


By: Leslie, Joie, & Ali
Feb 09, 2026




Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
medication administrations different routes
Typology: Summaries
1 / 15

This page cannot be seen from the preview
Don't miss anything!
Addison’s Diseases
Risk factors
Type 1 Diabetes
Thyroid Disorders
History of adrenal infection
Long-term steroid withdrawal
Family history of autoimmune disease
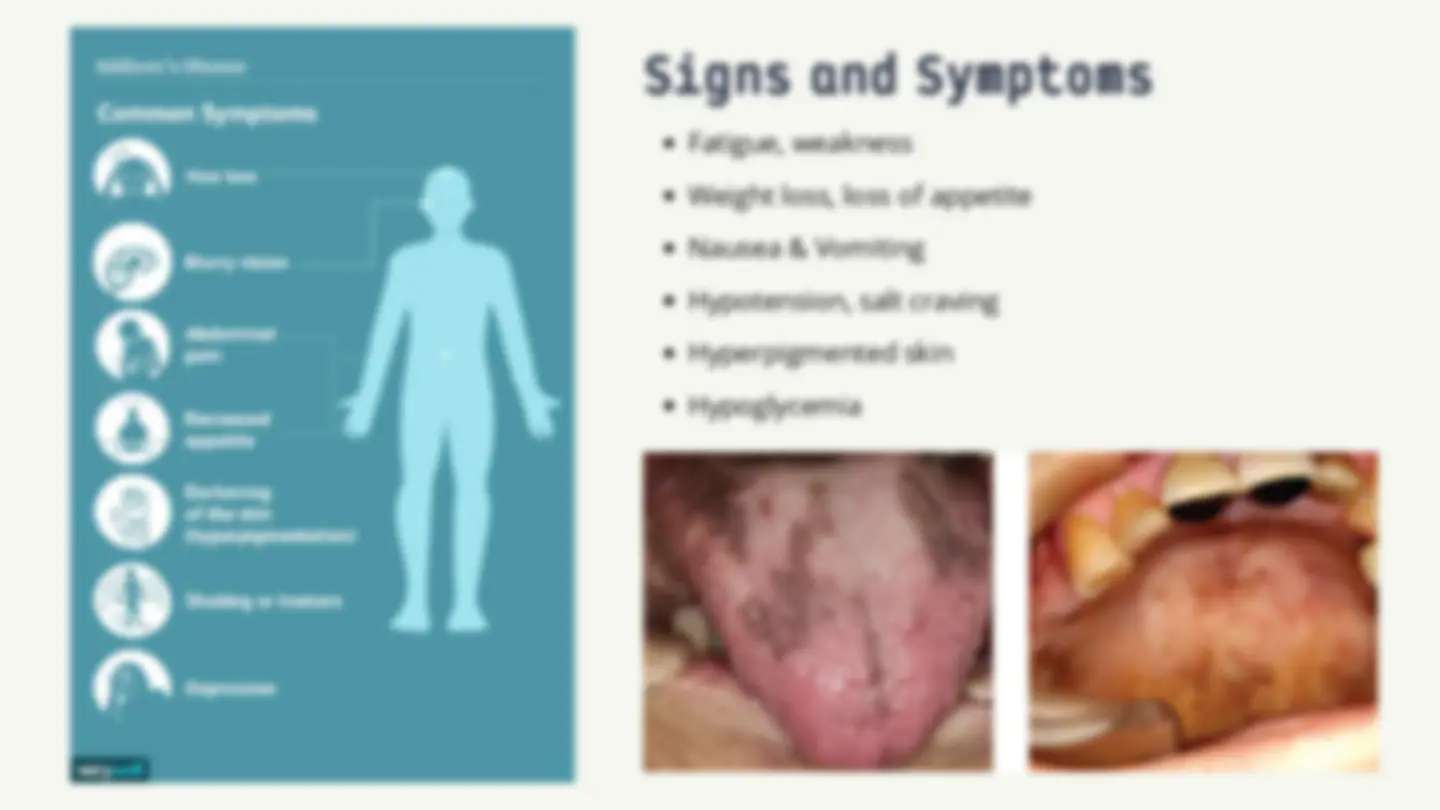
Signs and Symptoms
Fatigue, weakness
Weight loss, loss of appetite
Nausea & Vomiting
Hypotension, salt craving
Hyperpigmented skin
Hypoglycemia
Balanced diet
Adequte salt intake
Medical alert bracelet
Regular follow-up
Stress management
Non-Pharmacologic
NURSING INTERVENTION:
Pharmacologic
PATIENT TEACHING
Glucocorticoids: Hydrocortison, Prednisone
Mineralcorticoids: Fludrocortisone
hydrocortisone & fluid in crisis
Monitor BP, electrolytes, glucose Assess for signs of crisis Administer steroids as prescribed Maintain fluid balance
Never stop steroids abruptly Increase dose during stress/illness Carry emergency steroid kit Recognize crisis symptoms
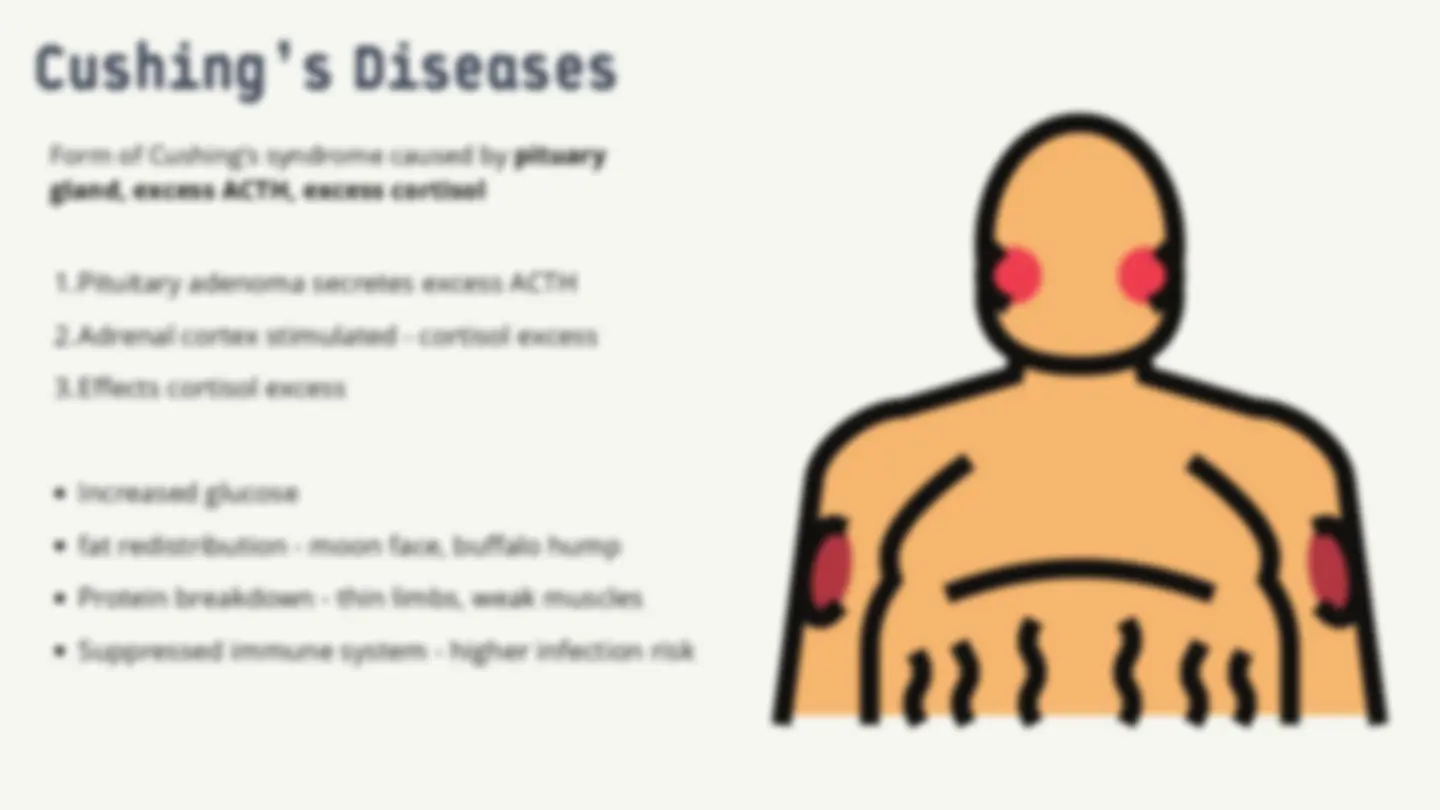
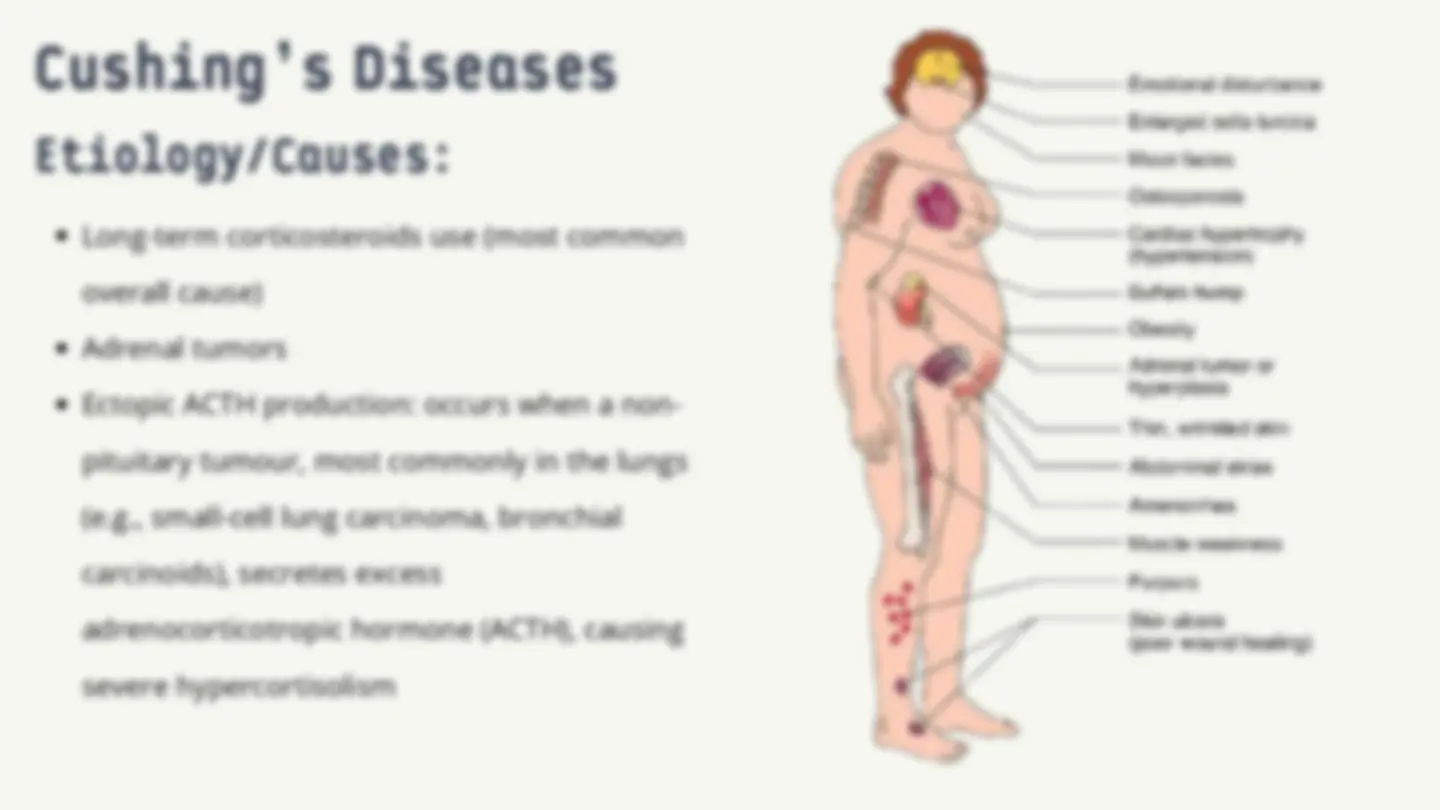
Cushing’s Diseases
1.Pituitary adenoma secretes excess ACTH
2.Adrenal cortex stimulated - cortisol excess
3.Effects cortisol excess
Increased glucose
fat redistribution - moon face, buffalo hump
Protein breakdown - thin limbs, weak muscles
Suppressed immune system - higher infection risk
Risk factors
Long-term steroids theraphy
Pituary/adrenal tumors
Obesity
Type 2 diabetes
Hypertension
Signs and Symptoms
Moon face, buffalo hump, central obesity
Thin arms & legs
Purple striae on abdomen
Apperance:
Hypertension
Hyperglycemia
Muscle weakness
Weight management
Low- sodium
Infection prevention
Stress reduction
Non-Pharmacologic
Pharmacologic
PATIENT TEACHING:
Cortisol- lowering drugs
Surgery for tumor removal
Radiation theraphy
Monitor BP, electrolytes, glucose Assess for infection Skin care (fragile skin) Promote mobility & safety
Take medications as prescribed Monitor blood sugar Follow dietary recommendations Report infection signs Maintain follow-up appointments
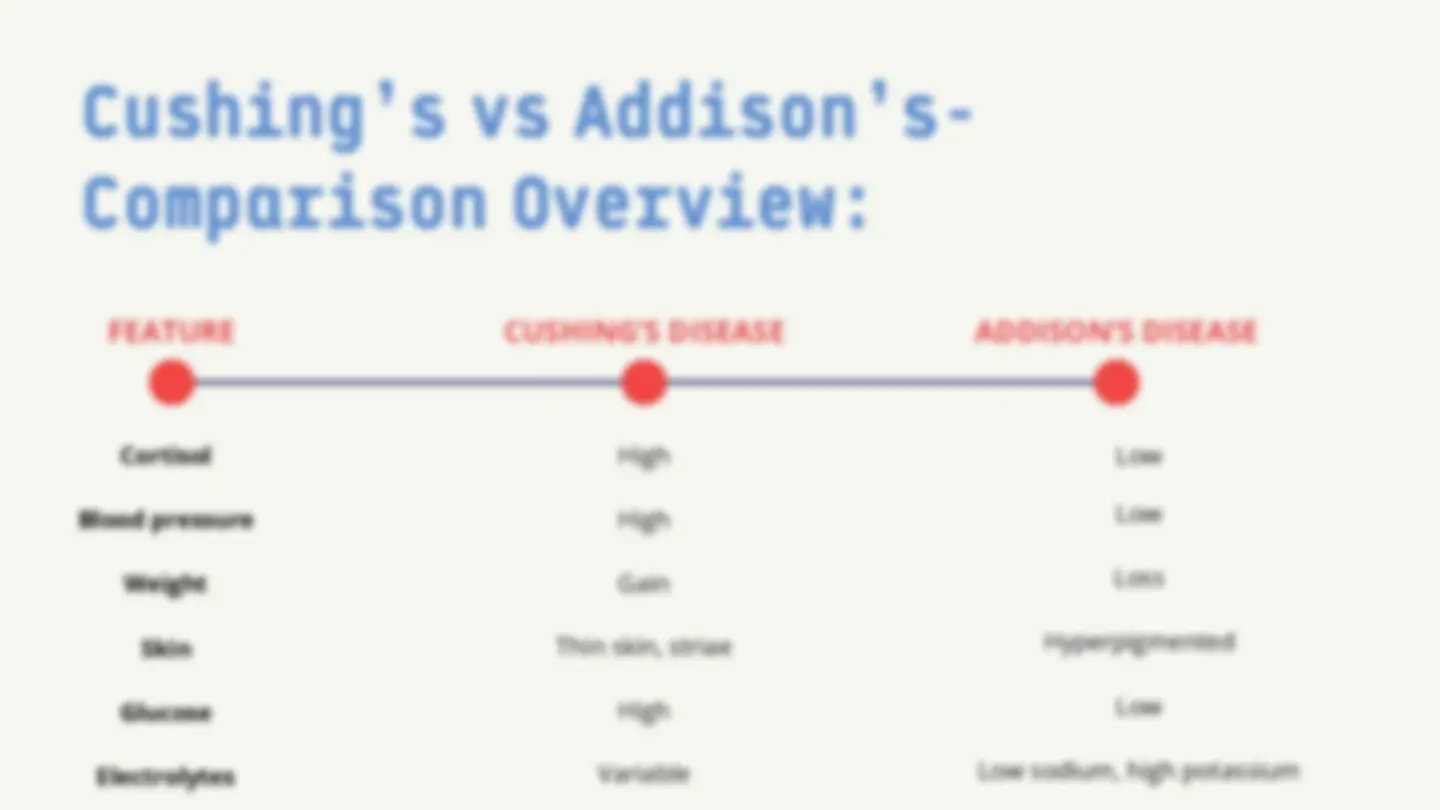
Cushing’s vs Addison’s-
Comparison Overview:
Cortisol
Blood pressure
Weight
Skin
Glucose
High
High
Gain
Thin skin, striae
High
Low
Low
Loss
Hyperpigmented
Low
Electrolytes Variable^ Low sodium, high potassium