


Overview
•- Indirect cholinergic agonism (AchE
inhibition)
•- Muscarinic antagonism (emphasis on
drugs and organ effects)
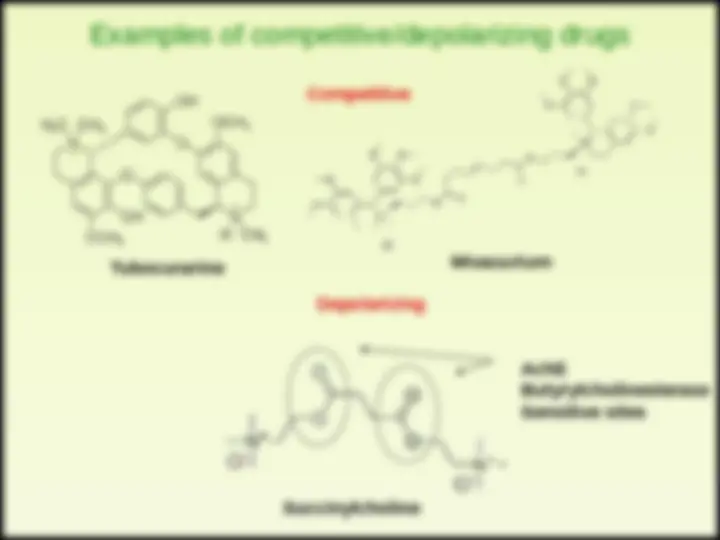
•- Nicotine-Ach receptor (emphasis on
drugs and therapeutics)










Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
An overview of indirect cholinergic agonists, focusing on acetylcholine esterase inhibitors and muscarinic antagonists. It covers the mechanisms of indirect agonism, the effects and therapeutic uses of these inhibitors, and the role of muscarinic antagonists. The document also includes information on the history and sources of relevant drugs, their effects on the body, and antidotes.
Typology: Lecture notes
1 / 27

This page cannot be seen from the preview
Don't miss anything!
Inhibitors of acetylcholinesterase
Increase acetylcholine concentration and lifetime by
inhibiting degradation
Act by binding to AchE active site causing reversible
(non covalent) or long lasting (covalent modification)
both sympathetic and parasympathetic
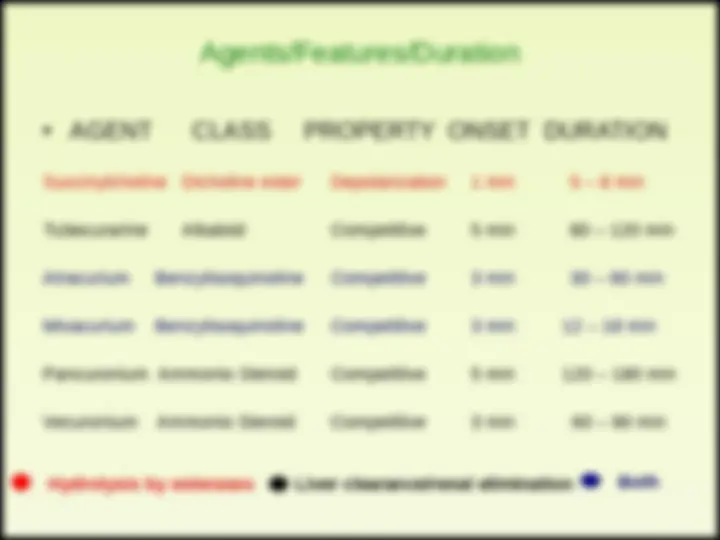
USES Approx Duration
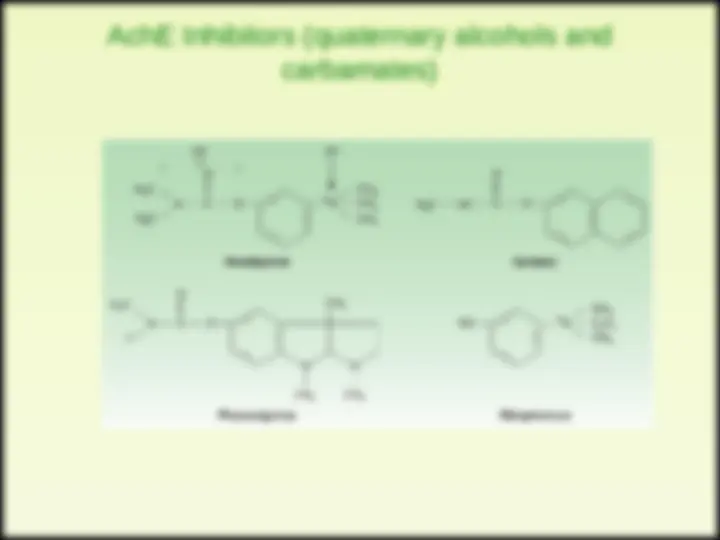
ALCOHOLS
Edrophonium Myasthenia gravis 5 – 15 minutes
arrythmias
CARBAMATES
Neostigmine Myasthenia gravis 0.5 – 2h
Pyridostigmine Myasthenia gravis 3 – 6h
Physostigmine Glaucoma 0.5 – 2h
Demecarium Glaucoma 4 – 6h
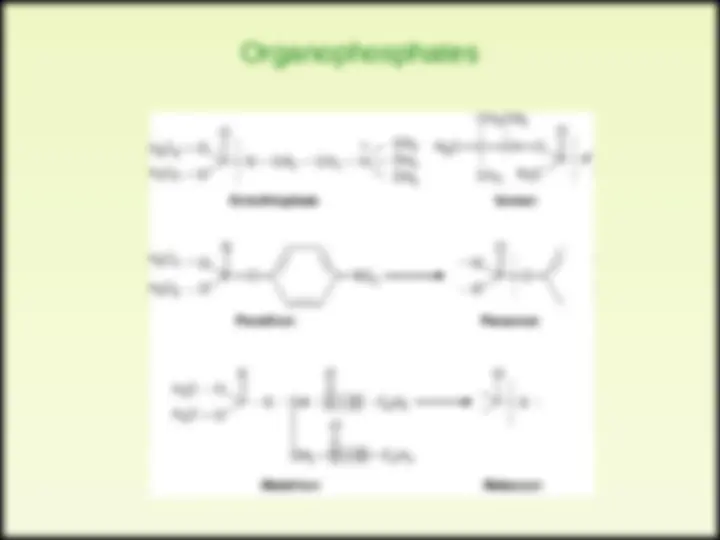
Organophosphates
Echotiophate Glaucoma 100 h (> 4 days)
1 - maintenance of vital signs (respiration particularly
important)
2 - Decontamination (to avoid further absorption)
3 - Atropine parenterally (to minimize muscarinic effects)
as required
4 - Rescue of AchE activity with Hydroxylamines
(Pralidoxime, Diacetylmonoxime)
ATROPINE
SCOPOLAMINE
ATROPINE
SCOPOLAMINE
Attropa belladona
(competitive inhibitors)
blood-brain barrier
scopolamine even at low doses has prominent CNS effects.
poisoning
Jimson plant leaves burned in India to treat Asthma (1800) purification
of atropine (1831)
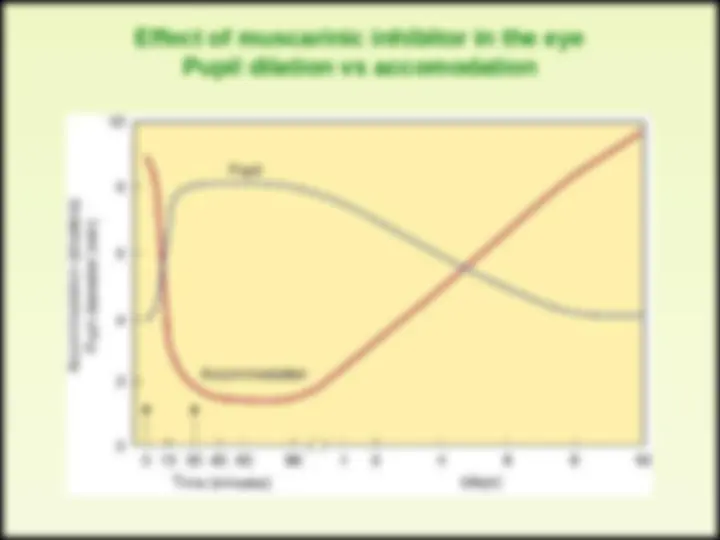
Effect of muscarinic inhibitor in the eye
Pupil dilation vs accomodation
Graphic summary of atropine effects
CNS Benztropine Treat Parkinson’s disease
Scopolamine Prevent/Reduce motion sickness
Eye Atropine Pupil dilation
Bronchi Ipatropium Bronchodilate in Asthma, COPD
GI Methscopolamine Reduce motility/cramps
GU Oxybutinin Treat transient cystitis
Postoperative bladder spasms
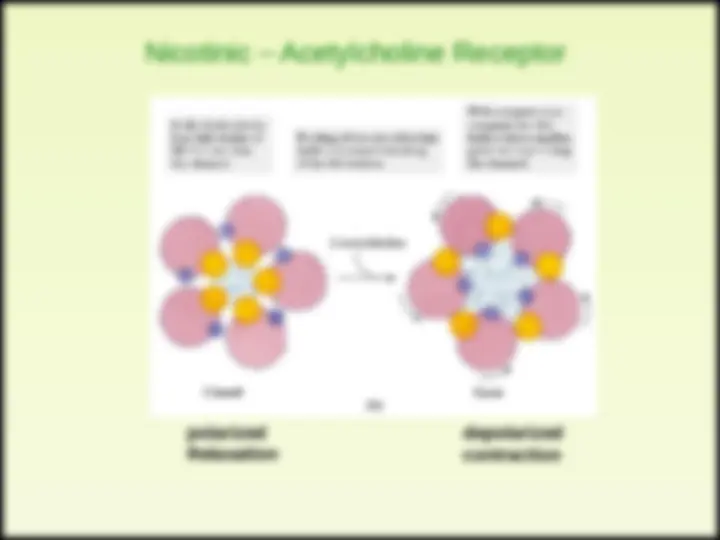
polarized
Relaxation
depolarized
contraction