Download Common Medical Conditions and Treatments and more Exams Nursing in PDF only on Docsity!
FNP TEST 1 QUESTIONS AND ANSWERS
HEENT
- A thin patient presents in office with hyperpigmentation and salt cravings. What lab do you want to do? ADDISON - Cortisol
- Which diabetic oral medication would you not want to use in a patient with HF?
- ACTOS (Pioglitazone) (THIAZOLIDINEDIONES)
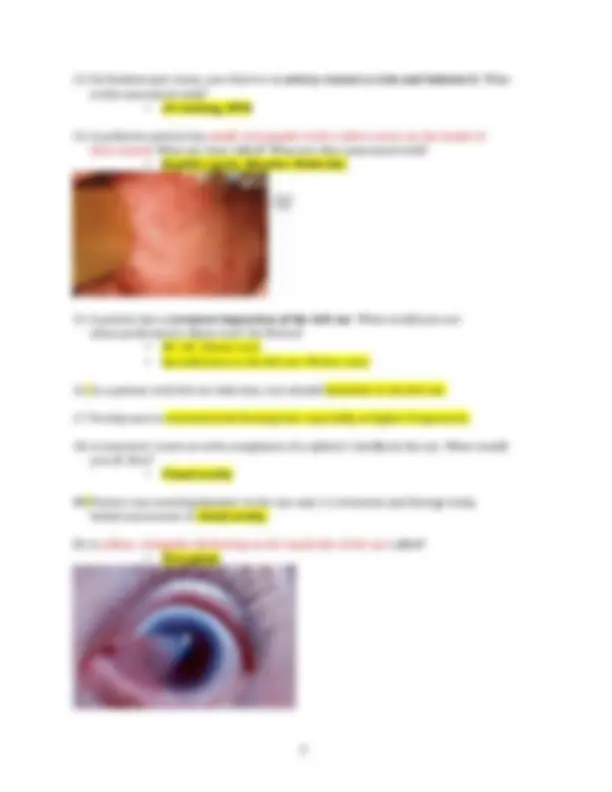
- Elderly patient presents with acute eye pain, blurred vision, headache, and n/v? What would you do? - Acute angle closure glaucoma, Refer to ED
- You perform a fundoscopic exam on a patient and see a swollen optic disc with blurred edges. What is this indicative of? - Papilledema, ICP
- Geriatric patient with progressive loss of vision and probable open-angle glaucoma can have notching of optic disc and changes in cup-to-disc ratio. 1. AV nicking = HTN (arterioles pressing on veins, arteries are smaller than veins, its hypertensive retinopathy , copper wire arterioles, flamed shaped hemorrhages. - Cotton wool spots = diabetes and/or HTN - Papilledema = ICP/ Meningitis - Optic disc cupping = IOP/Glaucoma 22 or higher - *WILL GET 2 or 4 questions on this
- What are some causes of ICP?
- What eye complaint is associated with sudden onset of floaters and complaints of a curtain closing? - Retinal detachment, refer to ED
8. What sinusitis is dental pain associated with? Maxillary
- What is a white, gray patch on the tongue or in the mouth called? What is it associated with? - Leukoplakia, HIV and oral cancer
- Adolescent presents with a painful, yellow ulcer with red base inside the mouth. What is it?
- Aphthous stomatitis, (canker sore) self-limiting. Resolves in 7- 10 days. Can use magic mouthwash. 2. College student with single, painful, intra-oral lesion with yellow center and erythematous base has aphthous ulcer. Aphthous stomatitis (canker sores): Single ulcers could also be caused by trauma from biting, braces, tooth, hot food, toothbrush; food intolerance or allergy; stress; hormone changes; genes; medications; stopping smoking.
- Besides avoiding allergens, what is the first line treatment for allergic rhinitis?
- Intranasal steroids. (Budesonide)
- A patient complains of swelling in the mouth, that is worse with meals, and comes and goes. It is commonly seen under the tongue and diagnose him with sialolithiasis. What is your treatment plan?
- Increase fluids, moist heat, NSAIDS, abx if infected, and surgery to remove stone
- What is the vascular area that anterior nosebleeds originate from?
- A 21-year-old female presents with complaints of nasal congestion for three weeks. She takes Afrin daily and NSAIDs, as needed, for migraines. What is the cause? - Afrin, or other nasal decongestant, use >3 days results in rebound congestion. This is called rhinitis medicamentosa
- What is the most common organism in acute otitis media? What is first line treatment? - S. Pneumoniae (Streptococcus pneumoniae): TTO: Amoxicillin What if the patient had an abx in the last three months? Augmentin (Amoxicillin / Clavulanic
- Patient has hives(ronchas) with penicillin and Ceftin (cephalosporin) and complains of n/v with erythromycin. What do you give? Azithromycin (Macrolide) erythromycin, roxithromycin, azithromycin and clarithromycin. - First-line indications for macrolides include the treatment of atypical community acquired pneumonia , H. Pylori (as part of triple therapy), chlamydia and acute non-specific urethritis.
- Patient was treated for Acute otitis media two weeks ago, but still complains of inner ear fullness. You educate him on middle ear effusion and tell him that it can last up to?
- Which patient is not at risk for H. Influenzae infection?
- or a patient with Otitis externa?
- What is the most common pathogen of Otitis externa?
- Pseudomonas aeruginosa
- Treat with? Corticosporin/hydrocortisone drops
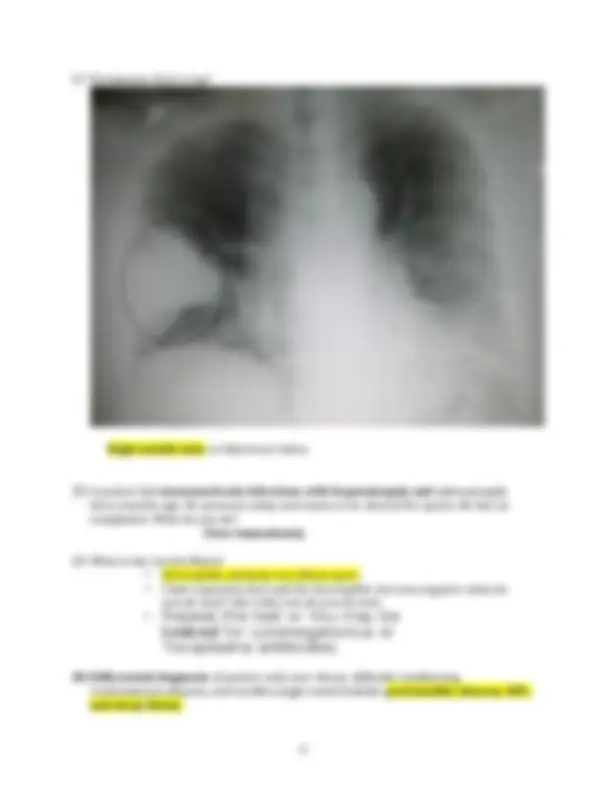
- Pneumonia chest x-ray? Right middle lobe or bilat lower lobes
- A patient had mononucleosis infections with hepatomegaly and splenomegaly three months ago. He presents today and wants to be cleared for sports. He has no complaints. What do you do? Clear immediately
- What is the test for Mono?
- Heterophile antibody test (Mono spot)
- I had a question that said the heterophile test was negative what do you do next? Like what test do you do next.
- Repeat the test or You may be
tested for cytomegalovirus or
Toxoplasma antibodies.
30.Differential diagnosis of patient with sore throat, difficulty swallowing, erythematous pharynx, and swollen single tonsil includes peritonsillar abscess, EBV, and strep throat.
- A middle-aged man presents with vesicular lesions on the right side of his abdomen. What is the cheapest (barato)treatment?
- An elderly patient complains of a slow growing lesion on her neck that is dry, red, and scaly. (Actinic keratosis). What is this a precursor to?
- Squamous cell carcinoma Actinic keratosis can lead to squamous cell carcinoma. Dx biopsy, refer to dermatology, TX topical 5 fluoracil 5-FU, cryotherapy. 39. Actinic keratosis can lead to Basal Cell Cancer : ( Hints: Waxy, pearly, telangiectasia
- How do you treat a subungual hematoma?
- Trephination- drill a hole in the finger and release the blood
- An elderly man has brown lesions that appear “ pasted on .” What do you advise him about these?
- Seborrheic keratosis, benign
- A 35-year-old appears with a yellow colored plaque on his upper eyelid. What labs would you draw?
- Lipid panel (xanthelasma, can be normal in over 40)
- What are pinpoint areas of bleeding when scales from a psoriatic lesion are removed? auspitz sign Psoriasis: Cause pitting in fingernails. TX topical steroids.
- A patient has smooth, dome shaped papules with central umbilication and a white plug. What do you suspect?
- A patient has superficial skin swelling and redness on his cheek. What is your diagnosis?
- Erysipelas Erysipelas of the face presents as painful, sharply demarcated erythema and edema. Erysipelas A subtype of cellulitis involving the upper dermis and superficial lymphatics that is usually caused by group A Streptococcus o (KEY WORD IS DEMARCATION) o TX: PCN or Macrolide o Caused by Strep infection 50. An adolescent patient has an erythematous, annular shape rash with raised borders on his arm. What is your diagnosis?
- Tinea corporis, antifungal cream
- Pruritic, angular , reddish-purple lesions with white lines in the center is - lichen planus.
- A patient has been treated for acne with Retin-A daily. He reports improvement, but states his skin is irritated. What do you do?
- Decrease his dose to three times a week
56-1- What if his acne wasn’t improving? Continue topical, add oral doxycycline (tetracycline)
- A fair skinned woman complains of flushing/blushing with pustules on her nose, mouth, chin and cheeks. What is this?
- Acne rosacea Treat with? Flagyl topical gel (Metronidazole)
- Pustular acne in doxycycline-allergic patient with recent exposure to MRSA can be treated with Bactrim. Or macrolides) (Mynocicline, Clindamycin) (doxycycline) Meniere's disease presents as horizontal nystagmus during an attack. inner ear disorder, episodes of vertigo, classic triad of symptoms – vertigo, tinnitus, hearing loss ; can resolve spontaneously or be chronic avoid caffeine, chocolate, tobacco, low sodium, TX meclizine (Antivert), diuretics, diazepam.
- An IV drug user presents with fever, chills, painful nodes on his fingers, over hands and feet and bleeding under his nailbed. What do you diagnose him with?
- Bacterial Endocarditis treatment – refer to cardiologist or ED for hospitalization and IV antibiotics; blood cultures x 3; 56. What is the first testing you would order on a patient you suspect to have AAA? - Ultrasound 57. What is an OTC medication that can exacerbate CHF? - NSAIDs 58. Medicines that can exacerbate GERD include calcium-channel blockers. (amlodipine, diltiazem, nifedipine, verapamil) 59. Foods that exacerbate GERD include chocolate, mints, caffeine, but not high- protein food.
- Geriatric arrhythmias can be caused by sinoatrial fibrosis.
- A 30-year-old male presents with a BP of 200/100. You hear an abdominal bruit on exam. What do you expect?
- Renovascular hypertension /renal artery stenosis, Not use ACEI (pril) in stenosis of renal artery 72.Carotid bruits can be caused by carotid narrowing.
- A patient has stable angina. What test do you order for him?
- An African American man presents to your clinic for follow up. He was previously placed on Losartan. His BP is still elevated. What do you do?
- Change to CCB 75. What is the cause of isolated systolic hypertension? TTO: Calcium Chanel Blocker
- Decreased elasticity of the arteries
- A patient complains of lower extremity pain with walking. The pain subsides when he sits down. What do you suspect?
- PAD What test would you use? Ankle brachial index PVD has swelling, darkening of skin of lower extremities 77. Name a few medications that interact with grapefruit juice. - Statin, CCB 78.Before initiating statin therapy , you should check AST/ALT. Liver enzymes)
- An overweight male presents with total cholesterol: 200, HDL: 35, LDL: 130 and Triglycerides: 350. What is your first line treatment?
- Diet and exercise -If the triglycerides were 650 , what would you do? Niacin -What are patients at risk for with high tri’s? Pancreatitis Cholesterol<200, HDL >40, LDL <100, Triglycerides < TX first line : life modifications, niacin, fenofibrate, statins. Always treat Triglycerides first.
80.Very high triglyceride levels put a patient at risk of pancreatitis.
81. A fat guy with high cholesterol should have initial intervention strategy of diet control and weight loss regimen.
- Besides(además) a SABA, what is your first line treatment in a patient diagnosed with chronic bronchitis? - Anticholinergic 83. First-line treatment of chronic bronchitis is short-acting beta-agonists. 84. Treatment for bacteria bronchitis
- What would you expect to hear on percussion of a patient’s lungs with COPD?
- Would oral steroids be considered long term management of a patient with COPD? - No 87. Long-term treatment of COPD does not include oral corticosteroids. 88. Polymyalgia rheumatic is treated with prednisone 20mg daily, with extremely slow taper over the course of a year. high risk for developing temporal arteritis 89. COPD patient with nighttime SpO2 of 88% should be placed on oxygen. 90. An elderly patient presents with HR:125, BP:88/56, confusion, and crackles in her lungs. Which would not constitute for a reason to admit this patient to the ED?
- A HIV patient is having his PPD read today. What would be the amount of induration that would qualify him as positive?
- 5mm -Where is TB most commonly seen in the lungs on XR? Upper or Hylium of lobes
- A HIV patient has a CD4 count of 200. What do you tell her?
- According to CDC, she has AID 93. Pt with HIV took high potency anti-viral treatments and CD4 is >400 , what does this indicate? This is good. Want higher than 350
- A female patient complains of RUQ pain, nausea, and aversion to smoking. What is your diagnosis?
- Hepatitis
- What lab/labs is elevated in chronic hepatitis? ALT (central to liver)alanina transferasa
- RUQ pain with radiation to shoulder after a heavy meal? Chole
- A patient has periumbilical pain. Which would NOT be in the list of differentials? - Appendicitis, hernia, gastroenteritis, or hepatitis
- An elderly patient presents with reports of weight loss and pencil like stools. What area of the colon would be considered?
- An elderly woman complains of intermittent diarrhea and weight loss. What would you do next?
- Colonoscopy 120. Most-specific test for an inflammatory intestinal condition is C.diff. 121 Person most likely to get C. diff is a patient who has taken abx recently for cellulitis. 122 What would you expect to see in a stool sample of a patient with an **inflammatory bowel disease?
- WBCs 123** An adult patient has complaints of acid reflux. He has been taking OTC tums. What is your first line treatment for him?
- H2 blockers 124 -A young woman complains of intermittent episodes of diarrhea and constipation. She complains of bloating , but it resolves with bowel movements. What do you suspect?
- IBS 125 The CHF is present in patient with: S3 heart sound, orthopnea, and paroxysmal nocturnal dyspnea. 126 An elderly woman is on a diuretic for CHF. Her creatinine level has gone from 0.8 to 1.2. What would you expect to see in her GFR? A geriatric patient with creatinine increasing from 0.8-1.2 on digoxin shows substantial decrease of GFR.
- Decrease in GFR ( Glomerular filtration rate) 127 Patient with calf pain upon exercise and reduced pedal pulses has arterial insufficiency 128 A patient with hyperpigmentation and swelling of lower legs has chronic venous insufficiency. 129 - What medication would you discontinue if you saw a patient’s creatinine increasing?
- ACEI , BB, or CCB? 130 -You suspect a patient has a UTI. You obtain a UA and it shows 2+ bacteria , - nitrites , and 3+ squamous cells. What do you expect?
- Contaminated sample 131 -Urinalysis given that shows 2+ bacteria, something like 15 WBC, and moderate squamous cells. The answers for interpretation include positive UTI and contamination. 132 - First line treatment for UTI in pregnancy? - Macrobid, but only in first two trimesters 133 -What is the gold standard diagnostic test for a patient with giant cell arteritis? - Temporal biopsy What is GCA commonly seen with? PMR Polimialgia reaumatica Describe PMR? Trouble getting out of bed, putting on bra 134 -A male patient presents with unilateral, knife like pain behind one eye and rhinorrhea. What is your treatment?
- High dose O 135 -A patient complains of low back pain that is relieved by sitting and worse with activity. What do you suspect?
- Herniated disk or spinal stenosis (sis=sit)? 136 -You ask an elderly patient to spell world backwards. What test are you performing?
- MMSE 137 - A patient with a history of migraines complains of a unilateral throbbing headache that has gradually worsened. She wants abortive therapy. What do you give her?
145 -What immunizations should a sickle cell patient have?
- All 146 -A patient comes in after falling with an outstretched hand. The XR is normal. What do you suspect? What kind of splint do you use? Thumb Spica splint Scaphoid fracture still having pain( Hand)
- repeat x-ray, splint wrist, refer to surgeon
- scaphoid fractures may not show on initial x-ray
- patient usually has history of falling forward on outstretched hand
- common complaint is deep, dull wrist pain that worsens with gripping or squeezing
- high risk of avascular necrosis and nonunion
A Salter–Harris fracture is a fracture that involves the epiphyseal plate or growth plate of a bone. It is thus a form of child bone fracture. It is a common injury found in children , occurring in 15% of childhood long bone fractures. 147 -A patient has lateral epicondylitis. What is your treatment? Rest, Ice, Compression, and Elevation (RICE) Any soft tissue injuries, use RICE 148 -What orthopedic maneuver tests for meniscal tear?
149 -You perform an anterior drawer sign. What is this testing? OJO
- ACL 150 -You want to test a patients MCL. Do you use the valgus or Varus stress test?
- Valgus Stress Test (“gum”) 151 -To assess MCL condition, valgus stress is applied.
- Valgus (X knee) - test MCL
- Varus ([ ] Knee) -test LCL 152 -A female complains of a pebble between her 3 rd^ and 4 th^ metatarsal. What do you suspect?
- Morton’s neuroma -What is the test? Mulder- Grasp Test and squeeze first and 5 th metatarsal. + pain.