Download Lecture 5 - Lung Diseases and more Lecture notes Radiology in PDF only on Docsity!
Radiology Team
Lecture 5
Lung Diseases
Done by:
• Abdulrahman AlMtairi
• Abdulelah AlMtairi
Edited by:
• Ahmed Alsaleh
• Nouf Alharbi
Color Index:
- Important • Females’ notes • Males’ notes • Explanations
★ Before starting, please check our Radiology editing file
Lung Diseases
MASS Vs. DIFFUSE INFILTERATION:
MASS DIFFUSE INFILTERATION
- The basic diagnostic instance is to detect an abnormality.
- In both of the cases, there is an abnormal opacity “consolidation”.
- In this case , the opacity would best be described as a mass because it Has edges well-defined (clear outline)3-D STRUCTURE “mass like orange”
- We can see the mass in PA and lateral views which prove the 3D nature of the mass.
- In lateral view appears oval like shape “3D”. - In this case, has an opacity that is poorly defined (Not clear outline). This is airspace disease such as pneumonia (diffuse disease). - Involve large space of the lung, flat and diffused. - In lateral view there will be a change in its appearance.
❖ Consolidation = as pneumonia
❖ Nodules = small
❖ Mass = large
❖ Atelectasis = Lung collapse
❖ Interstitial = diffuse lung disease
PLEURAL BASED LESION
FISSURES
- If the mass arises from the pleura (peripheral mass) it is called “Pleural Based Lesion” by this name it can help us to minimize and know the Deferential diagnosis.
- The Deferential diagnosis of pleural based masses is different, it is either pleural lesion or metastasis
- If there is a lesion in the core of the lung the first and the most important DDx is bronchogenic carcinoma
Encysted pleural effusion of transverse fissure (red arrow) and oblique fissures (green arrow), so when we saw the pathology the fissure outlines becomes more clearly
One of the most important things in lung X-Ray is the fissures : It has 2 benefits:
- It shows us the lung anatomy (upper, middle, lower lobes)
- The fissure are movable, if it moves up or down on x-ray it indicates something (pathology)
ATELECTASIS Vs. Consolidation
ATELECTASIS Consolidation
Loss of volume of lobe, segment or sub segment of the lung.
Loss of air in lobe, segment or sub segment of the lung. Example: collapse (lung) Example: pneumonia (lobe)
Major differentiating factors between atelectasis and
pneumonia:
- Volume loss
- Associated ipsilateral shift
(trachea and pleura will try
to fill the collapsed area )
- Linear, Wedge-shaped
- Apex at hilum
- Normal or increase volume
- No shifting, or if present then
contralateral
process
Air bronchograms can occur in both.
Sometimes consolidation and collapse happens together but it’s rare, so there will be loss of volume and some replacement of air.
PNEUMONIA VS ATELECTASIS
Pic 1 Pic 2
Pic 1 : in PA view there is an area of consolidation, is there any loss of volume or no?? We did a lateral view and we found opaque area :
- the green line → normal position of transverse and oblique fissures.
- red line → is the collapsed right middle lobe. We can see that there is loss of volume because the fissures has changed there position from the green to the red lines.
- There is displacement of the trachea toward the side that loss the volume in atelectasis “Known as effective loss”.
Pic 2 : middle lobe consolidation typically pneumonia
Localizing disease from the silhouette sign:
Lobar Atelectasis:
- Best sign – shift of a fissure
- Rapid development and clearance
- Air bronchograms if non-obstructive Secondary signs:
- Mediastinal shift
- Elevated diaphragm
- Ribs closer together
- Vague increased density
Right Upper lobe Atelectasis:
Pic 1 Pic 2
Pic 1 : patient presented with fever, they put intratracheal tube and after they put the tube, he gets dyspnea and after that chest x ray was done and they found : right upper lobe atelectasis. The patient took antibiotic and the proper treatment. They also remove the tube and they did follow up chest x ray.
Pic 2 : they found the transverse line come back to its normal position
Right middle lobe Atelectasis:
In the middle area of the right lung there is consolidation, is it collapse ? We did lateral view and we can see that the transverse and oblique fissures moved from their normal position which indicates right middle lobe atelectasis
Left Upper lobe Atelectasis:
Left Lower Lobe COLLAPSE:
Pic1 : there is area of consolidation on the left lung, we will do lateral view… Pic 2 : lateral view of the lung shows a clear cutline which is the oblique fissure moved from its normal position (normal oblique line crosses the lung hilum)
Pic 1 Pic 2
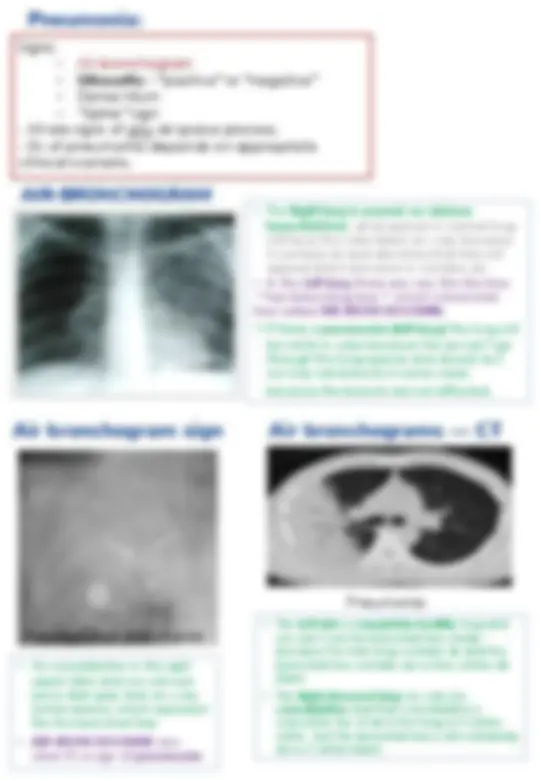
The lungs are filled of air and also the bronchi , we can’t see brachial tree because it’s also filled with air as the lungs, so both appear in black color while vessels appears in white because it filled with blood.
In case of pneumonia it appears as consolidation of lungs. The air is replaced by fluid or inflammatory cells. However. Bronchial tree remains as it is patent so we will be able to see bronchial tree on background of consolidation
PLEURAL EFFUSION:
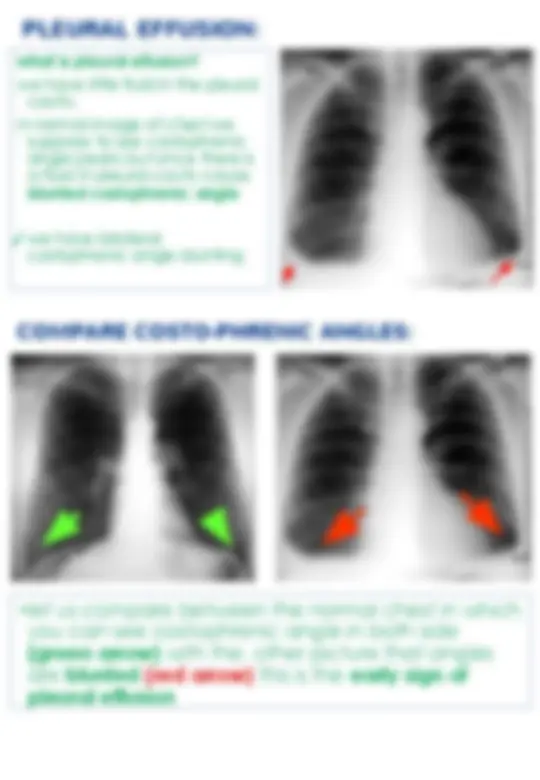
what is pleural effusion?
we have little fluid in the pleural
cavity.
in normal image of chest we
suppose to see costophrenic
angle peaks but once there is
a fluid in pleural cavity cause
blunted costophrenic angle
✓ we have bilateral
costophrenic angle blunting
COMPARE COSTO-PHRENIC ANGLES:
- let us compare between the normal chest in which you can see costophrenic angle in both side (green arrow) with the other picture that angles are blunted (red arrow) this is the early sign of pleural effusion
- On an upright film, an effusion will cause blunting on the lateral and if large enough, the posterior costophrenic sulci.
- Sometimes a depression of the involved diaphragm will occur.
- A large effusion can lead to a mediastinal shift away from the effusion and opacity the hemithorax.
- Approximately 200 ml of fluid are needed to detect an effusion in the frontal film vs. approximately 75ml for the lateral.
- Larger effusions, especially if unilateral, are more likely to be caused by malignancy than smaller ones.
PLEURAL EFFUSION
Moderate^ mild
- once fluid increase it goes up in curve line level , it is not like a cup of water with flat line level, costophrenic angle blunted once amount of fluid increase
- The doctor mentioned an experience in school we used to do it, we bring cup of water half empty when we see it from outside we see fluid level in flat line. if we cover and sucked air inside it it goes up in curve line.
- because there is no air , no pressure so it will be curved.
- naturally it has a low pressure because once fluid inside it, it will be sucked out
- always fluid in costophrenic angle given curve line however this is mild or moderate pleural effusion
- if we have mild pleural effusion we will get curve like in right picture, if we have Moderate pleural effusion we will get picture like in the left
- Right side lung with vessels
- On the Left side Jet black air , takes all left hemithorax we don’t have any lung here you can see the difference between Rt side and Lt sidre.d LT
Continue.. PNEUMOTHORAX
Hydro-pneumo-thorax:
- When will have air fluid level appears flat as this image?
- In Hydro-pneumo-thorax
- remember the example of covered cup filled with fluid.
- we have three things in right side: air – fluid level , above it jet black air so we have fluid, air and the lung.
A
Fluid Fluid
EMPHYSEMA:
- Increased Lung Volume
- Flattened Diaphragms
- Increase in Retrosternal Airspace
- Barrel chest
- Small Vessels
- Small, narrow cardiac shadow.
Emphysema is loss of elastic recoil of the lung with destruction of pulmonary capillary bed and alveolar septa. It is caused most often by cigarette smoking and less commonly by alpha- antitrypsin deficiency.
•Patient with emphysema take deep inspiration and can’t expire it out this will cause distention of the lung all the time will be full with air. •Ability to take short inspiration and expiration. •Cyanosed and has problem in inspiration and most of the times will be in ER.
LUNG (^) AIR
EMPHYSEMA Normal
- patient with emphysema have lost elastic recoil of lungs
- lung is rigid, so if the patient take deep inspiration will have problem in exhalation of that air as a result distention of lung.
normally if we take deep breath there will be normal recoiling and emptying the air without exertion.
emphysema : diaphragmatic cupola flatten ,heart decreased in size retrosternal air increases.
normally diaphragmatic cupola curved , heart broad , retrosternal air small and in lateral view diaphragmatic cupola not flatten
1-shortness of breath
2- cyanosis
3- diaphragmatic cupola will not raise as a result of increased lung volume flattening diaphragmatic cupola increased
4- increase retrosternal air in lateral view
5- barrel chest
6- attenuated vessels
7- hilar shadow “ heart “ smaller in size due to the air compression from each side.
- Emphysema is commonly seen on CXR as diffuse
hyperinflation with flattening of diaphragms, increased
retrosternal space, bullae (lucent, air-containing spaces that
have no vessels that are not perfused).
BLUNTED C/P ANGLE
BOTH SIDES
PNEUMOTHORA
X
AIR IN PLEURAL CAVITY
PNEUMOMEDIASTINU M
EMPHYSEMA
- Emphysema is commonly seen on CXR as diffuse hyperinflation with flattening of diaphragms, increased retrosternal space, bullae (lucent, air-containing spaces that have no vessels that are not perfused) and enlargement of PA/RV (secondary to chronic hypoxia) an entity also known as cor pulmonale. Hyperinflation and bullae are the best radiographic predictors of emphysema.
CT anatomy
CT
Air bronchograms — CT
Bronchus
vessel
Healthy
Pneumonia lung
Anterior Mediastinal Mass
- Anterior mediastinal masses consist of the 4 "T's" (Terrible lymphadenopathy, Thymic tumors, Teratoma, Thyroid mass) and aortic aneurysm, pericardial cyst, epicardial fat pad. Usually CT or fine needle aspiration is needed to make the definitive diagnosis of an anterior mediastinal mass.