Download Understanding Normal Laboratory Values for Blood Components and Tests and more Lecture notes Nursing in PDF only on Docsity!
Laboratory Values
PYRAMID TERMS
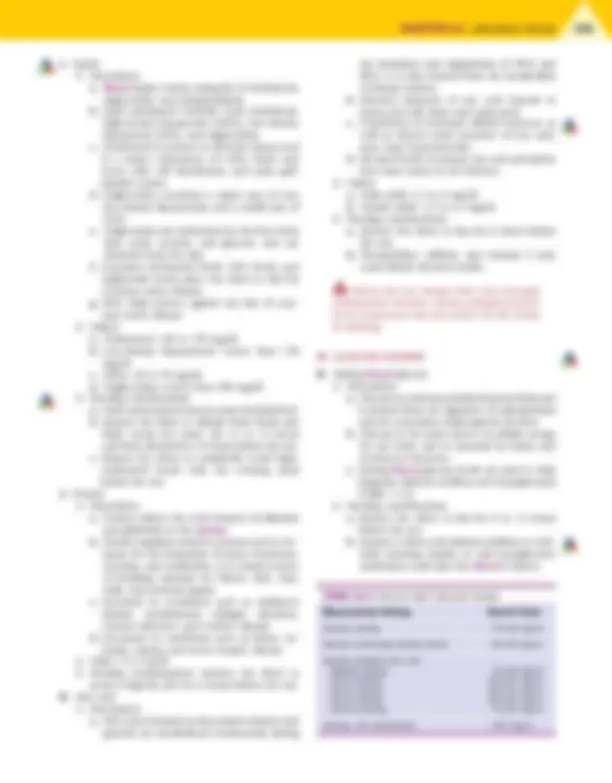
blood The liquid pumped by the heart through the arteries, veins, and capillaries. Blood is composed of a clear yellow fluid (plasma), formed elements, and cell types with different functions (Fig. 11-1). blood cell Any of the formed elements of the blood, including red cells (erythrocytes), white cells (leukocytes), and plate- lets (thrombocytes). plasma The watery, straw-colored, fluid part of lymph and the blood in which the formed elements (blood cells) are sus- pended. Plasma is made up of water, electrolytes, protein, glucose, fats, bilirubin, and gases and is essential for carry- ing the cellular elements of the blood through the circulation. serum The clear and thin fluid part of blood that remains after coagulation. Serum contains no blood cells, platelets, or fibrinogen. venipuncture Puncture into a vein to obtain a blood speci- men for testing; the antecubital veins are the veins of choice because of ease of access.
THE PYRAMID TO SUCCESS
This chapter identifies the normal adult values for the most common laboratory tests. It is important to remember that normal laboratory values may vary slightly, depending on the laboratory setting and equip- ment used in testing. If you are familiar with the normal values, you will be able to determine whether an abnor- mality exists when a laboratory value is presented in a question. The questions on the NCLEX-RN examination related to laboratory values will require you to identify whether the laboratory value is normal or abnormal, and then you are required to think critically about the effects of the laboratory value in terms of the client. Pyramid Points focus on knowledge of the normal values for the most common laboratory tests, therapeutic serum medication levels of commonly prescribed medi- cations, and determination of the need to implement specific actions based on the findings. When a question is presented on the NCLEX-RN examination regarding a specific laboratory value, note the disorder presented in the question and the associated body organ affected as
a result of the disorder. This process will assist you in determining the correct answer. For example, if the ques- tion asks about the immune status of a client receiving chemotherapy, assessment of laboratory values will focus on the white blood cell (WBC) count and the neu- trophils. You will need to analyze these results as possi- bly being low and determine the specific client need, which in this case would be the risk for infection. In the client receiving chemotherapy who has a low WBC count, your plan centers on the immune system and protecting the client from infection. Implementa- tion focuses on preventive interventions related to infec- tion, perhaps protective isolation measures. Evaluation may focus on maintenance of a normal temperature in the client. Box 11-1 lists some of the common abbrevia- tions found in laboratory values. The Priority Nursing Actions box lists the steps needed for obtaining a blood sample.
CLIENT NEEDS
Safe and Effective Care Environment
Applying principles of infection control Ensuring surgical asepsis when obtaining a specimen Implementing procedures for handling hazardous and infectious materials Maintaining standard, transmission-based, and surgical asepsis Obtaining informed consent for specific procedures Verifying the identity of the client
Health Promotion and Maintenance
Preparing the client for the laboratory test Discussing the importance of follow-up laboratory studies Identifying community resources available for the follow-up Implementing posttest procedures Describing specific interventions or home care mea-
114 sures required based on the results
Monitoring for signs and symptoms that indicate the need to notify the health care provider
Psychosocial Integrity
Communicating the purpose of the laboratory test to the client
Communicating with the client regarding the labora- tory results Providing emotional support during testing
Physiological Integrity
Identifying normal values for the most common labo- ratory tests Identifying therapeutic serum medication levels of commonly prescribed medications Monitoring for clinical manifestations associated with an abnormal laboratory value Providing comfort measures Reporting significant laboratory values Determining the significance of an abnormal laboratory value and the need to implement specific actions based on the laboratory results Monitoring for potential complications related to a test
Drawing blood specimens from an extremity in which an intravenous solution is infusing can pro- duce an inaccurate result. Prolonged use of a tourni- quet and clenching and unclenching the hand before venous sampling can increase the blood level of potassium, producing an inaccurate result.
TOTAL BODY WEIGHT
WHOLE BLOOD (percentage by volume)
FORMED ELEMENTS (number per cubic mm)
PLASMA (percentage by weight)
Blood 8%
Other fluids and tissues 92%
Centrifuged sample of blood
Buffy coat
PLASMA 55%
Platelets 150,000-400,
Proteins 7%
Water 91%
Other solutes 2%
Leukocytes 4,500-11,000 Neutrophils^ 60-70%
Lymphocytes 20-25%
Monocytes 3-8%
Eosinophils 2-4%
Basophils 0.5-1%
Albumins 54% Globulins 38% Fibrinogen 4% Prothrombin 1%
Ions Nutrients Waste products Gases Regulatory substances
LEUKOCYTES
PROTEINS
Erythrocytes 4-6.2 million
OTHER SOLUTES
FORMED ELEMENTS 45%
s FIGURE 11-1 Approximate values for the components of blood in a normal adult. (Modified from Thibodeau, G.A., & Patton, K.T. [2010]. The human body in health and disease [5th ed.]. St. Louis: Mosby.)
tBox 11-1 Pyramid Abbreviations
Abbreviation Definition g/dL grams per deciliter IU/L International units per liter mcg/dL micrograms per deciliter mcg/mL micrograms per milliliter mEq/L milliequivalents per liter mg/dL milligrams per deciliter microunits/mL microunits per milliliter mL/kg milliliters per kilogram mm 3 millimeters cubed mm/hr millimeters per hour ng/mL nanograms per milliliter pg/mL picogram per milliliter units/L units per liter mL microliters
s
CHAPTER 11 Laboratory Values 115
- Value: 20 to 36 seconds, depending on the type of activator used
- Nursing considerations a. If the client is receiving intermittent heparin therapy, draw the blood sample 1 hour before the next scheduled dose. b. Do not draw samples from an arm into which heparin is infusing. c. Transport specimen to the laboratory immediately. d. Provide direct pressure to the venipuncture site for 3 to 5 minutes. e. The aPTT should be between 1.5 and 2.5 times normal when the client is receiving heparin therapy; if the value is prolonged (longer than 90 seconds), the client is at risk for bleeding.
If the aPTT value is prolonged (longer than 90 seconds) in a client receiving IV heparin therapy, initiate bleeding precautions.
B. Prothrombin time (PT) and international normal- ized ratio (INR)
- Description a. Prothrombin is a vitamin K–dependent gly- coprotein produced by the liver that is neces- sary for fibrin clot formation. b. Each laboratory establishes a normal or con- trol value based on the method used to per- form the PT test. c. The PT measures the amount of time it takes in seconds for clot formation and is used to mon- itor response to warfarin sodium (Coumadin) therapy or to screen for dysfunction of the extrinsic clotting system resulting from liver disease, vitamin K deficiency, or disseminated intravascular coagulation. d. A PT value within 2 seconds (plus or minus) of the control is considered normal. e. The INR is a frequently used test to measure the effects of oral anticoagulants. f. The INR standardized the PT ratio and is cal- culated in the laboratory setting by raising the observed PT ratio to the power of the international sensitivity index specific to the thromboplastin reagent used.
- Values a. PT: 9.6 to 11.8 seconds (male adult); 9.5 to 11.3 seconds (female adult) b. INR: 2 to 3 for standard warfarin therapy c. INR: 3 to 4.5 for high-dose warfarin therapy
- Nursing considerations a. A baseline PT should be drawn before anti- coagulation therapy is started; note the time of collection on the laboratory form. b. Provide direct pressure to the venipuncture site for 3 to 5 minutes.
c. Concurrent warfarin therapy with heparin therapy can lengthen the PT for up to 5 hours after dosing. d. Diets high in green leafy vegetables can increase the absorption of vitamin K, which shortens the PT. e. Orally administered anticoagulation therapy usually maintains the PT at 1.5 to 2 times the laboratory control value. f. A PT longer than 30 seconds places the client at risk for bleeding.
If the PT value is longer than 30 seconds in a client receiving warfarin therapy, initiate bleeding precautions.
C. Clotting time
- Description: The time required for the interac- tion of all factors involved in the clotting process
- Value: 8 to 15 minutes
- Nursing considerations a. The client should not receive heparin therapy for 3 hours before specimen collection because the heparin therapy will affect the results. b. The test result is falsely prolonged by anti- coagulant therapy, test tube agitation, or expo- sure of the specimen to high temperatures. D. Platelet count
- Description a. Platelets function in hemostatic plug forma- tion, clot retraction, and coagulation factor activation. b. Platelets are produced by the bone marrow to function in hemostasis.
- Value: 150,000 to 400,000 cells/mm 3
- Nursing considerations a. Monitor the venipuncture site for bleeding in clients with known thrombocytopenia. b. High altitudes, chronic cold weather, and exercise increase platelet counts. c. Bleeding precautions should be instituted in clients with a low platelet count.
Monitor the platelet count closely in clients receiving chemotherapy because of the risk for thrombocytopenia.
III. ERYTHROCYTE STUDIES
A. Erythrocyte sedimentation rate
- Description a. Rate at which erythrocytes settle out of anti- coagulated blood in 1 hour b. A nonspecific test used to detect illnesses associated with acute and chronic infection, inflammation, advanced neoplasm, and tis- sue necrosis or infarction
s
CHAPTER 11 Laboratory Values 117
- Value: 0 to 30 mm/hr, depending on age of client
- Nursing consideration: Fasting is not necessary, but a fatty meal may cause plasma alterations. B. Hemoglobin and hematocrit
- Description a. Hemoglobin is the main component of ery- throcytes and serves as the vehicle for trans- porting oxygen and carbon dioxide. b. Hemoglobin determinations are important in identifying anemia. c. Hematocrit represents RBC mass and is an important measurement in the identification of anemia or polycythemia (Table 11-2).
- Nursing consideration: Fasting is not required. C. Serum iron
- Description a. Iron is found predominantly in hemoglobin. b. Iron acts as a carrier of oxygen from the lungs to the tissues and indirectly aids in the return of carbon dioxide to the lungs. c. Iron aids in diagnosing anemias and hemo- lytic disorders.
- Normal values a. Male adult: 65 to 175 mcg/dL b. Female adult: 50 to 170 mcg/dL
- Nursing consideration: Level of iron will be in- creased if the client has ingested iron before the test. D. RBC count (erythrocytes)
- Description a. RBCs function in hemoglobin transport, which results in delivery of oxygen to the body tissues. b. RBCs are formed by red bone marrow, have a life span of 120 days, and are removed from the blood via the liver, spleen, and bone marrow. c. The RBC count aids in diagnosing anemias and blood dyscrasias. d. The RBC count evaluates the ability of the body to produce RBCs in sufficient numbers.
- Values a. Female adult: 4 to 5.5 million cells/mL b. Male adult: 4.5 to 6.2 million cells/mL
- Nursing consideration: Fasting is not required.
IV. SERUM ENZYMES AND CARDIAC MARKERS
(Table 11-3) A. Creatine kinase (CK)
- Description a. Creatine kinase is an enzyme found in muscle and brain tissue that reflects tissue catabolism resulting from cell trauma. b. The CK level begins to rise within 6 hours of muscle damage, peaks at 18 hours, and returns to normal in 2 to 3 days. c. The test for CK is performed to detect myo- cardial or skeletal muscle damage or central nervous system damage; a normal CK value is 26 to 174 units/L. d. Isoenzymes include CK-MB (cardiac), CK-BB (brain), and CK-MM (muscles). e. Isoenzyme CK-MB is found mainly in cardiac muscle, CK-BB is found mainly in brain tis- sue, and CK-MM is found mainly is skeletal muscle.
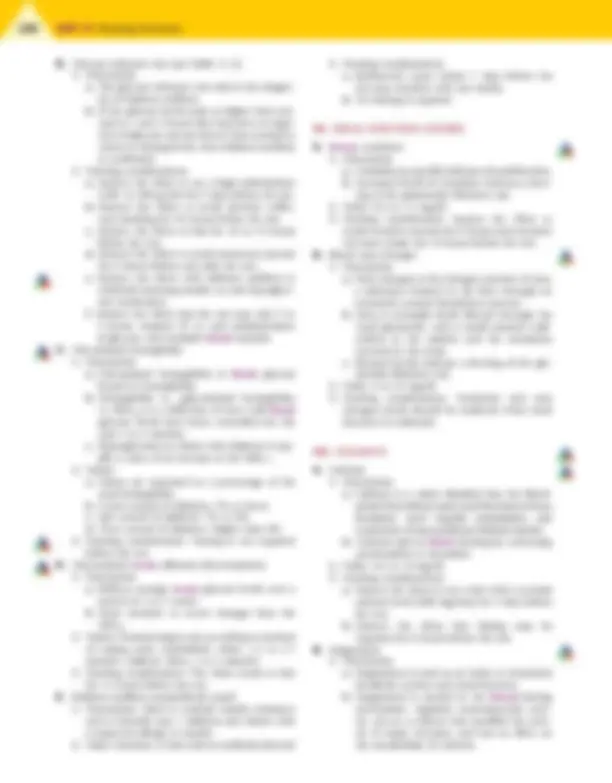
TABLE 11-2 Normal Adult Blood Components Blood Component Normal Value HEMOGLOBIN Male adult 14-16.5 g/dL Female adult 12-15 g/dL HEMATOCRIT Male adult 42%-52% Female adult 35%-47% IRON Male adult 65-175 mcg/dL Female adult 50-170 mcg/dL RED BLOOD CELLS Male adult 4.5-6.2 million/mL Female adult 4-5.5 million/mL
TABLE 11-3 Normal Adult Serum Enzymes/Cardiac Markers Serum Enzyme Normal Value Creatine kinase (CK) 26-174 units/L CK isoenzymes CK-MB 0%-5% of total CK-MM 95%-100% of total CK-BB 0% Lactate dehydrogenase 140-280 units/L Lactate dehydrogenase isoenzymes LDH1 14%-26% LDH2 29%-39% LDH3 20%-26% LDH4 8%-16% LDH5 6%-16% Troponin I <0.6 ng/mL; >1.5 ng/mL indicates myocardial infarction Troponin T >0.1-0.2 ng/mL indicates myocardial infarction Myoglobin <90 mcg/L; elevation could indicate myocardial infarction Atrial natriuretic peptides (ANP)
22 to 27 pg/mL
Brain natriuretic peptides (BNP)
Less than 100 pg/mL
C-type natriuretic peptides (CNP)
Not yet determined; reference range provided with results and should be reviewed
118 UNIT III Nursing Sciences
b. The level rises during periods of bone growth, liver disease, and bile duct obstruction.
- Value: 4.5 to 13 King-Armstrong units/dL
- Nursing considerations a. The client may need to fast 12 hours before the test. b. Hepatotoxic medications administered within 12 hours before specimen collection can cause a falsely elevated value. c. Transport the specimen to the laboratory immediately. C. Ammonia
- Description a. Ammonia is a byproduct of protein catabo- lism; most of it is created by bacteria acting on proteins present in the gut. b. Ammonia is metabolized by the liver and excreted by the kidneys as urea. c. Elevated levels resulting from hepatic dys- function may lead to encephalopathy. d. Venous ammonia levels are not a reliable indicator of hepatic coma.
- Value: 10 to 80 mcg/dL
- Nursing considerations a. Instruct the client to fast, except for water, and to refrain from smoking for 8 to 10 hours before the test; smoking increases ammonia levels. b. Place the specimen on ice and transport to the laboratory immediately. D. Alanine aminotransferase (ALT)
- Description: Used to identify hepatocellular dis- ease of the liver and to monitor improvement or worsening of the disease.
- Value: 4 to 6 international units/L
- Nursing considerations a. Previous intramuscular injections may cause elevated levels. b. No fasting is required. E. Aspartate aminotransferase (AST)
- Description: Used to evaluate a client with sus- pected hepatocellular disease (may also be used along with other cardiac markers to evaluate cor- onary artery occlusive disease)
- Value: 0 to 35 units/L
- Nursing considerations a. Previous intramuscular injections may cause elevated levels b. No fasting is required. F. Amylase
- Description a. This enzyme, produced by the pancreas and salivary glands, aids in the digestion of com- plex carbohydrates and is excreted by the kidneys. b. In acute pancreatitis, the amylase level is greatly increased; the level starts rising 3 to
6 hours after the onset of pain, peaks at about 24 hours, and returns to normal in 2 to 3 days after the onset of pain.
- Value: 25 to 151 units/L
- Nursing considerations a. On the laboratory form, list the medications that the client has taken during the previous 24 hours before the test. b. Note that many medications may cause false- positive or false-negative results. c. Results are invalidated if the specimen was obtained less than 72 hours after cholecys- tography with radiopaque dyes. G. Lipase
- Description a. This pancreatic enzyme converts fats and tri- glycerides into fatty acids and glycerol. b. Elevated lipase levels occur in pancreatic dis- orders; elevations may not occur until 24 to 36 hours after the onset of illness and may remain elevated for up to 14 days.
- Value: 10 to 140 units/L
- Nursing considerations: Endoscopic retrograde cholangiopancreatography (ERCP) may increase lipase activity. H. Bilirubin
- Description a. Bilirubin is produced by the liver, spleen, and bone marrow and is also a byproduct of hemoglobin breakdown. b. Total bilirubin levels can be broken down into direct bilirubin, which is excreted pri- marily via the intestinal tract, and indirect bilirubin, which circulates primarily in the bloodstream. c. Total bilirubin levels increase with any type of jaundice; direct and indirect bilirubin levels help differentiate the cause of the jaundice.
- Values a. Bilirubin, direct (conjugated): 0 to 0.3 mg/dL b. Bilirubin, indirect (unconjugated): 0.1 to 1 mg/dL c. Bilirubin, total: Lower than 1.5 mg/dL
- Nursing considerations a. Instruct the client to eat a diet low in yellow foods, avoiding foods such as carrots, yams, yellow beans, and pumpkins, for 3 to 4 days before the blood is drawn. b. Instruct the client to fast for 4 hours before the blood is drawn. c. Note that results will be elevated with the ingestion of alcohol or the administration of morphine sulfate, theophylline, ascorbic acid (vitamin C), or acetylsalicylic acid (aspirin). d. Note that results are invalidated if the client has received a radioactive scan within 24 hours before the test.
120 UNIT III Nursing Sciences
I. Lipids
- Description a. Blood lipids consist primarily of cholesterol, triglycerides, and phospholipids. b. Lipid assessment includes total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), and triglycerides. c. Cholesterol is present in all body tissues and is a major component of LDLs, brain and nerve cells, cell membranes, and some gall- bladder stones. d. Triglycerides constitute a major part of very low-density lipoproteins and a small part of LDLs. e. Triglycerides are synthesized in the liver from fatty acids, protein, and glucose, and are obtained from the diet. f. Increased cholesterol levels, LDL levels, and triglyceride levels place the client at risk for coronary artery disease. g. HDL helps protect against the risk of coro- nary artery disease
- Values: a. Cholesterol: 140 to 199 mg/dL b. Low-density lipoproteins: Lower than 130 mg/dL c. HDLs: 30 to 70 mg/dL d. Triglycerides: Lower than 200 mg/dL
- Nursing considerations a. Oral contraceptives may increase the lipid level. b. Instruct the client to abstain from foods and fluid, except for water, for 12 to 14 hours and from alcohol for 24 hours before the test. c. Instruct the client to completely avoid high- cholesterol foods with the evening meal before the test. J. Protein
- Description a. Protein reflects the total amount of albumin and globulins in the plasma. b. Protein regulates osmotic pressure and is nec- essary for the formation of many hormones, enzymes, and antibodies; it is a major source of building material for blood, skin, hair, nails, and internal organs. c. Increased in conditions such as Addison’s disease, autoimmune collagen disorders, chronic infection, and Crohn’s disease. d. Decreased in conditions such as burns, cir- rhosis, edema, and severe hepatic disease.
- Value: 6 to 8 g/dL
- Nursing considerations: Instruct the client to avoid a high-fat diet for 8 hours before the test. K. Uric acid
- Description a. Uric acid is formed as the purines adenine and guanine are metabolized continuously during
the formation and degradation of DNA and RNA. It is also formed from the metabolism of dietary purines. b. Elevated amounts of uric acid deposit in joints and soft tissue and cause gout. c. Conditions of increased cellular turnover, as well as slowed renal excretion of uric acid, may cause hyperuricemia. d. Elevated levels of urinary uric acid precipitate into urate stones in the kidneys.
- Values a. Male adult: 4.5 to 8 mg/dL b. Female adult: 2.5 to 6.2 mg/dL
- Nursing considerations a. Instruct the client to fast for 8 hours before the test. b. Theophylline, caffeine, and vitamin C may cause falsely elevated results.
Clients with liver disease often have prolonged clotting times; therefore, provide prolonged pressure at the venipuncture site and monitor the site closely for bleeding.
VI. GLUCOSE STUDIES
A. Fasting blood glucose
- Description a. Glucose is a monosaccharide found in fruits and is formed from the digestion of carbohydrates and the conversion of glycogen by the liver. b. Glucose is the main source of cellular energy for the body and is essential for brain and erythrocyte function. c. Fasting blood glucose levels are used to help diagnose diabetes mellitus and hypoglycemia (Table 11-4).
- Nursing considerations a. Instruct the client to fast for 8 to 12 hours before the test. b. Instruct a client with diabetes mellitus to with- hold morning insulin or oral hypoglycemic medication until after the blood is drawn.
TABLE 11-4 Normal Adult Glucose Values Measurement Setting Normal Value Glucose, fasting 70-110 mg/dL Glucose monitoring (capillary blood) 60-110 mg/dL Glucose tolerance test, oral Baseline fasting 70-110 mg/dL 30-min fasting 110-170 mg/dL 60-min fasting 120-170 mg/dL 90-min fasting 100-140 mg/dL 120-min fasting 70-120 mg/dL Glucose, 2-hr postprandial <140 mg/dL
s
CHAPTER 11 Laboratory Values 121
- Value: 1.6 to 2.6 mg/dL
- Nursing considerations a. Prolonged use of magnesium products causes increased serum levels. b. Long-term parenteral nutrition therapy or exces- sive loss of body fluids may decrease serum levels. C. Phosphorus
- Description a. Phosphorus is important in bone formation, energy storage and release, urinary acid-base buffering, and carbohydrate metabolism. b. Phosphorus is absorbed from food and is excreted by the kidneys. c. High concentrations of phosphorus are stored in bone and skeletal muscle.
- Value: 2.7 to 4.5 mg/dL
- Nursing considerations: Instruct the client to fast before the test.
IX. THYROID STUDIES
A. Description
- Thyroid studies are performed if a thyroid disor- der is suspected.
- Thyroid studies help differentiate primary thyroid disease from secondary causes and from abnor- malities in thyroxine-binding globulin levels. B. Values
- Thyroid-stimulating hormone (also called thyro- tropin): 0.2 to 5.4 microunits/mL
- Thyroxine (T 4 ): 5 to 12 mcg/dL
- Thyroxine, free (FT 4 ): 0.8 to 2.4 ng/dL
- Triiodothyronine (T 3 ): 80 to 230 ng/dL C. Nursing consideration: Test results may be invalid if the client has undergone a radionuclide scan within 7 days before the test.
X. WHITE BLOOD CELL COUNT
A. Description
- WBCs function in the immune defense system of the body.
- The WBC count assesses leukocyte distribution. B. Value: 4500 to 11,000 cells/mm 3 (Table 11-5)
C. Nursing considerations
- A “shift to the left” means that an increased number of immature neutrophils is present in the blood.
- A low total WBC count with a left shift indicates a recovery from bone marrow depression or an infection of such intensity that the demand for neutrophils in the tissue is higher than the capacity of the bone marrow to release them into the circulation.
- A high total WBC count with a left shift indi- cates an increased release of neutrophils by the bone marrow in response to an overwhelming infection or inflammation.
- A “shift to the right” means that cells have more than the usual number of nuclear segments; found in liver disease, Down syndrome, and megaloblastic and pernicious anemia.
Monitor the WBC count closely in clients receiving chemotherapy because of the risk for neutropenia.
XI. HEPATITIS TESTING
A. Description
- Tests include radioimmunoassay, enzyme-linked immunosorbent assay (ELISA), and microparti- cle enzyme immunoassay.
- Serological tests for specific hepatitis virus markers assist in defining the specific type of hepatitis. B. Values
- The presence of immunoglobulin M (IgM) anti- body to hepatitis A virus and the presence of the total antibody to hepatitis A virus identify the disease.
- Detection of hepatitis B core antigen (HBcAg), envelope antigen (HBeAg), and surface antigen (HBsAg), or their corresponding antibodies, constitutes hepatitis B assessment.
- Hepatitis C is confirmed by the presence of anti- bodies to hepatitis C virus.
- Serological hepatitis D virus determination is made by detection of the hepatitis D antigen (HDAg) early in the course of the infection and by detection of anti–hepatitis D virus antibody in the later disease stages.
- Specific serological tests for hepatitis E virus include detection of IgM and IgG antibodies to hepatitis E.
- Hepatitis G virus has been found in some blood donors (donated blood ), IV drug users, hemodi- alysis clients, and clients with hemophilia; how- ever, hepatitis G virus does not appear to cause significant liver disease. C. Nursing consideration: If the radioimmunoassay technique is being used, the injection of radionu- clides within 1 week before the blood test is per- formed may cause falsely elevated results.
TABLE 11-5 Normal Adult White Blood Cell Differential Count Cell Type Count Neutrophils 1800-7800 cells/mm 3 Bands 0-700 cells/mm 3 Eosinophils 0-450 cells/mm 3 Basophils 0-200 cells/mm 3 Lymphocytes 1000-4800 cells/mm 3 Monocytes 0-800 cells/mm 3
s
CHAPTER 11 Laboratory Values 123
XII. HUMAN IMMUNODEFICIENCY VIRUS (HIV)
AND ACQUIRED IMMUNODEFICIENCY
SYNDROME (AIDS) TESTING
A. Description
- Testing detects HIV, which is the cause of AIDS.
- Common tests used to determine the presence of antibodies to HIV include ELISA, Western blot, and immunofluorescence assay (IFA).
- A single reactive ELISA test by itself cannot be used to diagnose HIV and should be repeated in duplicate with the same blood sample; if the result is repeatedly reactive, follow-up tests using Western blot or IFA should be performed.
- A positive Western blot or IFA result is consid- ered confirmatory for HIV.
- A positive ELISA result that fails to be confirmed by Western blot or IFA should not be considered negative, and repeat testing should take place in 3 to 6 months. B. CD4 þ^ T-cell counts
- Monitors the progression of HIV
- As the disease progresses, usually the number of CD4 þ^ T-cells decreases, with a resultant decrease in immunity.
- Normal CD4 þ^ T-cell count is between 500 and 1600 cells/L.
- Generally, the immune system remains healthy with CD4 þ^ T-cell counts higher than 500 cells/L.
- Immune system problems occur when the CD4þ^ T-cell count is between 200 and 499 cells/L.
- Severe immune system problems occur when the CD4 þ^ T-cell count is lower than 200 cells/L. C. CD4-to-CD8 ratio
- Monitors progression of disease.
- Normal ratio is approximately 2:1. D. Viral culture involves placing the infected client’s blood cells in a culture medium and measuring the amount of reverse transcriptase activity over a specified period of time. E. Viral load testing measures the presence of HIV viral genetic material (RNA) or another viral protein in the client’s blood. F. The p24 antigen assay quantifies the amount of HIV viral core protein in the client’s serum. G. Oral testing for HIV
- Uses a device that is placed against the gum and cheek for 2 minutes
- Fluid (not saliva) is drawn into an absorbable pad, which, in an HIV-positive individual, con- tains antibodies.
- The pad is placed in a solution and a specified observable change is noted if the test result is positive.
- If the result is positive, a blood test is needed to confirm the results. H. Home test kits for HIV
- In one at-home test kit, a drop of blood is placed on a test card with a special code num- ber; the card is mailed to a laboratory for testing for HIV antibodies.
- The individual receives the results by calling a special telephone number and entering the spe- cial code number; test results are then given. I. Nursing considerations
- Maintain issues of confidentiality surrounding HIV and AIDS testing.
- Follow prescribed state regulations and proto- cols related to reporting positive test results.
XIII. URINE TESTS (Table 11-6)
XIV. THERAPEUTIC SERUM MEDICATION
LEVELS (Table 11-7)
TABLE 11-6 Normal Adult Values: Urine Tests Name of Test Value Color Pale yellow Odor Specific aromatic odor, similar to ammonia Turbidity Clear pH 4.5-7. Specific gravity 1.016 to 1. Glucose <0.5 g/day Ketones None Protein None Bilirubin None Casts None to few Crystals None Bacteria None or <1000/mL Red blood cells <3 cells/HPF White blood cells �4 cells/HPF Chloride 110-250 mEq/24 hr Magnesium 7.3-12.2 mg/dL Potassium 25-125 mEq/24 hr Sodium 40-220 mEq/24 hr Uric acid 250-750 mg/24 hr HPF, High-powered field.
124 UNIT III Nursing Sciences