Download Diagnosing Platelet Function Disorders: A Comprehensive Approach and more Exams Nursing in PDF only on Docsity!
Case Study of a 62 - year-old Female with Postoperative Bleeding and
Persistent Abnormalities on Platelet Aggregation Studies.
Case Presentation A 62-year-old female presented with a concerning palpable mass in her right breast in January
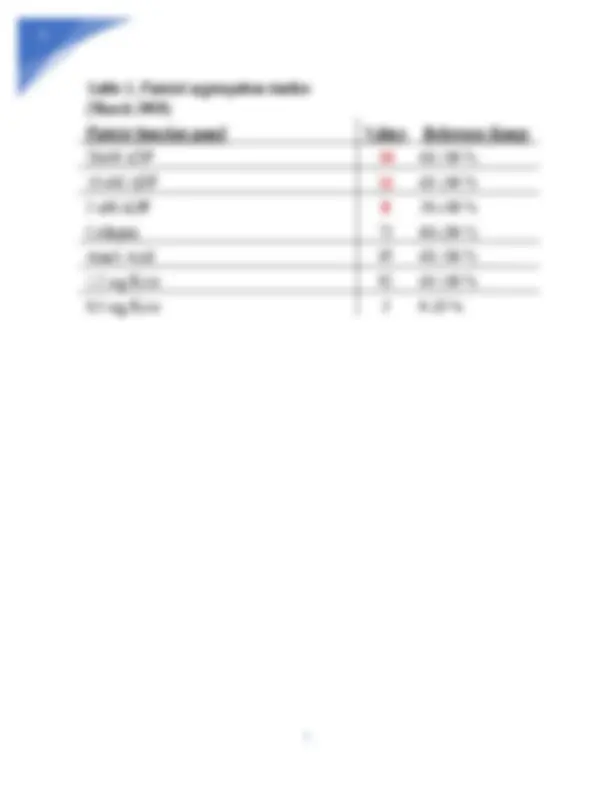
- The patient elected to undergo a lumpectomy, which was followed by a right modified radical mastectomy and axillary lymph node dissection. The right breast mastectomy was complicated by post-operative bleeding requiring transfusion of 1 unit of packed red blood cells (ISTH-BAT score 4). The patient’s past medical history was significant for easy bruising (ISTH- BAT score 1), frequent nosebleeds (ISTH-BAT score 1), heavy menstrual periods (ISTH-BAT score 1) and a history of a hematoma of the left thigh following an injury (ISTH-BAT score 1). The patient’s total ISTH bleeding score was 8 (normal range is <4 in adult males, <6 in adult females and <3 in children). Her family history was significant for easy bruising and frequent nosebleeds in her mother. The patient had no siblings or children. The only medication the patient was taking was levothyroxine (Synthroid) and her TSH was normal. She was not taking antiplatelet medication or over the counter medications. Due to her history of increased mucocutaneous bleeding symptoms, perioperative bleeding requiring blood transfusion, high ISTH bleeding score and family history she underwent laboratory testing in March 2008 which included a CBC with platelet count, peripheral blood film, prothrombin time (PT), activated partial thromboplastin time (aPTT), von Willebrand
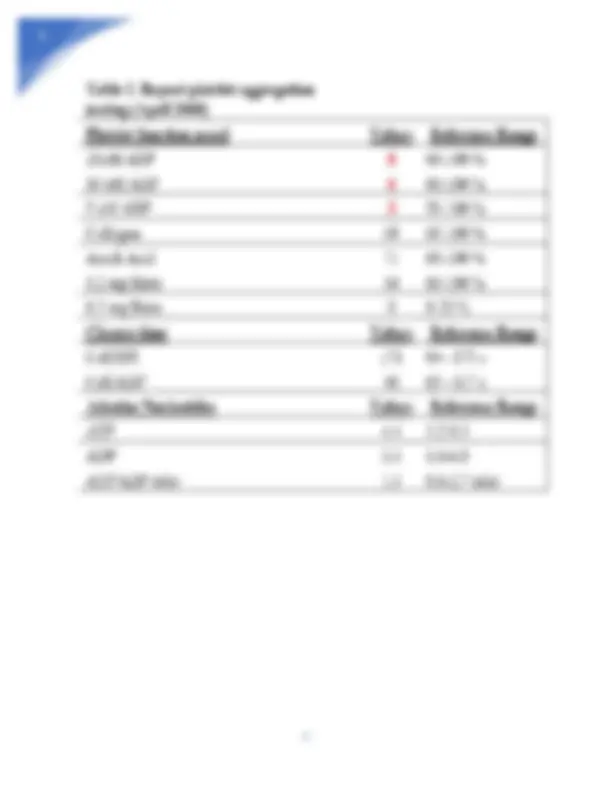
profile and closure times with collagen/ADP and collagen/EPI, all of which were normal. Platelet aggregation studies by light transmittance aggregometry on platelet rich plasma were abnormal with ADP only (Table 1). Repeat platelet aggregation studies in April 2008 (Table 2) demonstrated persistent abnormalities on platelet aggregation studies with ADP only, but adenine nucleotide testing for delta-storage pool deficiency was normal. Following persistent abnormalities on platelet aggregation studies, the diagnosis of a platelet function defect was rendered, however whether the disorder was inherited or acquired was not discernible. She had no spontaneous bleeding and was not planning any surgeries. She was recommended to be reevaluated prior to surgeries in the future. In January of 2024, the patient returned for care with an anticipated fistulectomy and hip replacement in the future. Her previously diagnosed hypothyroidism was well controlled, and she denied any episodes of spontaneous bleeding. Of note, the patient underwent an incision and drainage for a perianal abscess and recovered successfully without any post-operative bleeding complications. Due to her anticipated need of multiple surgical procedures and her history of qualitative platelet dysfunction, she was referred to hematology. Repeat platelet aggregation study results were similar to those previously done in 2008 with decreased platelet aggregation response to ADP only (Figure 1) and adenine nucleotide ratio was again normal. Patient samples were sent for platelet granule storage and release testing by flow cytometry (Table 3).
Figure 1. Platelet Aggregation Studies (2024) Interpretation Comment: Platelet granule storage and release test by flow cytometry demonstrated significantly decreased both delta and alpha granule release upon stimulation with thrombin receptor agonist (decreased mepacrine TRAP ratio and decreased CD62P TRAP %) and adenosine diphosphate (decreased mepacrine ADP ratio and decreased CD62P ADP %). Delta granule adenine nucleotide storage was normal when tested by mepacrine
minor injuries. These symptoms differ from disorders of secondary coagulation which normally occur due to a lack of coagulation factors; these patients can also present with petechiae and easy bleeding, but presence of bleeding into joints (hemarthrosis) is the main differentiating symptom. ISTH-BAT can help decide which patients may need to undergo laboratory testing. Once a bleeding history has been established, clinicians often will obtain multiple sequential studies to verify an abnormality of primary hemostasis or coagulation. The clinician should order a CBC with platelet counts and peripheral blood film, prothrombin time (PT) and activated partial thromboplastin time (aPTT). Additionally, von Willebrand panel may be ordered when there is a concern for vWD, Complete metabolic panel (CMP) can also be a useful initial test as these studies can rule out metabolic causes of platelet dysfunction such as uremia, renal failure or liver disease. These tests are helpful in identifying quantitative platelet disorders, however they are limited beyond initial screening, as patients with qualitative platelet function disorders often show platelet counts within the normal limits. Platelet function testing with platelet function analysis (PFA-100), platelet aggregometry and adenine nucleotide testing should be performed next. PFA-100 is a platelet function test that emulates in vitro primary hemostasis by passing blood through a collagen/ADP or collagen/EPI cartridge lined with collagen and measures the time is takes a sample to form a clot. The PFA- 100 is a rapid test and is easy to use, making it easy for most labs to perform this test and provide prompt results. However, PFA-100 is not sensitive to platelet secretion defects and there is scarce data on its overall sensitivity and specificity in the setting of complex bleeding disorders. Platelet aggregometry is a technique that can evaluate platelet aggregation by exposing the patient’s platelets to a variety of agonists such as ADP, collagen, ristocetin and arachidonic acid.
Platelet aggregometry can be performed on either whole blood or platelet rich plasma. After the sample is exposed to an agonist, the platelets will aggregate and the amount of light that can be transmitted through the sample will increase (Figure 2) and aggregation tracing is recorder as classic biphasic aggregation (Figure 3). The benefit to platelet aggregometry it is sensitive to antiplatelet therapy and can investigate different platelet pathways. Additionally, results from platelet aggregometry are available typically within 24 hours, providing rapid turn-around time for diagnosis and patient management. However, this test is only performed in specialized coagulation laboratories, requires manual sample processing and thus is very time consuming and labor intensive. Additionally, fresh samples are required, which can make this test practically challenging in the laboratory setting and thus it is a poorly standardized test. Aggregometry is not sensitive for detection of some platelet disorders such as granule storage and release deficiencies. Aggregometry is often used in the research setting as the conditions need to be carefully controlled and thus does not always resemble in vivo conditions. Another downside to platelet aggregation testing is that the test is insensitive to platelet pool deficiencies, as seen in this case. Adenine nucleotide testing is a third method of platelet function testing. Adenine nucleotide testing is only moderately sensitive to delta storage pool issues and cannot assess platelet granule release upon platelet stimulation. Neither aggregometry nor adenine nucleotide testing can produce reliable results in patients with thrombocytopenia.
Figure 3. Platelet Aggregometry, Percent Aggregation vs Time While the previously mentioned tests offer the ability to support the diagnosis of a platelet function disorder, they are relatively non-specific and cannot render a definite diagnosis. Two advanced laboratory techniques that can be utilized to diagnose the underlying platelet disorder are flow cytometry and electron microscopy. Flow cytometry has a higher sensitivity than the previously discussed platelet aggregometry tests, especially in the setting of thrombocytopenia. Flow cytometry analyzes single cells, such as platelets, as they flow past either one laser or multiple lasers in a buffered solution. As visible light passes through each cell, it will scatter and the way in which the light scatters will vary based on the internal granularity of the cell (Figure 4). Flow cytometry can detect platelet activation by assessing for expression of surface proteins GIIb/IIIa and P-selectin. Flow cytometric mepacrine fluorescence can be utilized to rule out granule deficiency without the need of a specialized lab. This test can measure dense granule
adenine nucleotide storage as well as release of both alpha and delta granules upon platelet stimulation. Flow cytometry is highly sensitive for detection of platelet granule storage and release issues and can produce reliable results for adenine nucleotide storage in thrombocytopenic patients. Unremarkable flow cytometry results can effectively rule out delta granule deficiencies, whereas the previously mentioned tests cannot. These factors make flow cytometry an ideal assay to aid in the diagnosis of platelet granule deficiencies. While flow cytometry is an esoteric test that is low cost and offers a great deal of information, currently the gold standard for diagnosing platelet pool disorders is electron microscopy. Electron microscopy (EM) consists of three different tests. Whole mount EM is used to quantify granules, platelet thin section EM is used to visualize ultra-structures such as alpha and dense granules, finally buffy coat EM is used to examine aberrant inclusion in platelets. While EM can provide a definitive diagnosis, the turnaround time to obtain the results is typically several weeks which can delay care and may not be practical if a patient has a time sensitive diagnosis and requires prompt treatment. Recent advancements in genetic testing have allowed investigators to determine if there are defects in megakaryopoiesis resulting in an inherited platelet disorder. There are over 50 genes that are associated with inherited platelet disorders that can be detected through genetic testing. The tests are practical as only a small amount of blood is needed; however turnaround time is slow, and the results must be interpreted cautiously to avoid over interpretation.
150,000/ul. Platelet counts can drop below the 150,000 ul level when there is decreased production of platelets or increased consumption. Qualitative platelet disorders can either be acquired or inherited. There are a multitude of etiologies that lead to an acquired platelet disorder, the most common being medications, liver disease, renal failure, myelodysplastic syndrome and myeloproliferative syndrome. Treatment for acquired platelet disorders is targeted at correcting the underlying problem. Inherited platelet disorders (IPDs) can be categorized into one of two main groups: inherited platelet number disorders (IPND) or inherited platelet dysfunction disorders (IPFD). Figure
5. Schematic depicting the differential diagnosis of inherited platelet disorders.
The differential diagnosis for inherited platelet function disorders would include disease of platelet membrane defects (i.e. Glanzmann’s thrombocytopenia, Bernard-Soulier syndrome, etc) and defects of platelet granules (i.e. Chediak-Higashi syndrome, Hermansky-Pudlak syndrome, Grey Platelet Syndrome, α and delta granule release deficiency, etc). Platelets contain three major granules: α-granules, dense granules (d granules) and lysosomes. α-granules contain fibrinogen, vWF, factor V and VIII, platelet derived growth factor (PDGF), platelet factor 4 and P-selectin (CD62P). α-Granule exocytosis is evaluated primarily by plasma membrane expression of P-selectin (CD62P) by flow cytometry. Interestingly, the α-granules are basophilic, and the absence of these granules can be visualized on peripheral smear and aid in the diagnosis of Grey Platelet Syndrome, where there is an absence of α-granules. The Dense (d) granules contain ADP, ATP, calcium, serotonin, epinephrine and CD63/LAMP3. Dense granule storage of adenine nucleotides in resting platelets and release of adenine nucleotides in stimulated platelets can be evaluated by flow cytometry through measurement of fluorescent signal from the compound mepacrine that binds adenine nucleotides when exposed to living platelets. α and dense-storage pool diseases are platelet pathologies that lead to bleeding symptoms that range in severity. Platelet granulogenesis and granule exocytosis are thought to be regulated by SNARE proteins, whose physiologic role is to provide enough mechanical energy to facilitate membrane fusion. Defective SNARE mediated exocytosis provides a possible explanation for the underlying pathophysiology of granule release disorders. The multifaceted pathway of granule formation and release makes the diagnosis of these disorders complex and requires the development of a standardized testing protocol. Treatment
Conclusion The patient’s history of easy bleeding, frequent nosebleeds, heavy menses and excessive bleeding after surgery in the setting of a positive family history of bleeding is concerning for a bleeding disorder. Clinically, her symptoms represent that of a primary bleeding disorder, rather than a secondary bleeding disorder as there is no significant history of bleeding into joint spaces. To optimize healthcare costs and provide high quality patient care without unnecessary testing, a systematic approach to diagnosing hereditary platelet disorders is required. The ISTH-BAT is a screening tool that can be used to assess for the presence of a platelet function disorder. In this patient’s case, the ISTH-BAT score was high at 8. Once a clinical suspicion of a platelet function disorder is established, further testing is required to determine the underlying cause. A quantitative platelet disorder was ruled out by use of a complete blood count (CBC) that indicated a normal platelet count. Platelet aggregation studies identified dysfunctional aggregation with ADP to help confirm a qualitative platelet function disorder, however there are limitations as not all hereditary platelet disorders can be detected by platelet function testing. If the initial tests cannot provide a diagnosis, then more advanced testing such as flow cytometry should be performed. The patient samples were sent for platelet granule storage and release testing via flow cytometry which identified a decrease in both delta and alpha granule release upon stimulation with thrombin receptor agonist and adenosine diphosphate. With anticipated surgical procedures in the future, these results will allow hematologists and surgeons to better manage excess bleeding during and after surgical procedures. Additional studies to consider for further testing would include electron microscopy (EM) and genetic testing as this would provide a definitive diagnosis.
References
- Dupuis A, Bordet J-C, Eckly A, Gachet C. Platelet δ-Storage Pool Disease: An Update. Journal of Clinical Medicine. 2020; 9(8):2508. https://doi.org/10.3390/jcm
- Elbatarny M, Mollah S, Grabell J, Bae S, Deforest M, Tuttle A, Hopman W, Clark DS, Mauer AC, Bowman M, Riddel J, Christopherson PA, Montgomery RR; Zimmerman Program Investigators, Rand ML, Coller B, James PD. Normal range of bleeding scores for the ISTH-BAT: adult and pediatric data from the merging project Haemophilia. 2014 Nov;20(6):831-5. doi: 10.1111/hae.12503. Epub 2014 Sep 6.
- Gross PL, Lopez JA. Acquired disorders of platelet function. In: Hoffman R, Benz EJ, Silberstein LE, et al, eds. Hematology: Basic Principles and Practice. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 128.
- Kirchmaier CM, Pillitteri D. Diagnosis and Management of Inherited Platelet Disorders. Transfus Med Hemother. 2010;37(5):237-246. doi: 10.1159/000320257. Epub 2010 Sep
- PMID: 21113246; PMCID: PMC2980508.
- Lowe G, Hayward C. Inherited platelet function disorders (IPFDs). UpToDate 2023. Available from https://www.uptodate.com/contents/inherited-platelet-function-disorders- ipfds?search=inherited%20platelet%20function%20disorders&source=search_result&sel ectedTitle=1%7E150&usage_type=default&display_rank=1#H
- Orsini, Sara et al. “Bleeding risk of surgery and its prevention in patients with inherited platelet disorders.” Haematologica vol. 102,7 (2017)
- Palma-Barqueros V, Revilla N, Sánchez A, Zamora Cánovas A, Rodriguez-Alén A, Marín-Quílez A, González-Porras JR, Vicente V, Lozano ML, Bastida JM, Rivera J.
- Rumbaut RE, Thiagarajan P. Platelet-Vessel Wall Interactions in Hemostasis and Thrombosis. San Rafael (CA): Morgan & Claypool Life Sciences; 2010. Chapter 4, Platelet Aggregation. Available from: https://www.ncbi.nlm.nih.gov/books/NBK53449/
- Sharda A, Flaumenhaft R. The life cycle of platelet granules. F1000Res. 2018 Feb 28;7:236. doi: 10.12688/f1000research.13283.1. PMID: 29560259; PMCID: PMC5832915.
- Sharma P, Sachdeva MUS, Kumar N, Bose S, Bose P, Uppal V, Malhotra P, Bansal D, Varma N, Ahluwalia J. A comparative study between light transmission aggregometry and flow cytometric platelet aggregation test for the identification of platelet function defects in patients with bleeding. Blood Res. 2021 Jun 30;56(2):109-118. doi: 10.5045/br.2021.2020232. PMID: 34187944; PMCID: PMC8246037.
- Shen CL, Wu YF. Flow cytometry for evaluating platelet immunophenotyping and function in patients with thrombocytopenia. Tzu Chi Med J. 2022 Jul 26;34(4):381-387. doi: 10.4103/tcmj.tcmj_117_22. PMID: 36578648; PMCID: PMC9791859.
- SUPPLEMENTARY MATERIAL TO THE OFFICIAL COMMUNICATION OF THE SSC (LAST REVISION: 19 JULY 2011) isth-ssc_bleeding_assessment.pdf
- Trampuš-Bakija A, Jazbec J, Faganel-Kotnik B. Platelet lumiaggregation testing: Reference intervals and the effect of acetylsalicylic acid in healthy adults. J Med Biochem. 2020 Oct 2;39(4):422-427. doi: 10.5937/jomb0-24690. PMID: 33312057; PMCID: PMC7710376.
- van Asten I, Blaauwgeers M, Granneman L, Heijnen HFG, Kruip MJHA, Beckers EAM, Coppens M, Eikenboom J, Tamminga RYJ, Pasterkamp G, Huisman A, van Galen KPM, Korporaal SJA, Schutgens REG, Urbanus RT. Flow cytometric mepacrine fluorescence
can be used for the exclusion of platelet dense granule deficiency. J Thromb Haemost. 2020 Mar;18(3):706-713. doi: 10.1111/jth.14698. Epub 2019 Dec 27. PMID: 31815339; PMCID: PMC7065135.