Download ICD-10-CM Codes Eosinophilic-Associated Diseases and more Lecture notes Medicine in PDF only on Docsity!
Request for ICD-10-CM Codes for Eosinophil-
Associated Diseases
Bruce Bochner, MD
Samuel M. Feinberg Professor of Medicine
Northwestern University Feinberg School of Medicine and
President, International Eosinophil Society
Disclosures for Dr. Bochner
- I currently serve as a consultant for Genentech.
- I receive research funding from the NIH and from Acerta Pharma.
- I am the President of the International Eosinophil Society, for which I receive no remuneration.
- I receive publishing royalties from Elsevier and Wolters Kluwer/UpToDate.
- I am a co-founder, own stock in, and serve on the scientific advisory board of Allakos Inc., a
biopharmaceutical company developing antibodies to Siglec-8 for therapeutic use.
- I am a co-inventor on Siglec-8-related patents owned by the Johns Hopkins University, and am
entitled to a share of future royalties received by the University on eventual sales of products
protected by those patents.
- The terms of these arrangements are being managed by the Johns Hopkins University and
Northwestern University in accordance with their conflict of interest policies.
ICD-10-CM: Request for 8 New Eosinophil-Associated
Diseases (EADs) Codes and 4 Amended Codes
APFED requested and the CDC approved in 2007 four ICD-9 codes for eosinophil
gastrointestinal diseases (EGIDs). These were converted to three ICD-10-CM
codes.
Other EADs generally use two generic “catch-all” codes, J82 (pulmonary
eosinophilia, not elsewhere classified ) and D72.1 (eosinophilia), either in isolation
or in combination with other non-specific codes.
Four “amendments” to existing codes, including a name change [Churg Strauss
syndrome to EPGA], a separation of two codes that were approved as unique
codes in ICD-9 [EG/EGE], and add exclusions to an existing code [EC].
Eight new EAD codes requested.
Without ICD-10-CM Codes for EADs…?
- Extended time to diagnosis
- Unmet patient needs in management and treatment options in these EADs because each is a different disorder with unique pathophysiology
- Healthcare resources misallocated given current prevalence and inability to collect patient care data and estimate “real” cost of care
- Unable to develop treatments or provide access to currently available approved treatments
- Missed opportunities to identify potential clinical study recruits
Acute versus Chronic Eosinophilic Pneumonia
- Acute Eosinophilic Pneumonia (AEP) was
first described as a distinct entity in medical
literature in 1989.
- AEP is characterized by rapidly progressive
respiratory failure with high levels of lung
eosinophils (>25%).
- Following diagnosis and corticosteroid
treatment, prognosis is excellent.
- Cause is unknown but smoking and
environment may be triggers (e.g., 9/
rescue workers with dust exposure).
- Currently Using Code J18. (for various
pneumonias) and/or J82 (pulmonary
eosinophilia, not elsewhere classified)
- Chronic Eosinophilic Pneumonia (CEP) was first
described in 1969 and is a distinct entity.
- CEP is characterized by progressive shortness of breath
and increase in eosinophils in the lungs and
bloodstream; abnormalities on chest imaging in the
periphery of the lungs, but unlike AEP does not progress
to acute respiratory failure.
- Relapse over many years is common even with
treatment. Can progress to severe asthma or EGPA.
- Cause is unknown; more common in women and adults.
- Currently Using Code J18. (for various pneumonias)
and/or J82 (pulmonary eosinophilia, not elsewhere
classified)
Eosinophilic Asthma (currently coded as J45.* with J82 rarely added)
Cited in research since 1889. Subset of asthma that is characterized by the presence of eosinophils
in the circulation and in the airways.
Is considered a leading cause of severe asthma, affecting 50 to 60 percent (approx 2 million)
of those with severe asthma.
Often associated with chronic sinusitis and nasal polyposis.
Is more prominent in adults and equally affects men and women (different from other
forms of adult asthma).
Frequent exacerbations and detrimental effect on QOL. Does not respond well to inhaled
corticosteroid treatments, even at high doses.
Three new FDA approved biologic therapies that specifically target eosinophils (by blocking IL-5 or
its receptor) reduce asthma exacerbations and are oral steroid sparing.
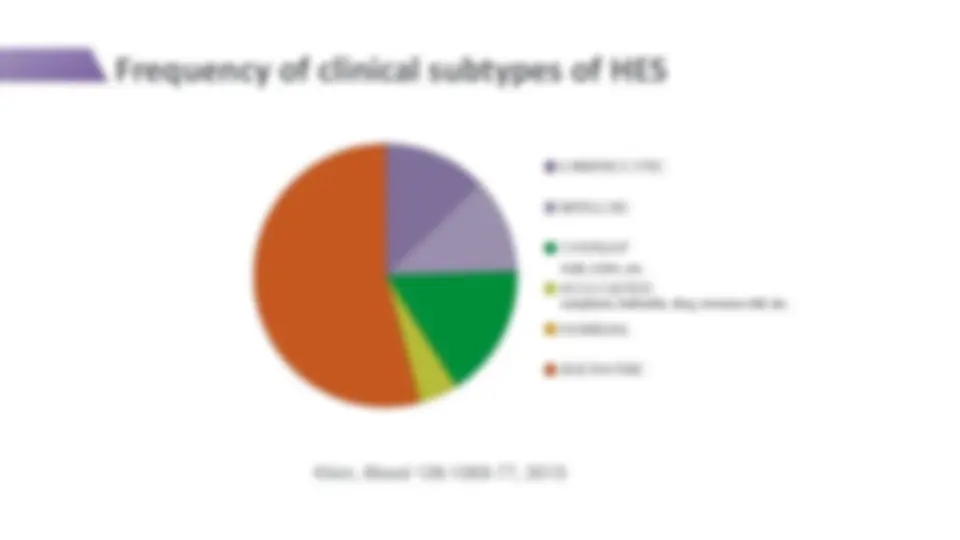
Frequency of clinical subtypes of HES
LYMPHOCYTIC
MYELOID
OVERLAP
ASSOCIATED
FAMILIAL
IDIOPATHIC
neoplasm, helminth, drug, immune def, etc. EGID, EGPA, etc. Klion, Blood 126:1069-77, 2015
Treatments for Hypereosinophilic Syndromes
Khoury and Bochner, J Allergy Clin Immunol Pract 6:1446-53, 2018
Idiopathic
Hypereosinophilic
Syndrome (IHES)
Currently Using Code D72.1 (“eosinophilia”) but this may also sometimes be eosinophilic leukemia IHES accounts for approximately 70 % of HES. Cause of IHES is unknown, and may affect any organ including the heart. Corticosteroids are the first line treatment. Currently no approved drugs indicated for treatment.
Episodic
Angioedema with
Eosinophilia (EAE),
Gleich’s Syndrome
Currently Using Code D72.1 (“eosinophilia”) First described in 1984 as a cyclic disorder characterized by recurrent episodes of fever, swelling, weight gain and eosinophilia recurring every 4 -6 weeks. EAE makes up < 1 % of patients with HES. EAE has traditionally been considered a variant of HES, and more recently LHES. Disease onset may occur at any age but is more common in adulthood.
Hypereosinophilic Syndromes (HES)
Drug Reaction with
Eosinophilia and Systemic
Symptoms (DRESS)
Currently Using Code: D72.1 (“eosinophilia”) + T88.7 (“unspecified
adverse effect of a drug or medicament”)
ICD-11 Code EH
Eosinophilic
Granulomatosis with
Polyangiitis (EGPA)
previously known as
Polyarteritis with Lung
Involvement [Churg-
Strauss Syndrome]
Name Change Only
Currently Using Code: M30.
ICD-11 Code 4A44.A
Other Eosinophil-Associated Diseases
Eosinophilic Granulomatosis with Polyangiitis (EGPA) Previously Known as Churg-Strauss Syndrome (Polyarteritis with lung involvement)
Requesting name change only- Eosinophilic
Granulomatosis with Polyangiitis (EGPA) as the
official name of what had previously referred to as
Churg-Strauss Syndrome.
Is a rare autoimmune disorder that may affect
multiple organ systems, especially the lungs in the
form of asthma, causing damage.
Characterized by abnormal presence of high blood
and tissue eosinophils, inflammation of blood vessels
(vasculitis), and development of inflammatory
nodular lesions called granulomas (granulomatosis).
Without treatment, serious organ damage can occur
and the disease may be fatal.
The cause of EGPA is unknown.
Requesting ICD-10-CM Codes for these EADs
Myeloid Hypereosinophilic Syndrome (MHES) Lymphocytic Variant Hypereosinophilic Syndrome (LHES) Idiopathic Hypereosinophilic Syndrome (IHES) Episodic Angioedema with Eosinophilia (EAE), also called Gleich’s Syndrome
Eosinophilic
Gastritis (EG)*
Eosinophilic
Gastroenteritis
(EGE)*
Eosinophilic
Colitis (EC)*
Acute Eosinophilic Pneumonia Chronic Eosinophilic Pneumonia Eosinophilic Asthma Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Eosinophilic Granulomatosis with Polyangiitis (EGPA), formerly called Churg-Strauss Syndrome *** REQUESTING A MENDMENTS OR N AME CHANGE ONLY*
Pulmonary
Eosinophil Diseases
Hypereosinophilic
Syndromes
Other EGIDs
Existing Code: K52.
Request to delete inclusions for food protein induced enterocolitis syndrome
(FPIES), allergic proctocolitis and milk-protein colitis.
In 2016, FPIES was approved for new ICD-10 CM code K52.21, so we are
requesting an exclusion for FPIES be added to K52..
Eosinophilic colitis diagnoses requires colonoscopy showing elevated
eosinophils. Allergic proctocolitis and milk-protein colitis are not diagnosed
with colonoscopy, occur in newborns, and are usually self-resolving diseases.
Eosinophilic Colitis
Eosinophil Gastrointestinal Diseases (EGIDs)
Code Amendments requested
Summary: Request for ICD-10-CM Codes for
Eosinophil-Associated Diseases
APFED requested and the CDC approved in 2007 four ICD-9 codes for eosinophil
gastrointestinal diseases (EGIDs). These were converted to three ICD-10-CM
codes.
Other EADs generally use two generic “catch-all” codes, J82 (pulmonary
eosinophilia, not elsewhere classified ) and D72.1 (eosinophilia), either in isolation
or in combination with other non-specific codes.
Four “amendments” to existing codes, including a name change [Churg Strauss
syndrome to EPGA], a separation of two codes that were approved as unique
codes in ICD-9 [EG/EGE], and add exclusions to an existing code [EC].
Eight new EAD codes requested.