



1
Comenius University in Bratislava
Jessenius Faculty of Medicine in Martin
Department of Anatomy
HEART AND RESPIRATORY SYSTEM
STUDY GUIDE
Desanka Výbohová
Gabriela Hešková
Yvetta Mellová
Martin 2019

























































































Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
1 / 125

This page cannot be seen from the preview
Don't miss anything!
Comenius University in Bratislava Jessenius Faculty of Medicine in Martin Department of Anatomy
Desanka Výbohová Gabriela Hešková Yvetta Mellová
Martin 2019
Authors: Doc. MUDr. Desanka Výbohová, PhD. MUDr. Gabriela Hešková, PhD. Doc. MUDr. Yvetta Mellová, CSc.
Authors themselves are responsible for the content and English of the chapters.
Reviewers: Prof. MUDr. Marian Adamkov, DrSc. MUDr. Zuzana Lazarová, PhD.
Heart (Cor)
The heart is a hollow muscular organ consisting of four chambers: the right atrium and ventricle, and the left atrium and vetricle. The shape of the heart is usually described as conical or pyramidal and the size of the heart is generally comparable with a fist of a respective human. The average weight of the heart is 230 – 340 g or 0.40 – 0.45% of the total body weight.
The myocardium rhythmically contracts and relaxes and thus pumps the blood throught the heart.
The heart works as two pumps. The left part of the heart pumps the oxygenated blood to the systemic circulation. The right part pumps the deoxygenated blood to the small (lung) circulation.
The period when the chamber of the heart is relaxed and filling with a blood is called a diastole. Contraction of the heart chamber when the blood is ejecting from the chamber is called a systole.
The right atrium of the heart receives the deoxygenated blood of the body. This blood continues into the right ventricle. From the right ventricle the blood is ejected into the pulmonary arteries to reach the lungs where the deoxygenated blood is oxygenating.
The oxygenated blood from the lungs is transported via the pulmonary veins into the left atrium. The blood from the left atrium inflows to the left ventricle and during the contraction (systole) of the left ventricle it is ejected to the aorta and from the aorta via the arteries to the whole body.
Position of the heart
The heart enclosed in pericardium lies in the thoracic cavity - in the mediastinum (the space between the pleural cavities). According the anatomical subdivision of mediastinum, the heart is situated in lower middle mediastinum. However, clinicians usually use easier clinical subdivision of mediastinum and according to this clinical classification the heart is in anterior mediastinum. As for the position of the heart to the median plane , one third of the heart is situated on the right side and two thirds on the left side.
The axis of the heart (imaginary line passing from the base of the heart to the apex of the heart) directs anteriorly, inferiorly and to the left.
Fig. 1 Heart in pericardium in the thorax Anterior view Dissection of formalin-fixed cadaver
Projection to the anterior thoracic wall
Physiologically sized heart is projected to the anterior thoracic wall to the area determined by following borders (lines):
the 2nd^ intercostal space superiorly the 5th^ intercostal space inferiorly right parasternal line (vertical line passing 1.5 – 2 cm beside the right border of sternum) left midclavicular line (vertical line passing through the midpoint of the left clavicle) Traditional chest radiographs or x-rays show the size of the heart very clearly (see fig. 2).
Enlargement of the heart can be caused by the hypertrophy and/or the dilation of the heart. The left side of the heart mainly the left ventricle is the most often enlarged from the arterial hypertension (high arterial blood pressure). The left ventricle have to pump the blood against higher resistence in arterial circulation thus it becomes hypertrophic. The enlargement of the right ventricle usually results from the pulmonary hypertension that is caused by pulmonary diseases. The acute enlargement of the right ventricle (dilation of the right ventricle) usually results from pulmonary embolia. Chronic hypertrophy of the righ ventricle can be caused e.g. by pulmonary fibrosis or bronchial athma. Certain pathological conditions can lead to the enormous enlargment of the heart termed cardiomegaly or „cor bovinum“, when the weight of the heart can increase up to 1 kg. However, the enlarged heart with the weight above 500g is in high risk of myocardial ischemia because usual blood flow in the coronary arteries is insufficient for such enlarged mass of myocardium.
Interestingly, the hearts of the athlets can show „physiological enlargement of the left ventricle“. So called „athlet's heart“ is a result of the endurance excercise training leading to the physiologic growth caused by both hypertrophy and neoformation of cardiomyocytes and concomitant angiogenesis.
Relations of the heart
Each physician should have a perfect knowledge as for the relations of the organs. It is important as for the understanding how the pathological processes (tumour, inflamation) can spread from affected organ to the other surronding ones „per continuitatem“ through surrounding tissue (not by the blood or lymph). The heart is related to the following organs :
recognise what is „own to the human body“ and what is „foreign“. This organ is the largest during the infancy and diminishes after the puberty.
** (^) Phrenic nerve comes from the cervical plexus, runs between the pleura amd pericardium to
supply the diaphragm.
*** (^) Tracheal bifurcation is the lowermost part of the trachea where it subdivides / splits in two
principal bronchi.
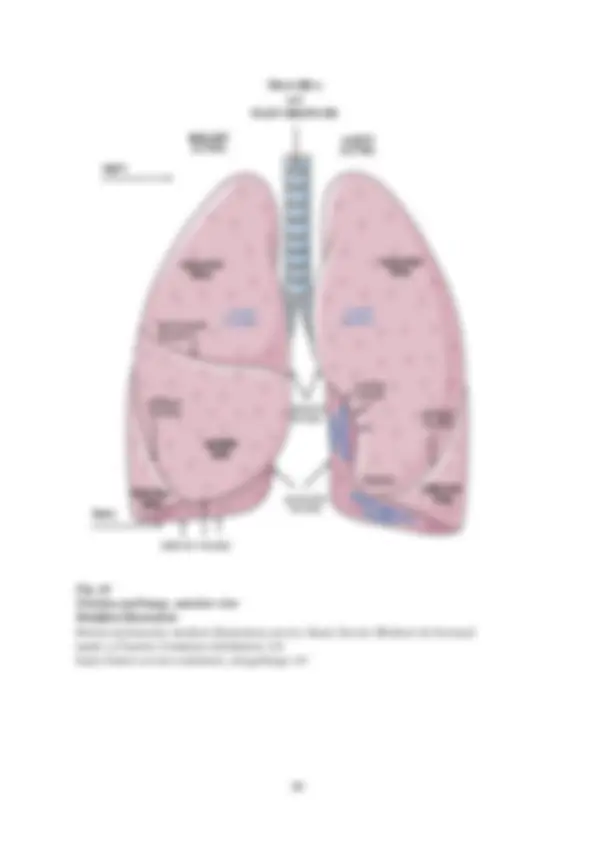
Fig. 4 Heart in pericardium, lungs reflected Anterior view Dissection of formalin-fixed cadaver
Cardiac massage
Rhytmic compressing of the chest also causes the compression of the ventricles and thus the blood is ejected into the great vessels. This procedure can provide some blood flow to the brain and the other organs to reduce the ischemic injuries and postpone the metabolic deterioration.
External features of the heart
The heart has a pyramidal shape with wider dorsocranial part, the base of the heart and anterocaudally situated apex of the heart.
The base of the heart directs superiorly, posteriorly and to the right. It is the area where the large vessels enter and exit the heart. Superior vena cava and inferior vena cava open into the right atrium, pulmonary veins to the left atrium. The aorta comes from the left ventricle, the pulmonary trunk fromt the right ventricle.
The apex of the heart is rounded and directs inferiorly anteriorly and to the left. It is formed by the left ventricle. The apex of the heart is projected to the anterior thoracic wall to the 5th intercostal space in the left midclavicular line. The apex beat can be palpated in this point.
Fig. Base and apex direction. Retrieved from Smart Servier Medical Art Servier Medical Art by Servier is licensed under a Creative Commons Attribution 3. Unported License ttps://smart.servier.com/ smart_image/aneurysm/ Modified
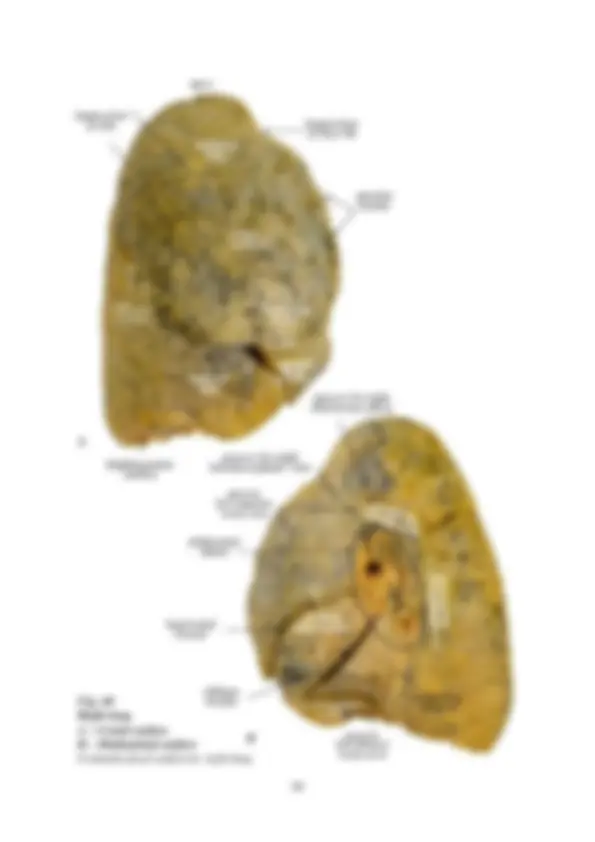
Surfaces of the heart
The definition of the surfaces is not always uniform. Used clinical terminology sometimes differs from the latest version of Terminologia Anatomica 1998. Therefore we review both the anatomical and the clinical terms. External surface of the heart is anatomically subdivided into: sternocostal surface ( clinically „anterior wall of the heart“ ) is slightly convex, related to the thymus sternum and the ribs; it is formed by the right atrium, left auricle, 2/3 of the right ventricle and 1/3 of the left ventricle diaphragmatic surface ( clinically „posterior wall of the heart“ ) is almost flat inferior surface related to the diaphragm; it is formed by 2/3 of the left ventricle, 1/3 of the right ventricle right and left pulmonary surfaces are convex surfaces where the heart touches the lungs at the sides; right pulmonary surface is formed by the right atrium; left pulmonary surface by the left ventricle and a part of left atrium. F
Fig. Sternocostal surface of the hear Sulci and vessels of the heart are not visible because they are covered by epicardial fatty tissue Formalin-fixed cadaveric heart
Fig. The right and left borders recognized at the frontal chest x – ray image
At the frontal chest x – ray images clinicians recognize the right and left borders formed by following marginal structures (see fig.10).:
the right border of the heart (from the top to the bottom): superior vena cava, right atrium the left border of the heart (from the top to the bottom): aortic arch, pulmonary trunk, left auricle, left ventricle
Sulci (grooves) at the surface of the heart
Partitions inside the heart subdivide the heart into 4 chambers. These partitions create the grooves or sulci at the surface of the heart. Sulci of the heart contain the vessels surrounded by epicardial (subepicardial) fat.
Coronary sulcus passes around the heart separating the atria from the ventricles at the surface of the heart. In its right part it contains the right coronary artery and small cardiac
vein. In its left part anteriorly there is the circumflex branch from the left coronary artery. Coronary sinus , large veinous channel, runs posteriorly in the left part of coronary sulcus.
Interventricular sulci overlie the interventricular septum and separate the right and left ventricle at the surface of the heart. Anterior interventricular sulcus runs at the sternocostal surface of the heart. It contains the anterior interventricular branch from the left coronary artery and anterior interventricular vein opening to the great cardiac vein. Posterior interventricular sulcus is situated at the diaphragmatic surface of the heart. Posterior interventricular branch from the right coronary artery and middle cardiac vein run in this groove.
Fig.
Coronary sulcus and anterior interventricular sulcus at the sternocostal surface of the heart occupied by the vessles
Formalin-fixed cadaveric heart
Althought it completely surrounds the heart it is not fixed to it. However, it is firmly attached to surrounding structures:
diaphragm (especially to the central tendon) by pericardiophrenic ligaments sternum b y sternopericardial ligaments tracheal bifurcation by bronchopericardial membrane. These attachments are important for the stabile position of the pericardial sac in the thorax. The fibrous pericardium also covers the roots of large vessels - aorta, superior vena cava, pulmonary arteries, pulmonary veins, but it does not cover inferior vena cava.
The phrenic nerves accompanied by the pericardiacophrenic vessel s pass along the external surface of the fibrous pericardium (see fig. 13).
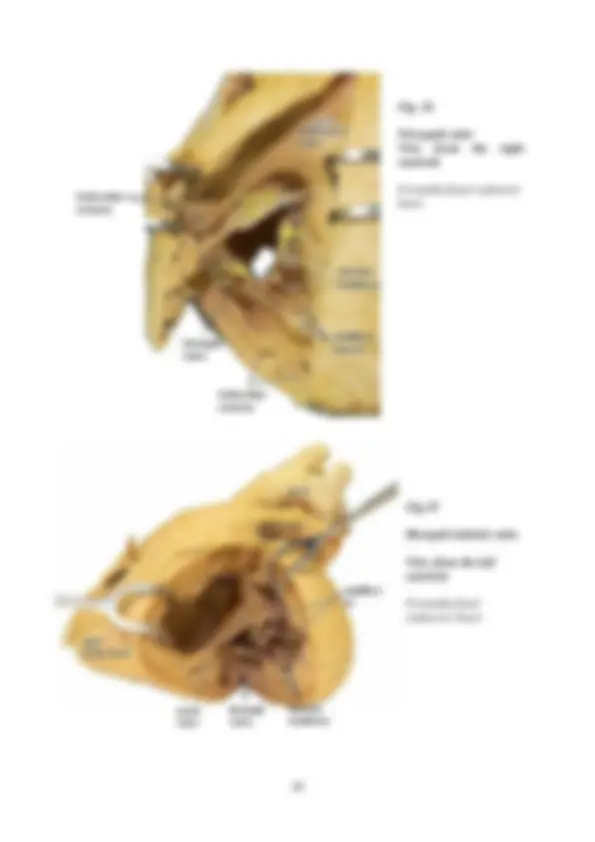
Fig. 14
Heart in pericardium with remains of the sternopericardiac and phrenicopericardiac ligaments. Pericardial cavity closed
Anterior view
Dissection of formalin-fixed cadaver
Fig. 14 Heart in opened pericardial cavity Anterior view Formalin-fixed cadaveric heart
Serous pericardium is a serous membrane formed by mesothelium and arranged in two layers:
parietal layer is connected to the internal surface of fibrous pericardium visceral layer (epicardium) directly covers the surface of the heart. Pericardial cavity is a narrow space between the visceral and parietal layers of the serous pericardium. Cavity contains 10-20 ml of serous pericardial fluid. Pericardial fluid lubricates the layers of serous pericardium to diminish the friction between them when the heart pumps. While the heart is enlarging and diminishing its volume the layers of serous pericardium glide over each other.