Download infective endocarditis echocardiography and more Slides Biology in PDF only on Docsity!
ECHOCARDIOGRAPHIC
EVALUATION OF ENDOCARDIAL
DISEASES
PRESENTERS:CHARITY.M COLLINS.N CHAIRPERSON;STEPHEN.O-CLINICAL CARDIOLOGY
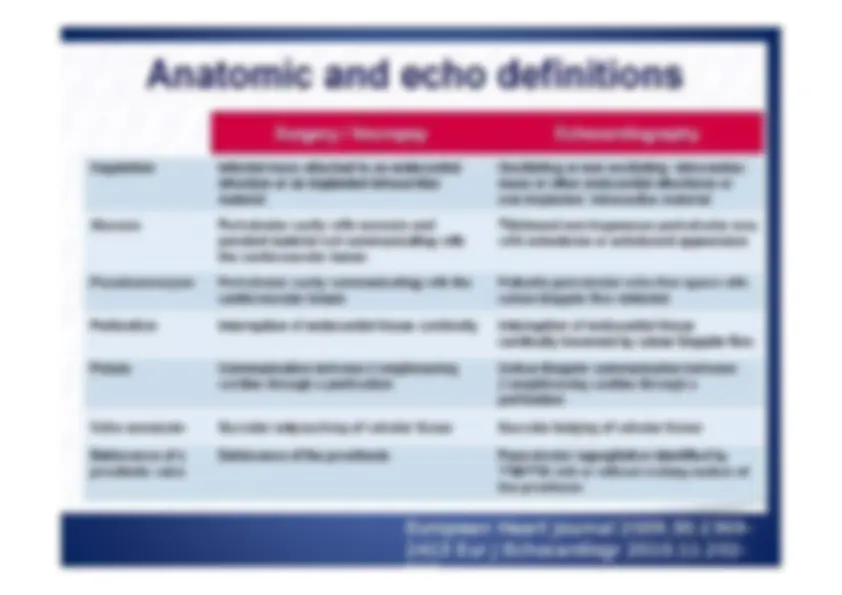
European Journal of Echocardiography 2010; 11: 202- 219
European Heart Journal 2009;30:2369- 2413 Eur J Echocardiogr 2010;11:202- 219
Echocardiographic criteria
for IE
- (^) Vegetations
- (^) Hallmark lesion of IE
- (^) Abscess and perivalvular involvement - (^) Aortic valve and prosthetic valve: more frequent - (^) Perivalvular complications: pseudoaneurysm and fistulization
- (^) New dehiscence of a prosthetic valve Eur J Echocardiogr 2010;11:202- 219
Limitations and Pitfalls of Echo
for Diagnosis of IE
- Both the sensitivity and specificity of TTE and TEE are not 100%.
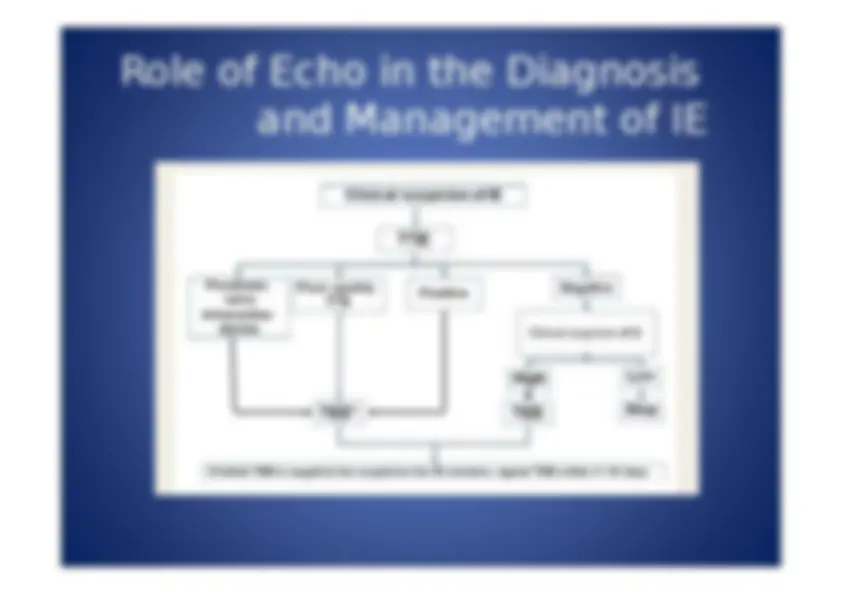
- A negative echo exam does not rule out IE.
- Repeat TTE/TEE maybe necessary in some situations.
- Results of the echo study must interpreted with caution,taking into account the clinical presentation and the likelihood of IE.
Echocardiography is not 100% sensitive for the diagnosis of infective endocarditis
- (^) A negative echocardiogram may be observed in about 15% of infective endocarditis.
- (^) The most frequent explanations :
- (^) Very small vegetations
- (^) Difficulties in identifying vegetations in the presence of pre- existing severe lesions.( mitral valve prolapse, degeneration lesions, and prosthetic valves)
- (^) When vegetations are non-oscillating and/or atypically located.
- (^) At the very early stage of the disease
- (^) When vegetations are not yet present or too small to be identified.
- (^) A repeat examination has to be performed 7- 10 days after the 1 st examination in case of high level of clinical suspicion or even earlier when justified by clinical presentation. Eur J Echocardiogr 2010;11:202- 219
Eur J Echocardiogr 2010;11:202- 219
Indications and timing of
surgery in IE
- (^) Heart failure
- (^) The most frequent indication: 40-60% of IE
- (^) Acute regurgitation
- (^) Uncontrolled infection
- (^) Abscess, pseudoaneurysm and fistula
- (^) Preventive of embolism
- (^) Vegetations > 10mm : high risk of embolism (^) Eur J Echocardiogr 2010;11:202- 219
Echo findings suggestive of
early surgery for IE with
heart failure
- (^) Extensive obstructive valve lesions
- (^) Massive regurgitation
- (^) Associated abscess and pseudoaneurysm
Vegetation and pseudoaneurysm fistul a absces s
Evolution of anterior aortic
bioprosthetic abscess
Echo vs Anatomy
Eur J Echocardiogr 2010;11:202- 219
Prognosis Assessment at
Admission
- (^) Perivalvular complications
- (^) Severe native or prosthetic regurgitation or obstruction
- (^) Low LVEF
- (^) Pulmonary hypertension
- (^) Large vegetations
- (^) Premature mitral valve closure or other signs of elevated diastolic pressures The above echo findings have been associated with a worse prognosis of IE.
Echo follow up under
therapy
- (^) Echo must be used to follow up of patients with IE under antibiotic therapy
- (^) The number, type and timing of repeated exams depend on - (^) The clinical presentation - (^) The type of organisms - (^) The initial echographic findings
- (^) Weekly TTE for non-complicated streptococcal native IE
- (^) More frequent TTE and TEE for post-op staphylococcal early PVE