Download Hereditary amelogenesis imperfecta and more Lecture notes Dentistry in PDF only on Docsity!
KIUT
DENTISTRY
No. 4.
Hereditary amelogenesis imperfecta.
KIUT
DENTISTRY
Subject : CLINICAL RESTORATIVE DENTISTRY 2 Lecturer : PhD, Associate Professor Khatamov Ulugbek Altibaevich Tashkent 2025
- (^) Hereditary dental tissue developmental
disorders are genetically determined
pathologies affecting the formation of
enamel, dentin, and sometimes
cementum. These disorders can manifest
as a variety of clinical manifestations,
reflecting both quantitative and
qualitative changes in tooth structure.
Main categories of hereditary disorders
- Hereditary amelogenesis imperfecta (HAI) This disease disrupts enamel formation. Clinical manifestations can range from minor defects (reduced tooth size, slight discoloration) to severe enamel thinning with pits, grooves, and shade changes (from yellow to brown). NNA can be inherited in an autosomal dominant, autosomal recessive, or X-linked manner.
- Hereditary dentinogenesis imperfecta (HDI) Disruption of dentin formation leads to a decrease in its mineral content and changes in its structure. This condition can manifest as increased tooth translucency, opalescence (teeth appearing "glassy"), and increased sensitivity to irritants. While caries develops less frequently, teeth are prone to rapid wear.
- Hereditary amelogenesis imperfecta (HAI) is a genetic disorder of dental enamel formation that affects both primary and permanent teeth. The disorder is caused by mutations in genes responsible for enamel synthesis and mineralization (e.g., AMELX, ENAM, KLK4, MMP-20, and DLX3), which lead to disruptions at various stages of enamel formation. The disorder can be inherited in an autosomal dominant, autosomal recessive, or X-linked manner.
- Amelogenesis imperfecta is a genetic disorder of tooth enamel formation that results in structural defects, discoloration, increased sensitivity, and a tendency to decay. This condition can affect both primary and permanent teeth and is often accompanied by aesthetic and functional problems.
Amelogenesis
Amelogenesis imperfecta
Clinical manifestations of NNA are varied and depend on the nature of the enamel apparatus disorder:
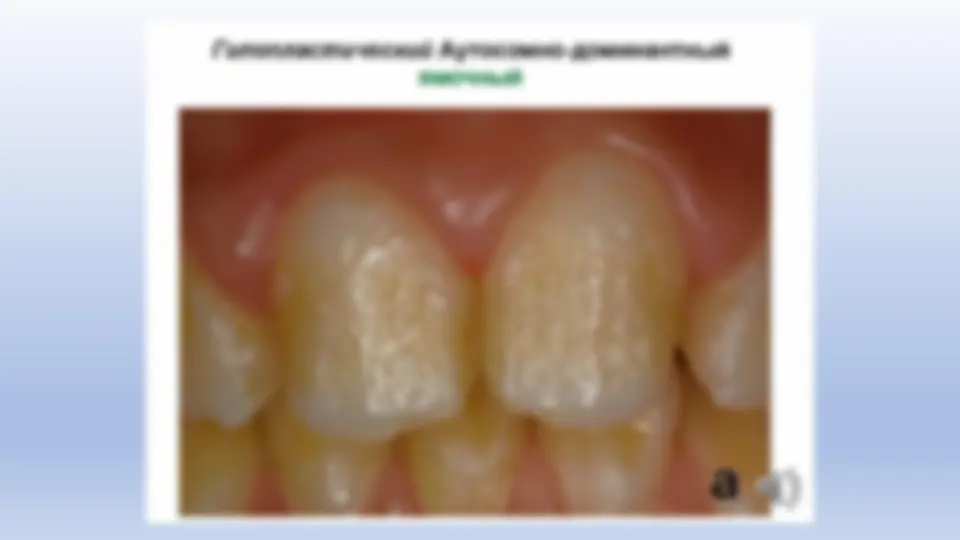
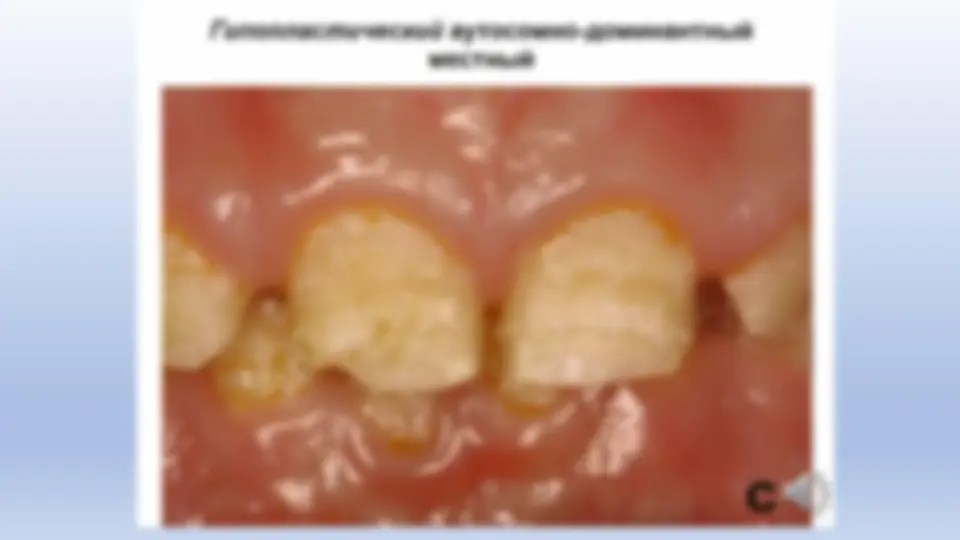
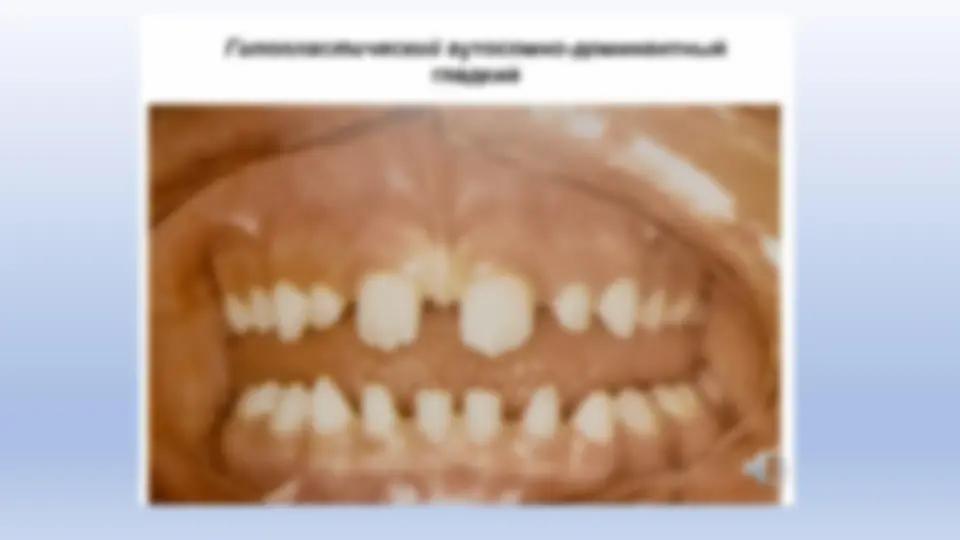
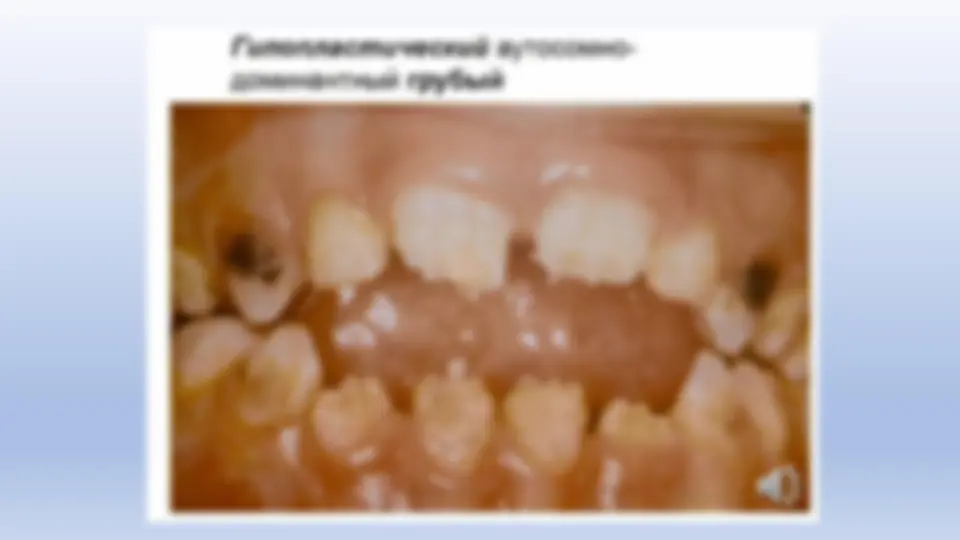
- (^) Hypoplastic form: a decrease in the amount of enamel matrix is observed , leading to thinning of the enamel, the appearance of pits, grooves, and a decrease in the size of the teeth. While the teeth may be normally shaped, gaps often form between them.
- (^) Hypomaturation form: the thickness of the enamel is preserved, but its maturation is disrupted , as a result of which the enamel becomes less strong , acquires a matte or altered shade (from light white to dark brown) and tooth sensitivity increases.
- (^) Hypocalcification form: enamel is formed with normal thickness, but its mineralization is impaired with insufficient calcium content. As a result, the enamel becomes soft, prone to chipping and rapid wear. Combined variants also occur (for example, hypomaturation with hypoplasia and taurodontism ), which further complicates the clinical picture.
Clinical picture
After eruption, the enamel takes on a yellowish and
brownish tint. Microscopically, unevenness of the
enamel-dentin junction and an increase in the amount of
organic matter are revealed.
One to three years after eruption, the enamel becomes
matte, rough, and cracks appear; the color changes to
brown. Dentin is dense and brown.
At the moment of eruption, the enamel is white,
covered with grooves, and quickly disappears, revealing
the dark brown dentin of normal structure.
At the moment of eruption, the enamel is
chalky , matte, absent in places and easily
separated from the dentin under mechanical action.
Patients complain of increased tooth
sensitivity.
Microscopically, dentin has a normal structure,
while the remaining enamel is significantly altered:
the orientation of the prisms is disrupted,
their transverse striations are increased , and
prism-free zones filled with an amorphous
substance are found.