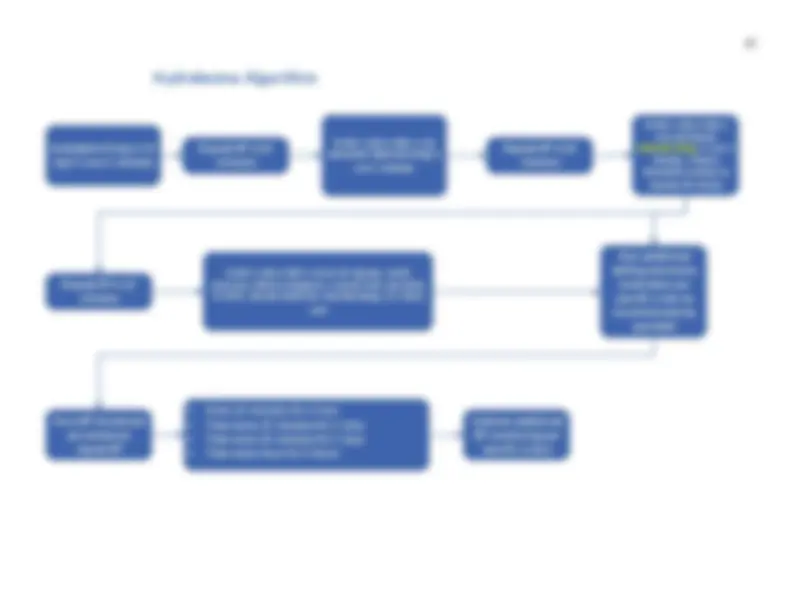
AND clinical practice guidelines”. Inclusion criteria for review included: (a) full-text resources, (b) English language, (c) publication within 5 years, and (d) research that focused on protocols and guidelines for patients with preeclampsia. Greater attention was given to literature focusing on the maternal mortality and morbidity in the United States related to hypertensive disorders in pregnancy. A matrix review was created and included as part of the appendices (see Appendix A). Research reviewed focuses on several aspects of the preeclamptic patient. In the area of medication, there are three medications routinely used for hypertensive emergencies: intravenous labetalol, intravenous hydralazine, and oral nifedipine (ACOG, 2013). These medications are often studied in research to determine the most efficacious. When reducing blood pressure in a pregnant patient, it is important to not reduce too quickly and lead to uteroplacental insufficiency (Gavit, Sharma, & Dixit, 2018). Research is split about the most effective medication to reduce blood pressure in women with a hypertensive emergency, but all research agrees that the difference is minimal. In studies comparing oral nifedipine and intravenous labetalol, oral nifedipine was found to be most effective in two studies by lowering the blood pressure the quickest (Gavit et al., 2018 ; Shekar et al., 2013). In contrast, comparing the two, labetalol has been effective with quicker results and less side effects in two studies (Dey et al., 2017 ; Padmaja & Sravanthi, 2017). Two studies found no difference in the efficacy of oral nifedipine and intravenous labetalol (Das et al., 2015; Kumari & Srilaxmi, 2016). Oral nifedipine and intravenous hydralazine have also been studied together. Sabir, et al, (2016) found intravenous hydralazine to be more effective and Sharma, et al, (2017) found no difference in the efficacy two medications.
The evidenced-based preeclampsia protocol (see Appendix B) encompasses the care of women diagnosed with preeclampsia from initial evaluation through discharge of both pregnant and postpartum women. The protocol includes the care of postpartum women readmitted with hypertension or preeclampsia. The preeclampsia protocol also includes the recommended discharge instructions, along with teaching, for the women that have been diagnosed with preeclampsia during their pregnancy. Evaluation of Protocol. After development, the protocol was presented and AGREE II instrument, designed by the Appraisal of Guidelines for Research and Evaluation, was shared with an interprofessional group of experts, via REDCap. Study data were collected and managed using REDCap electronic data capture tools hosted at The University of Kansas. The evaluation form consisted of 23 Likert-type statements of agreement (see Appendix C) with an area for comments and suggestions with each evaluation statement. The AGREE II instrument is both valid and reliable. The AGREE II instrument has been used in protocol evaluations for clinical guidelines in postpartum women and infants in primary care (Haran et al., 2014), World Health Organization (WHO) guidelines in maternal health (Polus et al., 2012), and clinical practice guidelines for postpartum hemorrhage (Novo et al., 2016). The participants included in the REDCap survey were seven OB/GYNs, eight Family Practice physicians that have delivery privileges at the hospital, six day shift Registered nurses with more than five years of labor and delivery experience, six night shift Registered nurses with more than five years labor and delivery experience and the nurse manager of the labor and delivery unit.
Analysis of Protocol. For the analysis, the Likert-type questions were reviewed to determine common levels of agreement amongst participants. The data was analyzed using the REDcap system, with descriptive statistics, including mean and range. 4 : Results Survey Results There were 27 total invitations sent with 15 completed for a 55.6% completion rate. Of those invited to the survey, three OB/GYNs, three family medicine physicians and nine Registered nurses responded to the survey (see Figure 3). Figure 3. Breakdown of interprofessional participants, by role, in the preeclampsia protocol survey. Adapted from REDCap. The AGREE II tool is divided into six domains. The first domain focuses on scope and purpose. All respondents to the survey answered positively to the overall objective being specifically described and the health questions in the guideline being specifically described in the protocol. The population to whom the guideline is meant to specifically describe statement yielded 86.7% partially agree or strongly agree answers. The second domain of the AGREE II tool asks respondents to rate level of agreement with statements relating to stakeholder involvement. Of all respondents, 87% either agree or 0 2 4 6 8 10 Registered Nurse OB/GYN Family Medicine
Please indicate your professional role in the
care of women in labor, delivery, recovery, and
postpartum:
In the fifth domain, applicability of the protocol was the focus. This domain started with a statement about the protocol describing facilitators and barriers to its applications and 20% of the respondents either disagreed or partially disagreed, 20% were neutral, and 60% either agreed or strongly agreed to the statement. All respondents were either neutral or agreed in some format, and over 50% strongly agreed, that the protocol provides advice and/or tools on how the recommendations can be put into practice. The potential resource implications of applying recommendation have been considered was either agreed or strongly agreed by 80% of the respondents. Two respondents disagreed that the protocol presents monitoring and/or auditing criteria, while over 73% either agree or strongly agree that the criteria is present in the protocol. The final domain had two statements about the editorial independence. Of the responses, 86.7% either agree or strongly agree that the views of the funding body have not influenced the content of the guideline while the other responses were neutral. The final question of the tool asked respondents to rate the competing interests of the guideline being recorded and addressed and over half of the respondents were neutral and the others either agreed or strongly agreed. Respondents were then asked to rate the overall quality of the guideline with a scale ranging from one to seven where the “1” is the lowest quality and the “7” is the highest quality, 26.7% selected a five, 40% selected a six, and 33.3% selected a seven (see Figure 4).
Figure 4. Participant rankings of overall quality of the preeclampsia protocol. Adapted from REDCap. When asked if the participants believe the protocol should be put into use, all respondents replied “yes” or “yes with edits” (see Figure 5). Figure 5. Bar graph of participants response about recommendation for use of the guideline. Adapted from REDCap. All participants had an opportunity for comments, including the following prompts: changes they would like to see, what they liked about the protocol, and perceived barriers to implementation. Comments regarding suggested improvements to the protocol include one from a participant that found an error in the hydralazine algorithm and clarification about who is to follow the protocol, physicians or nurses. Other comments include “great improvement to 0 1 2 3 4 5 6 7 7 6 5 4 3 2 1
Rate the overall quality of this guideline.
Scale of 1 (lowest possible quality) to 7
(highest possible quality):
0 2 4 6 8 10 12 14 No Yes with edits Yes
I would recommend this guideline for use: