Download Final Study Guide Compressed & Revised/Final Study Guide Compressed & Revised. and more Exams Health sciences in PDF only on Docsity!
Family theory: be able to identify a family developmental stage by a description. Family theory: be able to identify a family developmental stage by a description. Stage 1: Beginning family- Married couple establish home but no children Developmental Tasks : Establishing a satisfying home and marriage relationship and preparing for childbirth Stage 2: Childbearing Family- From birth of 1st child until that child is 2 ½ years old Developmental Task : Adjusting to increased family size and providing a positive developmental environment Stage 3: Family with Preschoolers- Oldest child is between 2 ½ and 6 Developmental tasks (DT): coping with demands on energy and attention with less privacy at home Stage 4: Family with School Children- When oldest child is between ages of 6 and 13 DT : Promoting educational achievement and fitting in with the community of families with school-age children Stage 5: Family with Teenagers- Oldest child is between ages of 13 and 20 DT : Allowing and helping children to become more independent Stage 6: Launching Centre- When oldest child leaves family until the youngest leaves home DT : Releasing young adults and accepting new ways of relating to them; maintaining a supportive home base Stage 7: Empty Nest- From time children are gone till couple retires DT : Renewing and redefining marriage relationship; preparing for retirement years Stage 8: Aging Family- From retirement till death of the marriage partner DT : Adjusting to retirement; coping with death and living alone. Growth/development: Identify normal vs. abnormal development if given a description of patient behaviors. Define the diagnosis and meaning of Autism. ● Jean Piaget— developmental psychologist; cognitive development theories ● Piaget’s Theory: Sensorimotor (0-2 years): Development is driven by motor development; coordination of senses with motor response, sensory curiosity. Language used for demands and cataloging. Object permanence developed. Preoperational (2-7 years): Symbolic thinking, use of proper syntax and grammar to express full concepts. Imagination and intuition are strong, but complex abstract thought still difficult. Conservation developed. Important milestones Age Milestones Newborn ● Vision is highly limited at birth (8-12 inches)
● Fixes on moving objects ● Prefers human face; establishes eye contact around one month of age ● Infant will tend to lay in flexed position; will turn head from side to side ● On horizontal suspension there will be some head sagging, but infant should not be hypotonic ● All primitive reflexes should be present Moro, grasp, rooting, tonic neck, etc. ● Infant should regain birthweight by 2 weeks and grow 30 g/day until 4 months of age ● (birth weight should double at this point) If they are premature, you have to correct for that ● Reacts to voice by one month of age—if child is not reacting, think of hearing loss ● Crying peaks around 6 weeks of age (up to 3 hours per day) 1 month old Reacts to voice, establishes eye contact 2 months old ● Infant is able to differentiate among patterns, colors, and consonants, but due to the baby’s yet-limited ability to communicate, this may be difficult to notice ● Infant should be able to track an object horizontally at 180 degrees—can track to midline ● Head lag should be gone and the head and trunk should be held in the same plane on horizontal suspension ● Social smile ● Will listen to voice and make cooing sounds—cooing is vocal development, not language ● Infant should be able to hold head steady while sitting in lap ● Infant should be able to raise head slightly when laying in prone position— TUMMY TIME!! Increases risk of SIDS if put to bed on stomach 4 months old Recognizes hand ● Infant becomes noticeably more distracted by surroundings ● Infant explores own body, especially hands and mouth ● Sense of proprioception begins to mature ● Infant will begin to recognize emotions in others and may mirror such emotions (sustained social smile & laughing) ● Object permanence has not yet developed, so peek-a-boo will amuse the infant ● Infant should be able to lift head above plane when held in horizontal suspension ● Infant should be able to grasp objects like a rattle and may reach for objects held above him/her
● Monosyllabic babbling –will reflect the inflection of the language that they’re around ● Baby should understand “bye-bye” and may wave 1 year old ( months) ● Say or recognize a few words ● Baby should be able to say or recognize a word other than “mama’ or “dada” ● Cognitive development is particularly nurtured at this period as baby begins to walk and navigate away from caretaker ● Birthweight should have tripled by first birthday; length increased by 50%; head circumference increased by 10 cm ● Baby should be able to stand on his/her own ● Baby is cruising by this point, and is often able to walk, at least with one hand held ● Often able to turn pages of a book—start exposing baby to picture books ● Makes postural adjustment to dressing ● May be able to respond to one step commands such as “give me” ● Tantrums often begin Tantrums lasting longer than 15 minutes or occurring more than 3x/day may reflect underlying medical, emotional or social problems 16 months old ● Follow some commands; indicate wants by pointing ● Classically, child should be able to build a 2 or 3 block tower 3 x baby’s age in years (roughly) ● While vocabulary is typically limited, the child is able to indicate what he/she wants by pointing This is a very important way for the child to communicate until his/her vocabulary expands further ● Child should be walking by 15 months of age, and if often able to run ● Child is often able to crawl up a stair(s) ● Should be able to scribble with a crayon ● Hugs parents and shows high preference to familiar people for comfort Preference towards strangers (i.e., you) for comfort is particularly concerning for potential neglect or abuse May be useful to continue to complete physical exam on parent’s lap for child’s comfort level 18 months old ● Classically, child should be able to build a 4 block tower ● Vocabulary should include at least 10 words and include at least one body part ● Child should be able to run by this point, but it will look bumbly ● Should be able to walk up and down stairs with hands held ● Often will be able to sit on a small, child-sized chair ● Able to kiss parent with a pucker ● Child exhibits self-awareness and may recognize self in mirror
● Should indicate some desires by pointing 2 years old ( months) ● Basic sentence; possessive (“mine”) ● Classically, child should be able to build a 7 block tower ● Child should be able to scribble or copy a circle ● Child should be able to put a very basic sentence together (“Come here”, “want more”); vocabulary begins to expand rapidly age 2 ● Child should begin to use pronouns and possessives ● Rule of thumb: the number of words a child can put together in a sentence roughly corresponds to his/her age (i.e., two words at age 2, three words at age 3, etc.) ● Should be able to jump in place ● Often able to insert small objects into holes ● Classically, by 2 years old, the child should be able to build a 7 block tower ● Linguistic development allows child to relate recent experiences in very simple expressions Vocabulary has usually expanded to 50-100 words and will dramatically increase after ● Should be able to properly use spoon ● Should be able to respond to two-step commands ● Engages in parallel play—two children, together, sitting playing togethe 2 ½ years old (30 months) ● Uses “I” to refer to self; knows name ● Child should understand the word “I” and “me” and use it to refer to himself or herself ● Should be able to respond with name when asked ● Should be able to make horizontal and vertical lines with crayon ● Birthweight should have quadrupled by age 2 ½ ● Child should be able to properly ascend stairs with alternating feet ● Child should be able to stand on one foot ● Child begins to engage in imaginative play, but may have difficulty distinguishing reality from fantasy Big problem when it comes to violence on TV; child could think it is normal or may be scared that the violence could happen towards them ● Tantrums peaks at 2 ½ years of age Child should be able to express themselves through words more but will still continue to have tantrums 3 years old ● Child should know age and sex—unless there are legitimate gender recognition issues ● Speech should be mostly understandable by strangers ● Should be able to count to 3 ● Should be able to recognize at least 3 colors
7 years ● Conservation ● When child develops “conversation”, he/she will know what these two containers still have the same amount of water ● Child who grow up in bilingual environments—linguistic development begins a little slower and tends to speed up and make up for it once they start school o Tend to do better in school and have higher IQ’s Well-child visits:
- Hospital Newborn Exam
- 3-5 days
- 1-3 weeks of age if necessary
- 2 months
- 4 months
- 6 months
- 9 months
- 12 months
- 15 months
- 18 months
- 2 years
- yearly visits ages 3-21 years Autistic Spectrum Disorder (ASD)— complex neurobiological and neurodevelopmental disorder characterized by patterns of delay and deviance in the development of social, communicative, and cognitive skills that arise in the first years of life ● ASD is characterized by two diagnostic domains: Deficits in social communication and interaction across multiple contexts Restrictive, repetitive patterns of behaviors, interests, and activities Patients must show symptoms from early childhood even if the symptoms are not recognized until later in life Screening is done with The Modified Checklist for Autism in Toddlers (M-CHAT) ● Development is uneven with talent in a limited area, such as music or mathematics ● Certain genetic disorders (fragile X syndrome, neurofibromatosis, tuberous sclerosis, Angelman syndrome, and Rett syndrome) are often associated with ASD Many autistic children will have other impairments, such as sleep problems, gastrointestinal problems (diarrhea, constipation, and abdominal pain), and irritability Risk factors for ASD: A critical period before, during, and immediately after birth Maternal ingestion of valproic acid and thalidomide during pregnancy Children born to older parents Children with certain genetic or chromosomal conditions, such as fragile X syndrome or tuberous sclerosis Can also include prenatal infections, neonatal infections, untreated phenylketonuria, prematurity, or twin and multiple pregnancy Red flags for autism:
Does not respond to his or her name by 12 months old Does not point at objects to show interest (pointing at an airplane flying over) by 14 months old Does not play “pretend” games (pretending to “feed” a doll) by 18 months old Avoid eye contact and wants to be alone Has trouble understanding other people’s feelings or talking about their own feelings Has delayed speech and language skills (no babbling or gesturing by 12 months old; no single words by 16 months old; no two-word [not echolalic] phrases by 24 months old) Repeats words or phrases over and over (echolalia) Gives unrelated answers to questions Gets upset by minor changes Has obsessive interests Flaps their hands, rocks their body, or spins in circles Has unusual reactions to the way things sound, smell, taste, look, or feel Fails to meet childhood developmental milestones Has a sibling with autism Has loss of any language or social abilities at any age Genetics: be able to recognize the signs of the common genetic disorders.
Disorder Physical characteristics Developmental
characteristics
Cause/ Diagnosis
Downs
Syndrome
*Most
common
cause of
moderate
MR
*associated
with ↑ in
maternal
age
*3 copies of
chromosom
e 21 due to
non-
disjunction
Flat face Upward slanted palpebral fissures Small ears Epicanthal fold Simian crease Protruding tongue Short neck Hypotonia, decreased moro reflex Obesity Issues with expressive language Some degree of developmental delay in all, may be high-functioning though Self-help skills delayed Alzheimer’s usually prenatal testing 1st trimester: fetal nuchal translucency 2nd trimester: quad screen or triple marker screen formal diagnosis is chromosomal analysis Management: routine care attend to comorbidites peds consult for congenital heart defects peds opthalmologist consult
Turner’s
Syndrome
*Sexual
aneuploidy in
females
(missing x
chromosome
or part of it)
*Most
common single
X chromosome
*Girls are
higher risk for
X chromosome
related genetic
diseases due to
lack of 2nd
*functional X
chromosome
Short stature Congenital lymphedema Webbed neck Scoliosis Colorblindness, cataracts, strabismus Primary amenorrhea (cannot diagnose until age
Delayed thelarche Hypothyroidism Widespread nipples Learning difficulties ADHD Gonadal dysgenesis Heart defects Females only chromosomal analysis 1st trimester: nuchal translucency Triple marker or quad screen CVS or amnio for positive sono or blood Management: routine neonatal sono screen for renal anomalies peds cardio consult for CHD pedi endo for growth management HGH to prevent short stature calcium and vitamin D supplement estrogen therapy at 12-15 to induce secondary sex characteristics Long term: high risk for aortic root dilation treat HTN aggressively diet and exercise can become pregnant with IVF and donor oocyte.
Fragile X Large, protruding ears^ Mental retardation^ Molecular analysis to
Syndrome
*error is on x
chromosome
so males are
more affected
*severity is
related to
mutation.
*error is on x
chromosome
so males are
more affected
Elongated face/ forehead High, arched palate scoliosis Macro-orchidism Hyper-extensible joints Short stature Obesity Autism ADHD Anxiety (esp. social) Gross motor delays- r/t hypotonia Fine motor delays Low IQ Speech and language delays Seizures Premature ovarian failure Early menopause diagnose- prenatally or postnatally prenatal test of amniotic fluid postnatal test with blood screen for heart defects. Most common is MVP. Long term: counseling for discipline and behavior modifications work training and special ed social worker normal life expectancy leads to cognitive/intellectual disability and some psych
Fetal Alcohol
Syndrome
Short palpebral fissure Epicanthal folds Low nasal bridge Flat midface Thin upper lip Smooth philtrum Small eye openings Short nose Microcephaly Growth retardation/restriction -pre and postnatally CNS dysfunction Mental retardation Congenital heart defects Behavioral disturbances ETOH crosses placenta and blood-brain barrier Treatment: intervention before it happens counseling
Klinefelter’s
Syndrome
Small testes and penis Reduced body hair Gynecomastia Need for testosterone replacement Infertility Extra X chromosome- random (not inherited) Karyotyping to
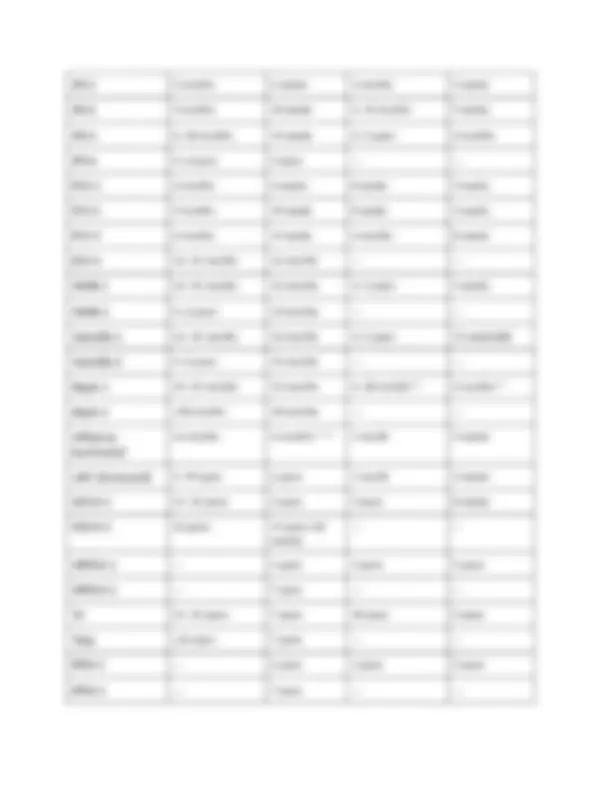
IPV-1 2 months^ 6 weeks^ 2 months^ 4 weeks
IPV-2 4 months^ 10 weeks^ 2--14 months^ 4 weeks
IPV-3 6--18 months^ 14 weeks^ 3--5 years^ 6 months
IPV-4 4--6 years^ 4 years^ ---^ ---
PCV-1 2 months^ 6 weeks^ 8 weeks^ 4 weeks
PCV-2 4 months^ 10 weeks^ 8 weeks^ 4 weeks
PCV-3 6 months^ 14 weeks^ 6 months^ 8 weeks
PCV-4 12--15 months^ 12 months^ ---^ ---
MMR-1 12--15 months^ 12 months^ 3--5 years^ 4 weeks
MMR-2 4--6 years 13 months --- ---
Varicella-1 12--15 months^ 12 months^ 3--5 years^ 12 weeks§§§
Varicella-2 4--6 years^ 15 months^ ---^ ---
HepA-1 12--23 months^ 12 months^ 6--18 months^ 6 months
HepA-2 ≥18 months^ 18 months^ ---^ ---
Influenza,
inactivated
≥6 months 6 months**** 1 month 4 weeks
LAIV (intranasal) 2--49 years^ 2 years^ 1 month^ 4 weeks
MCV4-1 11--12 years^ 2 years^ 5 years^ 8 weeks
MCV4-2 16 years^ 11 years (+
weeks)
MPSV4-1 ---^ 2 years^ 5 years^ 5 years
MPSV4-2 ---^ 7 years^ ---^ ---
Td 11--12 years^ 7 years^ 10 years^ 5 years
Tdap ≥11 years^ 7 years^ ---^ ---
PPSV-1 ---^ 2 years^ 5 years^ 5 years
PPSV-2 --- 7 years --- ---
HPV-1 11--12 years^ 9 years^ 2 months^ 4 weeks
HPV-2 11--12 years (+
months) 9 years (+ weeks) 4 months 12 weeks†††††
HPV-3 11--12 years (+
months) 9 years (+ weeks)
Rotavirus-1 2 months^ 6 weeks^ 2 months^ 4 weeks
Rotavirus-2 4 months^ 10 weeks^ 2 months^ 4 weeks
Rotavirus-3 6 months^ 14 weeks^ ---^ ---
Herpes zoster ≥60 years^ 60 years
o Hep B (3 doses) 0, 2, and no earlier than 6 months If HBsAg + mother- give dose 1 and HBIG at birth If HBsAg unknown mother- give dose 1 at birth and give HBIG within 7 days if mom is tested + o Rotavirus (2-3 doses) 2, 4, 6 months * Live Attenuated Virus* o DTaP (3 doses & 2 boosters) 2, 4, 6 months, 15 months, 4 years o TDaP (1 dose) 11 years, each pregnancy at >20 weeks gestation, adults >65 if contact with infants; age 7 if catch-up needed (Td booster every 10 years) o Hib (3 doses & 1 booster) 2, 4, 6 months, 12 months o PCV-13 (3 doses & 1 booster) 2, 4, 6 months, 12 months; additionally 23-valent can be given at 2 years for chronic illness o IPV (4 doses) 2, 4, 6 months, 4 years
previous dose of DTP/DTaP Persistent, inconsolable crying lasting ≥3 hours within 48 hours after receiving a previous dose of DTP/DTaP GBS <6 weeks after previous dose of tetanus toxoid--containing vaccine History of arthus-type hypersensitivity reactions after a previous dose of tetanus toxoid--containing vaccine; defer vaccination until at least 10 years have elapsed since the last tetanus toxoid--containing vaccine Moderate or severe acute illness with or without fever
DT, Td Severe allergic reaction (e.g., anaphylaxis) after
a previous dose or to a vaccine component GBS <6 weeks after previous dose of tetanus toxoid--containing vaccine History of arthus-type hypersensitivity reactions after a previous dose of tetanus toxoid--containing vaccine; defer vaccination until at least 10 years have elapsed since the last tetanus- toxoid-containing vaccine Moderate or severe acute illness with or without fever
Tdap Severe allergic reaction (e.g., anaphylaxis) after
a previous dose or to a vaccine component Encephalopathy (e.g., coma, decreased level of consciousness, or prolonged seizures), not attributable to another identifiable cause, within 7 days of administration of previous dose of DTP, DTaP, or Tdap GBS <6 weeks after a previous dose of tetanus toxoid--containing vaccine Progressive or unstable neurological disorder, uncontrolled seizures, or progressive encephalopathy until a treatment regimen has been established and the condition has stabilized History of arthus-type hypersensitivity reactions after a previous dose of tetanus toxoid--containing vaccine; defer vaccination until at least 10 years have elapsed since the last tetanus toxoid--containing vaccine Moderate or severe acute illness with or without fever
IPV Severe allergic reaction (e.g., anaphylaxis) after
a previous dose or to a vaccine component Pregnancy Moderate or severe acute illness with or without fever
MMR†,§ Severe allergic reaction (e.g., anaphylaxis) after Recent (≤11 months) receipt of
a previous dose or to a vaccine component Pregnancy Known severe immunodeficiency (e.g., from hematologic and solid tumors, receipt of chemotherapy, congenital immunodeficiency, or long-term immunosuppressive therapy or patients with HIV infection who are severely immunocompromised)§ antibody-containing blood product (specific interval depends on product)** History of thrombocytopenia or thrombocytopenic purpura Need for tuberculin skin testing†† Moderate or severe acute illness with or without fever
Hib Severe allergic reaction (e.g., anaphylaxis) after
a previous dose or to a vaccine component Age <6 weeks Moderate or severe acute illness with or without fever
Hepatitis
B
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component Infant weight <2,000 gm§§ Moderate or severe acute illness with or without fever
Hepatitis
A
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component Pregnancy Moderate or severe acute illness with or without fever
Varicella Severe allergic reaction (e.g., anaphylaxis) after
a previous dose or to a vaccine component Known severe immunodeficiency (e.g., from hematologic and solid tumors, receipt of chemotherapy, congenital immunodeficiency, or long-term immunosuppressive therapy or patients with HIV infection who are severely immunocompromised) Pregnancy Recent (≤11 months) receipt of antibody-containing blood product (specific interval depends on product) Moderate or severe acute illness with or without fever Women’s health Women’s/men’s health: Identify a problem based on symptoms. Contrast normal vs abnormal findings. Plan contraception and know contraindications in hormonal therapies. Female: Amenorrhea- tx of underlying cause (most common is pregnancy) Bartholin gland cysts or abscesses- tx is antibiotics or surgical procedures Breast issues- see answer below. Chronic pelvic pain- many causes, often difficult to diagnose Dysmenorrhea- supportive, NSAIDS/ birth control Dyspareunia is often a result of inadequate vaginal lubrication, OTC or prescription lubricative agents can be useful, as well as education about adequate female arousal prior to intercourse. Benign breast lumps- make up 80% of lumps seen. Risk of cancer correlates with age (younger is less risk, older is more risk- esp. after menopause) Fibroadenoma- benign lump in patient under 30 years old. Solid tumor, palpable, rounded and mobile. 10% spontaneously resolve. US to see best. Increased risk of breast ca later in life.
● Circulating blood volume and number of erythrocytes increase. ● Coagulation factors increase. ● Hemoglobin concentration is diluted but hemoglobin should not go below 11. ● Iron requirements increase—will typically receive an iron supplement. ● Leukocyte counts decrease—the increased risk of infection calls for monitoring for infection Endocrine ● Carbohydrate metabolism undergo changes causing the patient to have changes in blood ● sugar and lipids. Patients have elevations in post-prandial blood sugars and may develop diabetes. ● Patients also become hyperinsulinemic (as a growth factor) and may develop a.m. hypoglycemia. ● The thyroid may be very slightly enlarged but NOT nodular. Pregnancy Progression Fetal Growth ● Uterus ● 70 grams non pregnant ● 1100 grams at delivery ● Uterine Volume ● 10 ccs non pregnant ● 5000 ccs at term Calculating Due Dates Naegeles Rule The EDC (estimated date of confinement) or EDB (estimated date of birth) is usually calculated from the menstrual history. How to calculate:
- The calculation begins with the First day of the last menstrual period
- From this date, go back 3 months
- Add 7 days to the last date Example:
- First day of last menstrual period = March 12.
- Go back 3 months from March 12 = December 12.
- Add 7 days to December 12 = December 19 is the due date Care of the Patient in the 1st^ Trimester ● History and physical ● Management of any chronic diseases ● Education, diet, exercise ● Prenatal vitamin with iron ● Screening for HIV, STI, urinary tract infection, anemia, domestic violence The First Trimester: Red Flags and Common Discomforts: ● Bleeding
● Nausea and vomiting ● Pain: ectopic or threatened abortion First Trimester Bleeding ● Not normal but VERY common. ● Remember that the cervix becomes more vascular in early pregnancy (Chadwick’s sign). ● Intercourse or infection may cause bleeding of this now vascular tissue. ● Bleeding may also result from polyps. ● Spontaneous abortion. Ectopic Pregnancy ● Fertilized egg grows inside the tube or other extra uterine site. ● The growing tissue causes severe pain in the pelvic area. ● Usually seen between weeks 5-10. ● If diagnosed early, the patient may be treated with Methotrexate to stop the growth of fetal tissue. ● Otherwise, the patient will require surgical removal. Nausea and Vomiting ● Common signs in early pregnancy but patient must be assessed for danger signs. ● Assess for urinary ketones and hydration status. ● Liver enzymes may be elevated, indicating hepatitis. ● The provider also must consider pancreatitis and cholecystitis. ● Patients with no organic cause may improve with Phenergan or Zofran. *REMEMBER: Nausea and vomiting after the first trimester must be investigated! The Second Trimester: Red Flags Just FYI—during the second trimester, estrogen causes growth of blood supply of lots of things—moles, warts, gums. Patients may report bleeding gums—they should see the dentist, but you can reassure them about this. Incompetent Cervix ● An incompetent cervix dilates in response to the growing uterine contents. ● This may lead to premature delivery. ● Signs are bleeding, loss of fluids. ● A common procedure is cerclage—the use of suture to hold the cervical os closed. Emergency: Abruptio Placenta ● Occurs when placenta separates prematurely from the uterus. ● Fetus loses part of blood supply. ● Maternal death may occur from hemorrhage.