Download Intestinal obstruction and more Study notes Pathophysiology in PDF only on Docsity!
Intestinal obstruction
Prof. Marek Jackowski
Definition
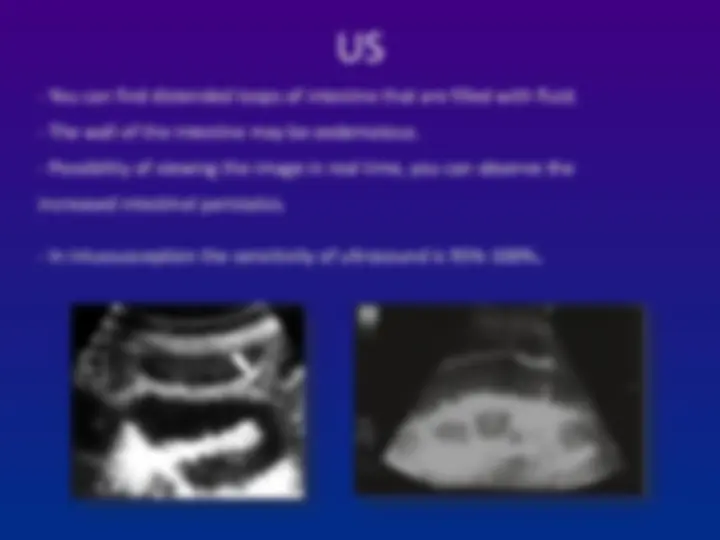
- Any condition interferes with normal
propulsion and passage of intestinal contents.
- Can involve the small bowel, colon or both
small and colon as in generalized ileus.
Epidemiology 1 % of all hospitalization 3 - 5 % of emergency surgical admissions More frequent in female patients - gynecological and pelvic surgical operations are important etiologies for postop. adhesions Adhesion is the most common cause of intestinal obstruction 80 % of bowel obstruction due to small bowel obstruction - the most common causes are:
- Adhesion
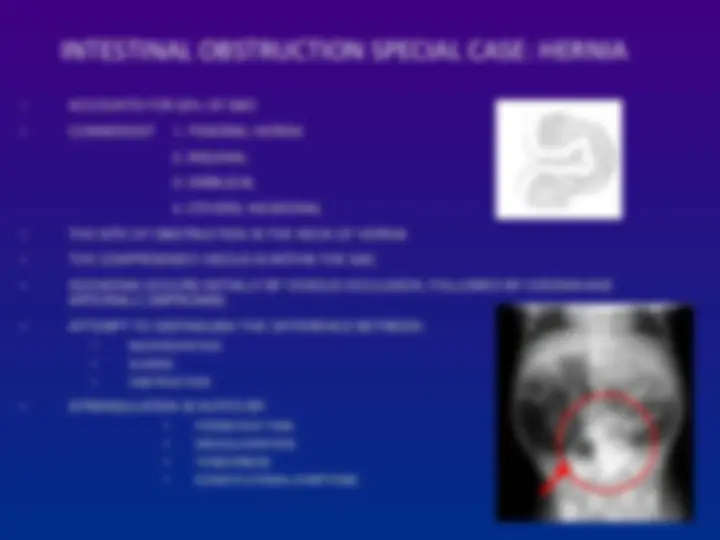
- Hernia
- Neoplasm 20 % due to colon obstruction - the most common cause:
- CR-cancer 60 - 70 %,
- diverticular disease and volvulus - 30 % Mortality rate range between 3 % for simple bowel obstruction to 30 % when there is strangulation or perforation Recurrent rate vary according to method of treatment ;
- conservative 12 %
- surgical treatment 8 - 32 %
Classification
- Cause of obstruction: mechanical or
functional.
- Duration of obstruction: acute or chronic.
- Extent of obstruction: partial or complete
- Type of obstruction: simple or complex
(closed loop and strangulation).
Etiology
Mechanical bowel obstruction:
A. Small bowel obstruction:
- Adhesion 60 %
- Hernia 20 %
- Neoplasm 5 %
- Volvulus 5 %
- Others: IBD-GALL STONE-FOREIGN BODY-INTUSSUSCEPTION B. Large bowel obstruction:
- Cancer 60 %
- Diverticular disease 15 %
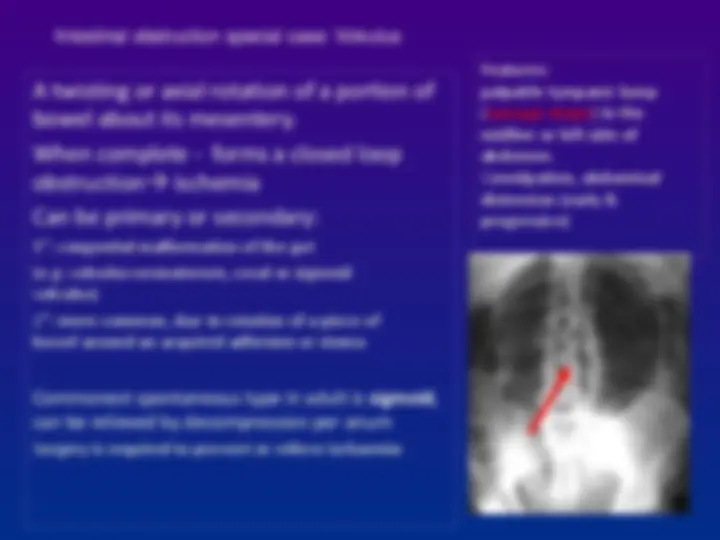
- Volvulus 15 %
- Others: hernia – fecal impaction-inflammatory
Etiology
Functional bowel obstruction: 3 types
A. Vascular occlusion ileus.
B. Spastic ileus. (intestine remain contracted and no
propulsive) causes are:
- Uremia.
- Porphyria.
- Heavy metal poison.
C. Adynamic or inhibition ileus:
- Post operation mostly after abdominal surgery
- Metabolic causes: hyponateremia-hypokalemia – hypomagnesaemia.
- Drugs: morphine - antacid-anticonvulsant.
- Intra-abdominal inflammation – sepsis – occult wound infection.
- Pneumonia – renal stone – retroperitoneal hematoma – fracture spine and ribs
CAUSES OF I.O (DYNAMIC)
Intraluminal
- Impaction
- Foreign bodies
- Bezoars
- Gallstone Intramural
- Congenital atresia
- Stricture
- Malignancy ( 15 %) Extramural
- Bands/ adhesion ( 40 %)
- Hernia ( 12 %)
- Volvulus
- Intussusception
- Tumor- benign/malignant
Pathophysiology: Proximal bowel dilated & develops altered motility dilate reduce peristaltic strength flaccidity & paralysis (prev. vascular damage due to inc. intraluminal pressure) Distal to obs. Bowel exhibits normal peristalsis & absorbtion become empty contract & become immobile Distention is by gas & fluid
- Gas: aerobic & anaerobic growth
- Fluid: Digestive juices & retarded absorption Dehydration & electrolytes loss: Reduced oral intake, defective intestinal absorption, loses from vomiting & sequestration in bowel of lumen.
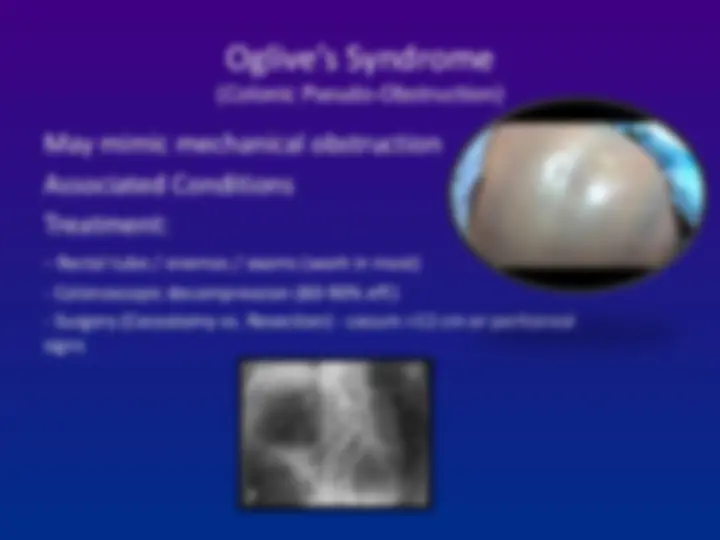
Functional obstruction
secondary to factors that cause either paralysis or dysmotility of intestinal peristalsis. Postoperative ileus is the most common form Postoperative ileus - after intra-abdominal operation Postoperative ileus correlates with degree of surgical trauma and type of surgery Different anatomic segments of GIT recover at different rates after manipulation and trauma:
- Small bowel - hours after operation.
- Stomach - 24 - 48 hrs.
- Colon - 3 - 5 days post op.
should be differentiated from early postoperative mechanical
bowel obstruction:
Occurs within the first 6 weeks post operation
Acute adhesions > 90 %
other causes:
Internal herniation intra-abdominal abscess intramural hematoma anastomatic edema and leak Difficult to differentiate by clinical presentation and X-ray so contrast study and CT scan - helpful
Postoperative ileus
Small Bowel Obstruction
Etiology
- Adhesions
- Malignancy
- External or Internal Hernia
- Volvulus
- Crohn’s Disease
- Intra-abdominal Abscess
Large Bowel Obstruction
Etiology
- Colon Cancer
- Diverticulitis
- Extrinsic Cancer
- Fecal Impaction
- Intussusception
- Volvulus
- Incarcerated Hernias