Download Endocrine System Summary Pancreas, Thyroid, Parathyroid, Adrenal & Pituitary Glands | H and more Study notes Clinical Medicine in PDF only on Docsity!
Endocrine System Summary – Pancreas,
Thyroid, Parathyroid, Adrenal & Pituitary
Glands | Hormone Functions, Feedback
Loops & Metabolic Effects | Full Clinical
Guide (2024–2025)
The Pancreas and Insulin The normal blood glucose in the body is 4-6mM and is controlled by pancreatic hormones insulin and glucagon.
- It is important to control these as certain organs like the brain can only use glucose as a respiratory substrate.
- Normally glucose –> broken down by glycolysis –> enters Krebs cycle –> oxidative phosphorylation. Some cells can also metabolize fat. This produces reduced FAD/NAD which enter oxidative phosphorylation. But some organs like the brain cannot break down fat and instead use ketone bodies which are made in the liver. These ketone bodies are an alternative fuel source – They are Acetone, Acetoacetate and B-hydroxybutyrate. - Acetyl CoA + Acetyl CoA –> Acetoacetic CoA –> HMG-CoA –> Acetyl CoA + Acetoacetic CoA Insulin This is a peptide hormone which is synthesized in the b-cells in the islets of Langerhans in the pancreas.
- When blood glucose increases, more glucose enters the cells through GLUT2 channels –> more glycolysis occurs –> increase in cell ATP
- ATP binds to KATP channels (which is attached to sulphonylurea receptor) closing them –> leads to cell depolarisation
- Voltage gated Ca2+^ channels open –> increase in exocytosis of insulin. There are many factors which affect insulin release in the body: i) Cephalic phase – parasympathetic stimulation (using Ach) of Beta-cells promotes anticipatory insulin release before consuming a meal ii) Blood glucose – insulin levels rise if [glucose] > 5mM iii) Incretins – GIP and GLP-1 are stomach hormones released in response to oral glucose. These stimulate insulin release and inhibit glucagon. These are broken down by enzyme dipeptidyl peptidase 4 (DPP-4) iv) Sympathetic stimulation – it inhibits insulin release, allowing blood glucose to increase in exercise.
Glucagon On the other hand, glucagon is produced by the a-cells in the islets of Langerhans. It works to blood glucose and fatty acids, acting as the main catabolic hormone of the body Release : It is produced by the pancreas when concentration of insulin and glucose in the bloodstream falls too low.
- Stimulated by hypoglycaemia and adrenaline but inhibited by insulin and hyperglycaemia Actions : It promotes gluconeogenesis and glycogenolysis in the liver raising free blood glucose
- Decreases fatty acid synthesis + promotes lipolysis in liver and adipose for use by skeletal muscle
Thyroid and Parathyroid
Thyroid Gland
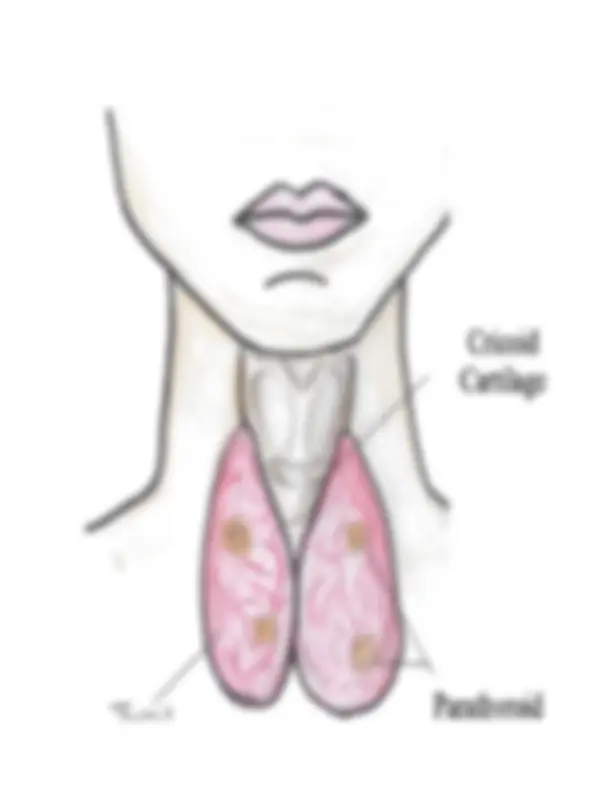
The thyroid gland is an endocrine gland in the neck. It is made of two lobes joined together by an isthmus. It is made up of two types of cells which control metabolic rate and calcium levels in the body. a) Parafollicular cells
- Secrete Calcitonin, which antagonizes effects of PTH
- Decreases plasma [Ca2+] by decreasing bone breakdown by inhibiting osteoclasts whilst promoting osteoblasts b) Follicular cells
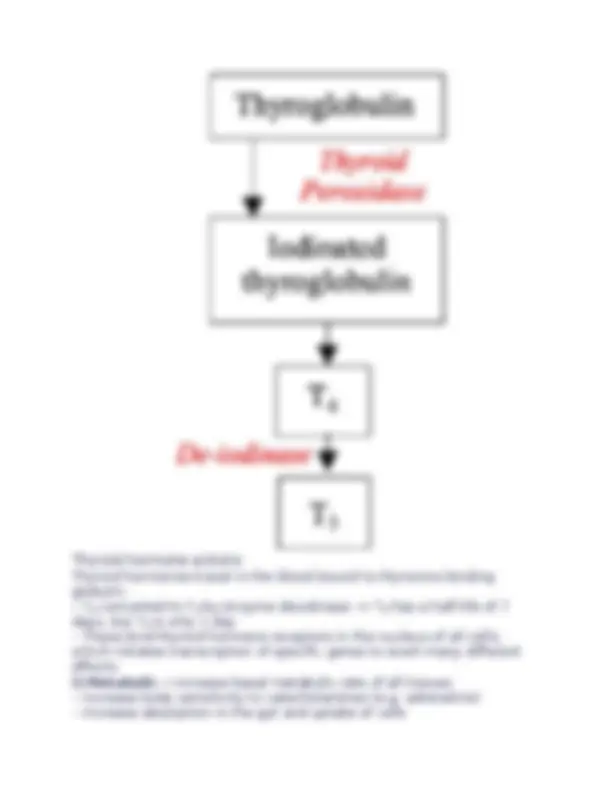
- Produce thyroid hormones, triiodothyronine (T3) and thyroxine (T4) – tyrosine based hormones partially composed of iodine.
- Mainly produces T 4 which is 5x less active than T 3 – 85% of T 3 is made from peripheral conversion of T 4
- Control of synthesis is from the hypothalamus via the HPT axis.
- T 3 exerts short and long negative feedback loops self-regulating release.
Thyroid hormone actions
Thyroid hormones travel in the blood bound to thyroxine binding globulin.
- T 4 converted to T 3 by enzyme deiodinase –> T 4 has a half-life of 7 days, but T 3 is only 1 day
- These bind thyroid hormone receptors in the nucleus of all cells, which initiates transcription of specific genes to exert many different effects: i) Metabolic – Increase basal metabolic rate of all tissues
- Increase body sensitivity to catecholamines (e.g. adrenaline)
- Increase absorption in the gut and uptake of cells
Parathyroid gland The Parathyroid Glands are 4 tiny glands that are located behind the thyroid in the anterior mediastinum. Function : Maintain the body’s calcium and phosphate levels
- This is achieved through the secretion of Parathyroid Hormone (PTH) Release : Secreted in response to decreased plasma Calcium Actions : PTH acts on the bone and the kidney.
- Increases [Calcium] by stimulating bone resorption by osteoclasts and reabsorption by kidney.
- Causes a net decrease in Phosphate by increasing phosphate excretion by kidney despite bone resorption.
Regulation of calcium homeostasis
The kidney also regulates calcium, which is important as it makes bones and affects resting membrane potential.
- This is because Calcium stabilizes sodium channels on the cell membrane decreasing their excitability
- A decrease in calcium reduces threshold for action potentials – increases excitability of neurons.
- Free [Ca2+] extracellular = 1mM, intracellular = 0.1mM Calcium cocentration is regulated by 3 hormones: 1) Parathyroid hormone :
- PTH is secreted by the parathyroid glands in the neck
- Acts to raise plasma [Ca2+] and lower [Phosphate]
- Has actions both on bone and the kidneys
3) Calcitonin: This is secreted by the parafollicular cells of thyroid cells
- Inhibits osteoclast activity favouring osteoblast activity
- Acts to decrease ECF free [Ca2+], antagonizing PTH and 1,25-DHCC
- It is important during pregnancy to protect maternal bone and lactation
Hypercalcemia:
- Usually due to hyperparathyroidism and malignancy (bony metastasis)
- Raised Ca2+^ decreases excitability of cells
- Classically leads to groans (lethargy, pain)
- stones (calcium deposits) + psychiatric moans
- First line treatment is to administer fluids
Hypocalcemia:
- Most commonly due to hypoparathyroidism
- This increases excitability of cells giving signs:
e.g. Trousseau sign – inflating cuff above systolic BP –> reflex muscle
contraction
Chvostek sign – tap on zygomatic bone –> twitching of facial muscle as
it is more excitable
Adrenal Gland
The adrenal gland is split into the adrenal medulla and the cortex, which itself is subdivided into 3 sections. The glands are found above the kidneys and are supplied by superior, middle and inferior adrenal arteries.
Medulla
This is at the center of each adrenal gland.
- Made up of chromaffin cells producing noradrenaline (20%) and
adrenaline (80%)
- Driven by sympathetic preganglionic fibres which synapse in medulla
- Considered a specialized sympathetic ganglion which releases secretions into the blood. Cortex This is the outermost layer of the adrenal gland which is split into 3 zones: i) Zona glomerulosa This is the outermost zone of the adrenal cortex.
- This is responsible for the production of aldosterone, a mineralocorticoid, which is made by the enzyme aldosterone synthase.
Cortisol Cortisol synthesis is stimulated by the release of corticotrophin- releasing factor from the hypothalamus.
- Stimulates production of ACTH from anterior pituitary gland
- This acts on the adrenal cortex to directly stimulate cortisol synthesis and some mineralocorticoid release. Cortisol exerts its effects by binding the glucocorticoid receptor within nuclei and causing transcription of specific genes. Metabolic actions: i) Counters insulin – increases gluconeogenesis and decreases uptake by fat/muscle increasing blood glucose ii) Increases protein breakdown and reduces protein synthesis
Immune Actions: i) Decreases T and B cell proliferation ii) Decreases production of inflammatory cytokines IL-12 and TNFa iii) Increases production of anti-inflammatory cytokines IL- iv) Switches from Th1 –> Th2 response Other actions: Cortisol also changes one’s mood and suppresses reproductive function.
- Inhibits bone formation and collagen synthesis in the skin and stimulates gastric acid secretion Because the steroid has these actions, prolonged exposure to steroids has a number of side effects. Side Effects of Cortisol
The Pituitary Gland
The pituitary gland is one of the most important endocrine glands in the body. It interacts with the hypothalamus which stimulates the production of hormones from the pituitary. It is split into 2 parts:
Posterior pituitary
This is a down-growth of the brain contained within the blood brain barrier which releases 2 hormones: a) ADH This controls the water content on the body by influencing water reabsorption from collecting duct.
- Binds V1 receptors on artieroles (vasoconstriction) + V2 receptors on collecting duct
- N.B. Ethanol inhibits ADH secretion, explains why you need to urinate (“Break the seal”) b) Oxytocin This is responsible for the milk ejection reflex; acts in the mammary glands to release milk
- Uterine contractions; important for cervical dilation before
Anterior pituitary
This lies outside the blood brain barrier and is made up of hormone producing cells. It is stimulated by hormones released into the portal blood circulation and then it releases hormones into the blood stream. i) TSH:
iii) Prolactin: Secretion is stimulated by PRF (prolactin releasing factor)
- Secretion is inhibited by tuberoinfundibular (TIDA) dopamine neurons
- Causes enlargement of mammary glands during pregnancy
- Stimulates mammary glands to produce milk and plays an important role in maternal behavior.
- Contributes to pulmonary surfactant synthesis and neurogenesis iv) FSH/LH: These sex hormones act on the testes and ovaries
- This results in sexual maturation by forming testosterone and estrogen. - Regulated by GnRH secretion from the hypothalamus which is produced in quantities during puberty.
Males : FSH binds Sertoli cells whereas LH binds Leydig cells.
- In puberty, FSH stimulate primary spermatocytes to undergo meiosis, to form secondary spermatocytes.
- LH increases testosterone which responsible for secondary characteristics and sperm production.
Females : FSH initiates follicular growth whereas LH triggers ovulation.
v) Growth hormone This is a hormone which is secreted by somatotrophs in response to hypoglycaemia, low free fatty acids and high amino acids.
- Secretion stimulated by GnRH produced by the hypothalamus
- Secretion inhibited by somatostatin produced by delta cells of pancreas – this inhibits GH and TSH from the pituitary and release of VIP + glucagon + insulin from pancreas. It has many effects both on metabolism and growth: Metabolic – Stimulates gluconeogenesis and lipolysis
- Reduces glucose uptake from fat and muscle raising blood [glucose]
- Increases protein synthesis and conversion of T 4 –> T 3
Growth – It acts by stimulating production of IGF-1 in the target
tissues.
- It stimulates osteoblast and chondrocytes to promote bone growth.
- Insulin is a permissive factor – hence you do not grow in starvation.