Download Laboratory Values Interpretation Resource and more Exercises Physiology in PDF only on Docsity!
Updated 2017
Laboratory Values Interpretation Resource
Academy of Acute Care Physical Therapy – APTA Task Force on Lab Values
2017 Members James Tompkins, PT, DPT | Co-Chair Traci Norris, PT, DPT, GCS | Co-Chair Kim Levenhagen, PT, DPT, WCC | Co-Chair Kate Adeletti, PT, DPT, NCS Courtney Bryan, PT Malinda Brown-Crowell, PT, DPT, GCS Jamie Dyson, PT, DPT Komal Shah, PT, DPT, NCS Kathy Swanick, PT, DPT, OCS Julie Terrell, DPT Risa Maruyama, PT, NCS Caitlin Price
2012 Members Roya Ghazinouri | Chair Samidha Deshmukh Sharon Gorman, PT, DPTSc, FNAP, GCS Angela Hauber Mary Kroohs Elizabeth Moritz Babette Sanders, PT, DPT, MS, FAPTA Darin Trees, PT, DPT, CWS
2008 Members Holly McKenzie, PT, DPT Dawn Piech, PT, MPT Jim Smith, PT, DPT, MA
Approved by Academy of Acute Care Physical Therapy – APTA Board of Directors: 8/2008, 12/2011, 1/
Evolution of the 2017 Edition of the Laboratory Values Interpretation
Resource by the Academy of Acute Care Physical Therapy
As emerging research regarding early mobilization and advancements in medical practice is evolving, the Academy of Acute Care Physical Therapy – American Physical Therapy Association Task Force on Lab Values took on the mission of updating the Laboratory Values Interpretation Resource to better accommodate practitioners’ needs. The task force consisted of physical therapists from across the country in various acute care settings. Based on practitioners’ feedback, this document was adapted to improve usability in the busy acute care setting.
The task force set out to use current literature from the past five years. Original sources were captured and referenced for each item. The task force collaborated with university librarians to ensure the comprehensiveness of the literature search. After consulting with clinical lab scientists, the task force was unable to identify a gold standard in regard to a laboratory guide listing reference values (see disclaimer). For the purpose of consistency, the task force decided to use the reference values from one reputable laboratory values textbook, unless there was a clinical practice guideline related to that laboratory value. Each laboratory test captured in this 2017 version has a brief explanation of the test or laboratory panel, reference values, clinical presentation, and clinical implications. In response to unmet clinical decision-making needs from membership thus far, updates have been made to the content from the previous version, and a new point-of- care document listing key laboratory tests has been created for this version. As the task force closes its current work on this project, it does so in the understanding that this living document needs continuous updating to ensure that the needs of clinicians will be appropriately accommodated.
Disclaimer
The reference ranges and recommendations in this resource are based on the current, best-available evidence. Considering the absence of a universal reference range for any of the more than 5,000 lab tests in existence, accredited laboratories are required to establish and validate their reference values at least annually. Thus, any given result should be interpreted based on the reference value of the laboratory in which the test was performed. Reference values must be updated each time a new reagent kit or diagnostic instrument is added. In addition, differences in patient populations (ethnicity, age, gender, behaviors, and culture) might result in variability of reference ranges. Abnormal values are defined as those results that are outside a specific range obtained from a cohort of healthy individuals. 1
Physical therapists have the professional responsibility to provide excellent care, adhere to high standards, and collaborate with other healthcare providers to achieve optimal health outcomes for their patients. Acute care physical therapists work in an environment that is quickly evolving and therefore should be knowledgeable regarding critical laboratory values and safe mobility recommendations. Lundberg (1972) defined a critical value as a “physiological state at such variance with normal as to be life threatening unless something is done promptly and for which some corrective action can be taken.” 2 As critical values might evolve quickly in the acute care setting, physical therapists should be vigilant in reevaluating safe and effective patient management. Although the recommendations made in this document are evidence-based, the final judgment regarding the appropriateness of particular physical therapy interventions should be made by the clinician. The goal of clinical standardization is not to produce rigid guidelines; it is to establish an evidence- and consensus- founded treatment approach that could change and evolve based on the patient’s clinical presentation and individual values, as well as expectations and preferences.
Today’s electronic health record environment allows for fast retrieval of laboratory results. Test names and specific value ranges are easily visualized with high-priority findings (i.e. critical alerts), having predetermined indicators or color highlights to bring attention to medical team.
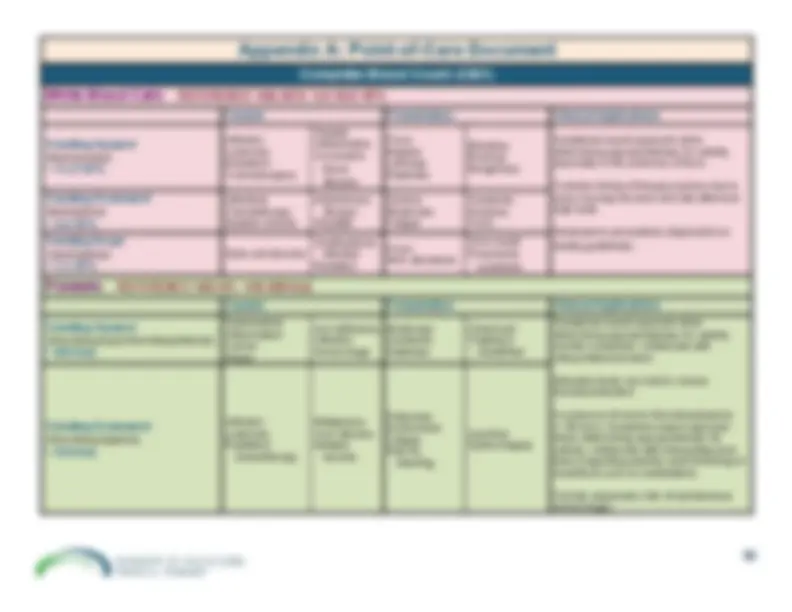
9. Bleeding Ratio/Viscosity a. International Normalized Ratio (INR) b. Activated Partial Thromboplastin Time (aPTT) c. Prothrombin Time (PT) d. Anti-Factor Xa Assay e. D-Dimer f. Algorithm for Mobilizing Patients with Known Lower-Extremity Deep Vein Thrombosis 10. Cardiovascular-Specific Labs a. Troponin b. B-Type Natriuretic Peptide (BNP) c. Creatinine Kinase (CK) 11. References Appendix A: Point-of-Care Document
1. Understanding Lab Values
a. Trends
Physical therapists should not rely exclusively on a single laboratory finding; instead, they should also consider a variety of other clinical factors. For instance, clinicians should be aware of the time the laboratory specimen was drawn, potential drug interactions, or the patient’s recent meals. Likewise, it is important to understand the significance of trends in the values over time. Electrolyte panels might change with intravenous infusions, medications, and diet. Patients with chronic medical conditions, such as anemia, might be asymptomatic during exercise, while a patient with a precipitous drop in hemoglobin and hematocrit might require urgent medical attention.
When a patient presents with symptoms of a suspected myocardial infarction (MI), cardiac biomarker laboratory tests are ordered to assist with a differential diagnosis. Cardiac biomarkers are materials released into the bloodstream when the heart is under stress. Typically, under normal circumstances, these substances do not appear in circulation; however, when there is insufficient blood flow to the heart, markers associated with myocardial injury increase in a predictable fashion. Up to 80% of patients with an acute MI will present with an elevation of troponin within 3 hours of onset of chest pain. 3
However, not all patients with cardiac impairments present with obvious symptoms, and they might not have undergone diagnostic testing. It is not uncommon for patients with complex comorbidities and non-specific and subtle symptoms, including unexplained fatigue and weakness, to be referred to acute care physical therapy. It is, therefore, prudent for therapists to be aware of the presence of cardiac biomarkers and potential delays in the diagnosing of cardiac ischemia.
b. Risk vs. Benefit Considerations of the Therapeutic Intervention The fundamental consideration when reviewing patient laboratory findings is toward determining an appropriate plan of care and weighing the anticipated benefit of a therapy intervention against the potential risk to the patient.
Physical therapists should carefully anticipate the physiological changes that might have occurred whenever a laboratory value is out of range. They should also be aware of the heightened risk level if a value should fall into the critical range. It is critical to understand pertinent lab values and the subsequent potential of adverse events when practicing in this kind of practice setting. In weighing risks and benefits, physical therapists should also consider the potential benefits from a therapeutic plan that increases the patient’s activity. Immediate risks and benefits, as well as the longer-term consequences over the episode of care, should be assessed. To fully explore the potential effects of physical therapy intervention, collaboration with other members of the interprofessional medical team is often necessary. It is prudent and congruent with standards of professionalism for physical therapists to assist with the development of facility policies, procedures, and protocols to aid in the clinical decision-making process regarding the use of lab values in determining the intensity level of therapeutic interventions.
c. Acute vs. Chronic Considerations of the Therapeutic Intervention
In addition to comparing a patient’s specific laboratory values to known reference ranges for a population, clinical decisions require understanding of the patient’s symptoms and the dynamic physiological changes indicated by the laboratory tests. As an example, acute laboratory value changes, such as those associated
Table 1: Definitions pertaining to sex and gender roles.^12
Term Definition Sex Categorical differentiation between men and women, assigned at birth based on briefvisual examination of external genitalia.
Gender Binary social construct involving characteristics distinguishing men from women. Gender Identity Person’s sense of being male or female.
Transsexual Outdated term for person who feels they were assigned the incorrect sex.
Transgender Overarching term for persons with various identities and expressions that areassociated with assignment of incorrect sex.
Transition Legal, medical, and surgical processes that a transsexual person might experience tocorrect the incongruence of incorrect sexual assignment.
Transwoman A person who identifies as female but was assigned the male sex. Transman A person who identifies as male but was assigned the female sex.
Individual patients might be in the process of transitioning to their preferred gender through medical (i.e., hormone replacement therapy), surgical (i.e., gender reassignment surgery), and/or legal (i.e., amending legal documents to reflect gender identity) means to correct incongruence of sex. Physical therapists should determine if patients in transition are currently under medical treatment for this transition, which could occur prior to or in conjunction with surgical transition, and will be continued after surgical transition. If the patient is on hormone replacement therapy, physical therapists should use the transitioned gender to determine the reference value. If the patient is not receiving hormone therapy, physical therapists should use the patient’s biological sex to determine the reference value. For example, a transwomen on estrogen replacement therapy should have her lab values compared to normal values of females due to the effects of estrogen on her physiology, whereas a transman on testosterone should have his lab values compared to those of males due to the effects of testosterone on his physiology. The key factor is not whether the medical record assigns a patient a particular sex or whether the patient has undergone sexual reassignment surgery, but whether patients are taking hormone therapy that will affect their physiology and lab chemistry. Knowing the medical transition status of a transsexual person reduces the risk of misinterpretation of lab values and ensure correct application of normal reference values consistently. 12
e. Age Considerations
This outline was created to assist the clinician with lab value considerations for the general population. The clinician should be aware that “norms” are created for the healthy adult, and each patient’s lab values should be interpreted within the context of the patient’s current medical status. That is to say, when reading the value ranges in this section, be aware that considerations for mobility might vary based on the patient’s age and current medical condition. For example, an 18-year-old boy with a below-normal hematocrit might tolerate this lower level better than a 90-year-old male with the same low hematocrit. Thus, a clinician might be more willing to mobilize a patient with a below-normal value who is younger and has overall more reserve. Conversely, patients being treated for certain blood cancers can more safely participate in mobility with lower platelet levels vs. the general population, the latter likely being at an increased risk of bleeding.
We have not included lab ranges for the pediatric population. Please refer to the Academy of Pediatric Physical Therapy for more information, as normative values might differ from the adult populations.
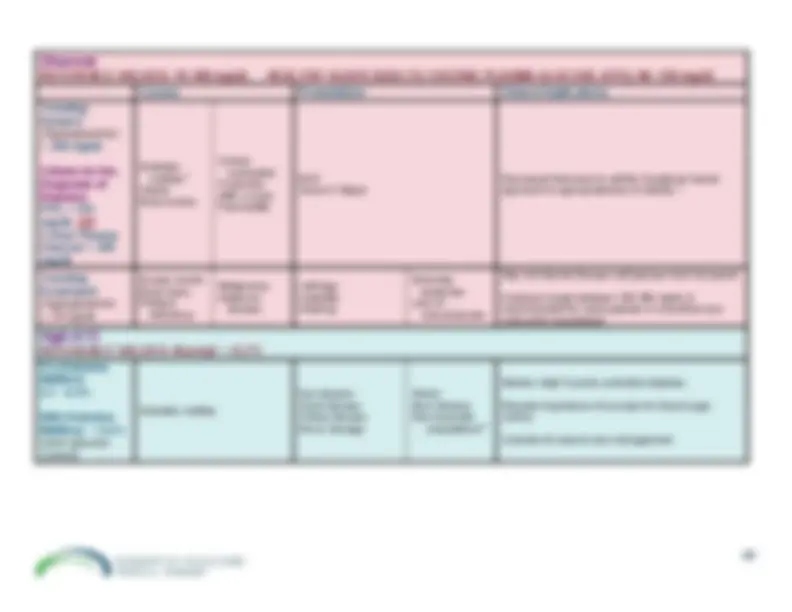
2. Complete Blood Count (CBC)Complete Blood Count (CBC) Provides results regarding the concentration of red bloodcells, white blood cells, and platelets in a blood sample.
1
Causes
Presentation
Clinical Implications
White Blood Cells Routine test to identifythe presence ofinfection, inflammation,allergens.
REFERENCEVALUES
13
^10
9 /L
Trending Upward
(leukocytosis)
13
9 /L
InfectionLeukemiaNeoplasmTraumaSurgerySickle-cell diseaseStress/painMedication-inducedSmokingObesityCongenitalChronic inflammationConnective tissue
disease
FeverMalaiseLethargyDizzinessBleedingBruisingWeight loss
(unintentional) LymphadenopathyPainful inflamed joints
Symptoms-based approach whendetermining appropriateness for activity,especially in the presence of fever.Consider timing of therapy session dueto early-morning low level and late-afternoon high peak.
14
TrendingDownward (leukopenia)
13
9 /L
Viral infectionsChemotherapyAplastic anemiaAutoimmune diseaseHepatitis
AnemiaWeaknessFatigueFeverHeadacheShortness of breath
Symptoms-based approach whendetermining appropriateness for activity,especially in the presence of fever.
14
TrendingDownward (neutropenia)
13
9 /L
9 /L =
moderateneutropenia< 0.5 10
9 /L=
severe neutropenia
Stem cell disorderBacterial infectionViral infectionRadiation
Low-grade feverSkin abscessesSore mouthSymptoms of
pneumonia
Neutropenic precautions (dependent onfacility guidelines).
14
Symptoms-based approach whendetermining appropriateness for activity,especially in the presence of fever.
14
Complete Blood Count (CBC)
Causes
Presentation
Clinical Implications
Hemoglobin(cont.) Assess anemia, blood loss,bone marrow suppression
REFERENCE VALUESMale:
14-17.4 g/dL
13
Female:
12-16 g/dL
13
Note:
Values are slightly
decreased in elderly.
13
TrendingDownward^ (anemia)
HemorrhageNutritional
deficiency NeoplasiaLymphomaSystemic lupus
erythematosus SarcoidosisRenal diseaseSplenomegalySickle cell anemiaStress to bone
marrow RBC destruction
Decreased
endurance Decreased activity
tolerance PallorTachycardia
Monitor vitals including SpO
to predict tissue 2
perfusion. May present with tachycardia and/ororthostatic hypotension.Medical team might monitor patients with pre-existingcerebrovascular, cardiac, or renal conditions forineffective tissue perfusion related to decreasedhemoglobin.
18
If <8 g/dL: Symptoms-based approach whendetermining appropriateness for activity; collaboratewith interprofessional team (regarding possible needfor/timing of transfusion prior to mobilization).
13-15,
Consultation with the interprofessional team as whileas monitoring of signs and symptoms is imperativesince hemoglobin levels and blood transfusions isindividualized.
18
^
hospitalized patients who arehemodynamically stable and asymptomaticmay transfuse at 7 g/dL ^
post surgical cardiac or orthopedic patientsand those with underlying cardiovasculardisease may transfuse at 8 g/dL. ^
patients with hematological disorders,oncological disorders and severethrombocytopenia ,or chronic transfusion-dependent anemia: no transfusion thresholdrecommendation is available.
Complete Blood Count (CBC)
Causes
Presentation
Clinical Implications
Hematocrit Assess blood loss andfluid balance.
REFERENCEVALUESMale:
13
Female:
13
Note:
Values are slightly decreased inthe elderly.
(^13)
Trending Upward
(polycythemia)
BurnsEclampsiaSevere dehydrationErythrocytosisTend to be elevated
with those living inhigher altitude Hypoxia due to chronic
pulmonary conditions(COPD, CHF)
FeverHeadacheDizzinessWeaknessFatigueEasy bruising or
bleeding
Low critical value (<15-20%) cardiacfailure or death.
13-
High critical value (>60%) spontaneousblood clotting.
13-
Symptoms-based approach whendetermining appropriateness for activity;monitor symptoms; collaborate withinterprofessional team
13-
TrendingDownward^ (anemia)
LeukemiaBone marrow failureMultiple myelomaDietary deficiencyPregnancyHyperthyroidismCirrhosisRheumatoid arthritisHemorrhageHigh altitude
Pale skinHeadacheDizzinessCold hands/feetChest painArrhythmiaShortness of breath
Patient might have impaired endurance;progress slowly with activity.Monitor vitals including SpO
to predict 2
tissue perfusion. Might present withtachycardia and/or orthostatichypotension.Medical team might monitor patientswith pre-existing cerebrovascular,cardiac, or renal conditions forineffective tissue perfusion related todecreased hematocrit.
18
If < 25%: Symptoms-based approachwhen determining appropriateness foractivity; collaborate withinterprofessional team (regardingpossible need for/timing of transfusionprior to mobilization)
13-15,
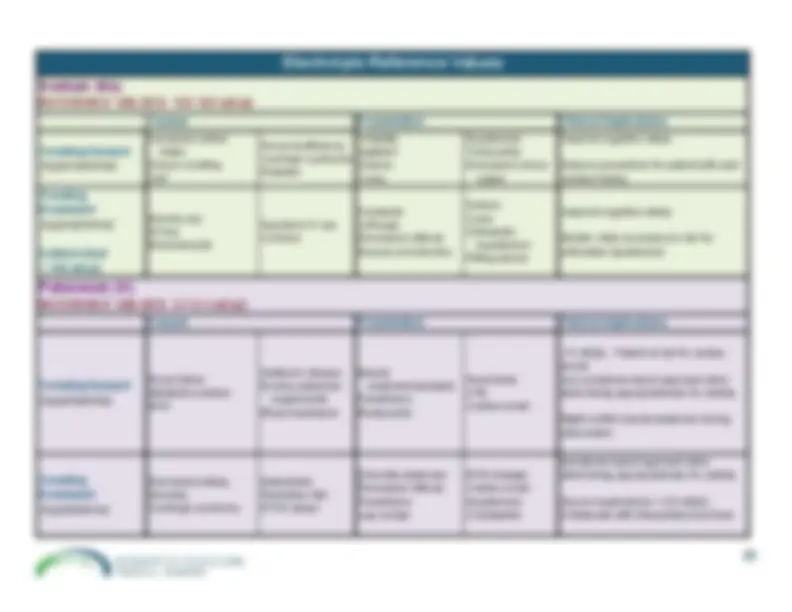
Electrolyte Reference Values
Causes
Presentation
Clinical Implications
Calcium (Ca) Important for boneformation, cell divisionand growth, bloodcoagulation, musclecontraction, andrelease ofneurotransmitters.
REFERENCEVALUES8.6-10.3 mg/dL
13
Hypercalcemia^ (high levels ofcalcium in blood) Trending Upward
Excessive calcium
supplements/antacids Bone destruction –
tumor ImmobilizationFractureExcessive vitamin DCancerRenal failure
20
Ventricular dysrhythmiasHeart blockAsystoleComaLethargyMuscle weaknessDecreased reflexesConstipationNausea/vomiting
21
Symptoms-based approach whendetermining appropriateness foractivity.
1,20,
Hypocalcemia (low levels of calcium
in blood) TrendingDownward
ETOH abusePoor dietary intakeLimited GI absorptionPancreatitisLaxative use
21
AnxietyConfusionAgitationSeizureEKG changesFatigueNumbness/tinglingIncreased reflexesMuscle cramps
21
Might have impaired cognitiveabilities.Symptoms-based approach whendetermining appropriateness foractivity.
1,20,
Chloride (Cl) Important for fluidbalance and acid basestatus.
REFERENCEVALUES98-108 mEq/L
13
Hyperchloremia^ (high levels ofchloride in blood) Trending Upward
High-salt, low-water dietHypertonic IVMetabolic AcidosisRenal failure
21
LethargyDecreased level of
consciousness WeaknessEdemaTachypneaHypertension (HTN)Tachycardia
21
Determine if appropriate fortreatment if exhibiting decreasedlevel of consciousness.
21
Hypochloremia (low levels of chloride
in blood)
Trending Downward
Low salt dietWater intoxicationDiuresisExcessive vomiting
and/or diarrhea
21
AgitationIrritabilityHypertonicityIncreased reflexesCrampingTwitching
21
Monitor level of consciousness andmotor function.
1,20,
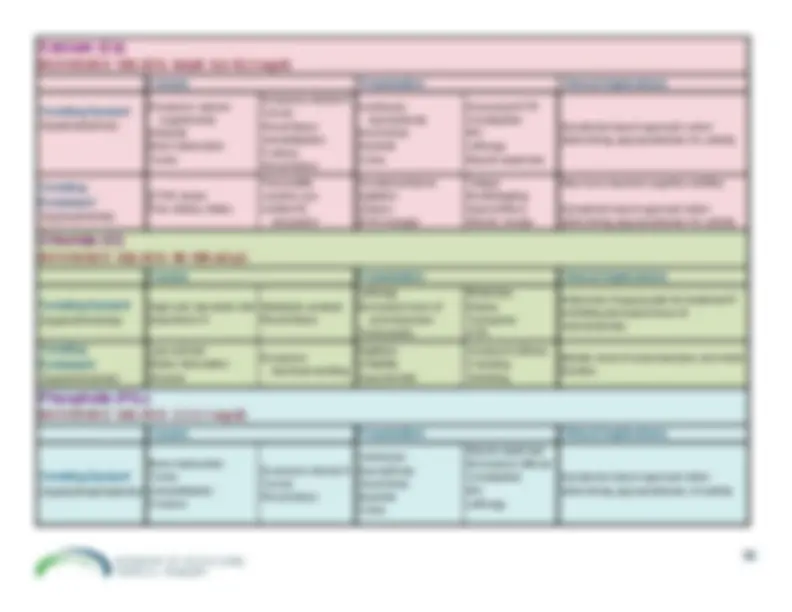
Electrolyte Reference Values
Causes
Presentation
Clinical Implications
Phosphate(PO
) 4
Necessary for boneformation, acid-basebalance, and storageand transfer of energy.
REFERENCEVALUES2.3-4.1 mg/dL
13
Hyperphosphatemia
(high level of phosphate in blood)^ Trending Upward
Bone destruction –
tumor ImmobilizationFractureExcessive vitamin DCancerRenal failure
21
Ventricular dysrhythmiaHeart blockAsystoleComaLethargyMuscle weaknessDecreased reflexesConstipationNausea/vomting
21
Symptoms-based approach whendetermining appropriatenessof activity.
1,20,
Hypophosphatemia
(low level of phosphate in blood) Trending Downward
ETOH abusePoor dietary IntakeLimited GI absorptionPancreatitisLaxative Use
21
AnxietyConfusionAgitationSeizureEKG changesFatigueNumbness/tinglingIncreased reflexesMuscle cramps
21
Might have impaired cognitiveabilities.Symptoms-based approach whendetermining appropriatenessfor activity.
1,20,
Magnesium(Mg) Concentrated in boneand muscle;concentration primarilyregulated by kidneys(ordered separatelyfrom BMP).
REFERENCEVALUES1.2-1.9 mEq/L
13
Hypermagnesemia
(high level of magnesium in blood)^ Trending Upward
Increased intake of
antacids/magnesiumcitrate Renal failureLeukemiaDehydration
21
DiaphoresisN/VDrowsinessLethargyWeakness flaccidityDecreased reflexesHypotensionHeart block
21
Symptoms-based approach whendetermining appropriatenessfor activity.
1,20,
Hypomagnesemia
(low level of magnesium in blood) Trending Downward
ETOH abuseEating disordersDiuresisDKAMedications
21
Increased reflexesTremorsSpasticitySeizuresNystagmusEKG changes (prematureventricular contraction(PVC)
v-tach
v-fib )
Emotional lability
21
Symptoms-based approach whendetermining appropriatenessfor activity.
1,20,
5. EndocrineGlucose Reference Values
Causes
Presentation
Clinical Implications
Glucose
Measures blood glucose at the timesample obtained.
REFERENCE VALUES70-100 mg/dL FASTING PLASMA GLUCOSE (FPG)90-130 mg/dL Criteria for the Diagnosisof Diabetes
24
FPG > 126 mg/dL
OR
2-hour Plasma Glucose > 200 mg/dL
HyperglycemicTrending Upward^ (> 200 mg/dL)
Diabetes mellitus
21
SepsisBrain TumorsCertain medicationsIV glucoseAfter a mealPancreatitis
Diabetic
ketoacidosis Severe fatigue
21
Decreased tolerance toactivity.
(^21)
Symptoms-based approach toappropriateness ofactivity.
1,20,
Hypoglycemic Trending Downward
(< 70 mg/dL)
Excess insulin
21
Brain injuryPituitary deficiencyMalignancyAddison's disease
LethargyIrritabilityShakingExtremity
Weakness Loss of
consciousness
21
May not tolerate therapy untilglucose level increased.
21
A glucose target between140-180 mg/dL isrecommended for mostpatients in noncritical careunits while hospitalized.
(^24)
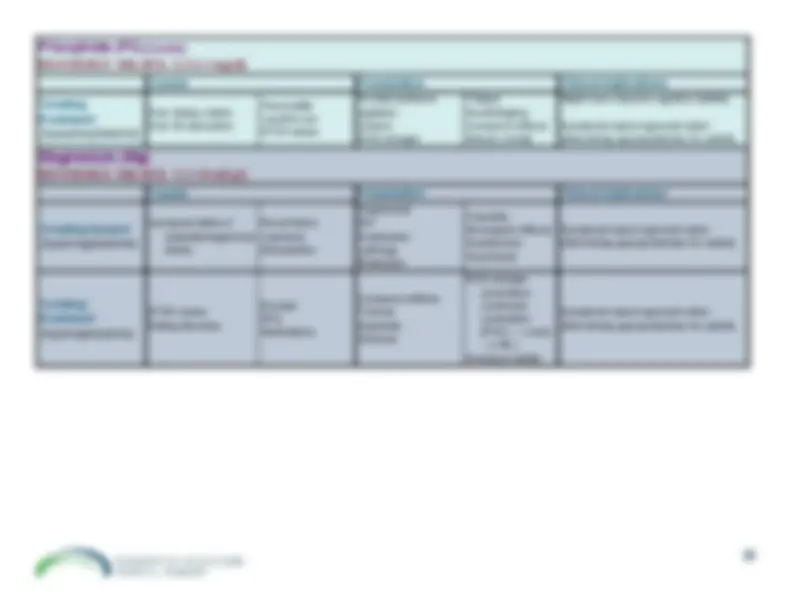
Hgb A1C Reference Values
Causes
Presentation
Clinical Implications
Hgb A1C
Shows the average level of blood glucosecontrol over the previous 3 months.
REFERENCE VALUESNormal: < 5.7%^ Pre-diabetes mellitus: 5.7 - 6.4%With diabetes mellitus: > 6.5%^ (poor glucose control)
Diabetes mellitus
Eye diseaseHeart diseaseKidney diseaseNerve damageStrokeGum diseaseNon-traumatic
amputations
24
Monitor vitals if poorly controlleddiabetes.Educate importance of exercise forblood sugar control.Consider for wound caremanagement.
24
Thyroid Function Reference Values
1
Presentation
Clinical Implications
Thyroxine (T4)
REFERENCE VALUESTotal 4.5-11.5 μg/dL Triiodothyronine (T3)
REFERENCE VALUES80-200 ng/dL Thyroid – StimulatingHormone (TSH)
REFERENCE VALUES0.3-3.0 U/mL Note:
Increased TSH and
decreased T4 = thyroid disease;decreased TSH = pituitarydisease
Hyperthyroidism Increased T3 and/or T
TremorsNervousness/labilityWeakness/muscular atrophyIncreased reflexesFatigueTachycardia – increased cardiac
output Arrhythmias (atrial fibrillation)HypotensionChronic periarthritisProximal weaknessAlso affects: integumentary,
gastrointestinal and genitourinarysystems
Decreased exercise tolerance – bothstrength and capacity.Monitor heart rate and bloodpressure.Patient at risk for dysrhythmiasduring exercise.Patient in a hypermetabolic state willdeplete nutrients quickly withexercise.
1
HypothyroidismIncreased TSH Decreased T3 and or
T
Slow Speech/HoarsenessSlow Mental FunctionAtaxiaProximal muscle weaknessCarpel tunnel syndromeProlonged reflexesParesthesiaMuscular/joint edemaBack painBradycardiaCHFPoor peripheral circulationHyperlipidemiaHTNAlso affects: integumentary,
gastrointestinal and genitourinarysystems
Hypothyroidism – frequentlyaccompanied by myalgia and CKelevation.More prone to skin tears.Activity intolerance; should improvewith treatment of hypothyroidism.Rhabdomyolysis, although rare, canappear in the presence of heavyexercise, alcohol, or medications.Monitor heart rate – bradycardia.
1
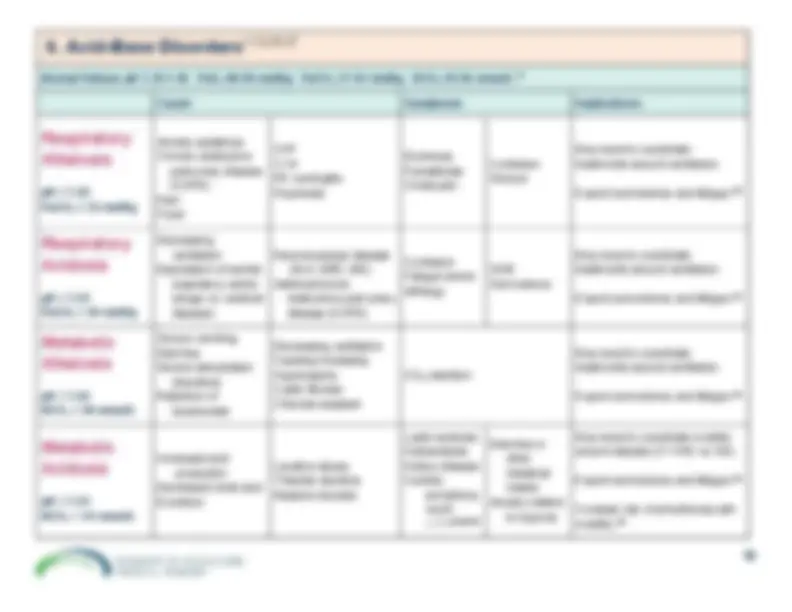
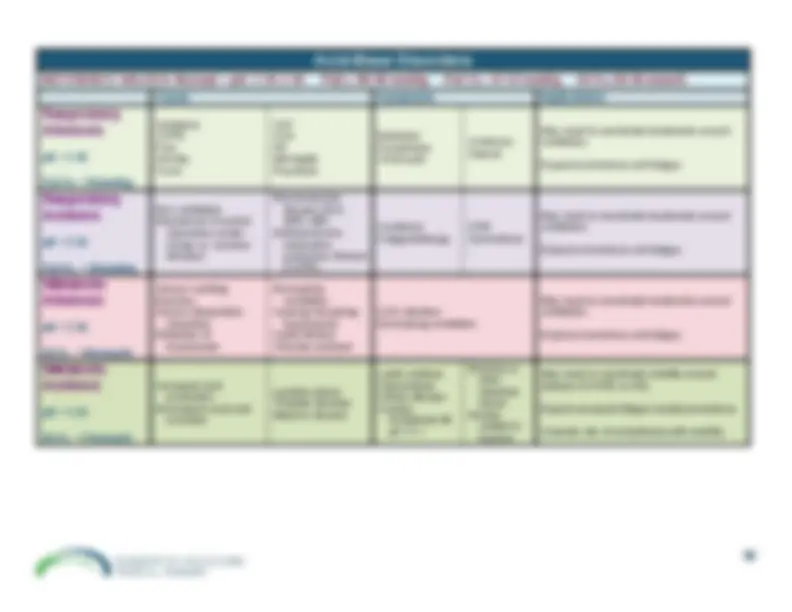
Anion Gap
The difference between free cations and free anions. The major free cations are Sodium (Na+) and Potassium (K+). The major anions are Chloride(Cl
−) and Bicarbonate (HCO
The anion gap (AG) it is calculated from the equation AG= [(Na+) + (K+)]
[(Cl
−) + (HCO
3 )]- note- K+ may or may not be included- refer to your
specific lab to know if K+ is included in Anion Gap REFERENCE VALUE 8 to 16 mEq without K+12 to 20 mEq with K+ Clinical Considerations – Elevated Anion Gap
^
ETOH Ketoacidosis ^
Uncontrolled diabetes-Increased ketoacids ^
Methanol intoxication- Increased formic acid ^
Tissue hypoxia-Increased lactic acid ^
Ketogenic diet ^
Fasting ^
Poisoning- salicylate, ethynol, methanol
Clinical Decisions Use a systems-based approach based on the cause of the elevated AG level, not the value itself.
7. Liver Function/Hepatic PanelLiver Function/Hepatic Panel ReferenceRanges Assesses the liver’s ability to clear bilirubin, totalprotein, and albumin.
Causes
Presentation
Clinical Implications
Serum Albumin Half-life of 21 days. 3.5-5.2 g/dL
13
SerumPrealbumin Half-life 2 days; detectscurrent nutritional statuswithin a patient's body.
13
19-39 mg/dL
13
0-5 mg/dL = severeprotein depletion5-10 mg/dL = moderateprotein depletion10-15 mg/dL (mildprotein depletion)
13
TrendingUpward
Severe infectionsCongenital disordersSevere dehydrationHepatitisChronic inflammationTuberculosisOverdose of cortisone
medications CHFRenal DiseaseCancer
21
Clinical features are
dependent on thecause (i.e. renal,cardiac, TB, etc.)
21
Assess integumentary dailyCollaborate with the interprofessionalteam regarding nutrition
31
TrendingDownward
InfectionNutritional compromiseInflammationLiver diseaseCrohn's diseaseBurnsMalnutritionThyroid disease
21
Peripheral edemaNon-healing woundHypotension
21
Assess integumentary daily.Collaborate with the interprofessionalteam regarding nutrition.Low levels occur with prolongedhospital stay.
13
Serum Albumin: < 3.0 g/dLnutritionally compromised; < 2.8 g/dLgeneralized symmetrical peripheraledema, poor wound healing, potentialdrug toxicitySerum Pre-Albumin: < 10 g/dLsignificant nutritional risk, poor woundhealing, generalized edema