



Monitoring, Evaluation, and Reporting
Indicator Reference Guide
MER 2.0 (Version 2.4)
September 2019




















































































Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
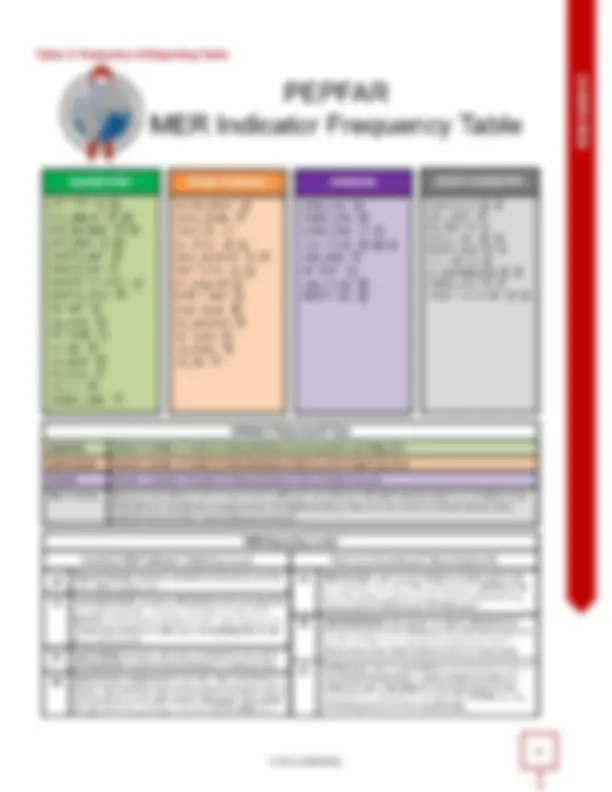
Figure 4: Indicator reporting frequency and the PEPFAR fiscal year. Based on programmatic gaps in case finding, linkages, index testing ...
Typology: Lecture notes
1 / 251

This page cannot be seen from the preview
Don't miss anything!
2
OVERVIEW
PEPFAR United States President’s Emergency Plan for AIDS Relief PHIA Public Health Impact Assessment PITC provider-initiated testing and counseling PLHIV people living with HIV PMTCT prevention of mother-to-child transmission POART PEPFAR Oversight and Accountability Response Team POCT point-of-care testing PP priority populations PrEP pre-exposure prophylaxis PT proficiency testing PVLS patient viral load suppression PWID people who inject drugs SID sustainability index SI strategic informaiton SIMS site improvement through monitoring systems STI sexually transmitted infection TA-SDI technical assistance for service delivery improvement TB tuberculosis TG transgender people TX treatment UNAIDS Joint United Nations Programme on HIV/AIDS USG United States Government VL viral load VLS viral load suppression VMMC voluntary medical male circumcision WHO World Health Organization OVERVIEW 7
Acknowledgments MER Indicator Refresh Headquarters Team: Kristine Clark (S/GAC), Heather Iufer (DOD), Catherine Nichols (USAID), Kimi Sato (Peace Corps), Nadia Solehdin (CDC), Pooja Vinayak (S/GAC) MER Indicator Refresh Field Committee: Sisay Abayneh (CDC: Ethiopia), Patrick Amanzi (USAID: Zambia), Mavis Boateng (USAID: South Africa), Trust Chiguvare (CDC: Zimbabwe), Bill Elur (CDC: Uganda), Rachel Kwezi (USAID: Uganda), Mutsa Mhangara (USAID: Zimbabwe), Anthony Muganza (Peace Corps: Namibia), Ghislain Mumbari (DOD: Cameroon), Mduduzi Ndlovu (CDC: South Africa), Joseph Nondi (DOD: Tanzania), Ifeanyi Okoye (DOD: Nigeria), Kim Perez (USAID: South Africa), Marisa Sanguankwamdee (USAID: Thailand), Leigh Tally (CDC: Zambia) Indicator Leads and Training Content Development Team: Shabeen Ally, Jenny Albertini, Teeb Al-Samarrai, Gretchen Bachman, Joseph Sean Cavanaugh, Kristine Clark, Caroline Cooney, Meaghan Douglas, Erin Eckstein, Heather Iufer, Lenny Kosicki, Catherine Nichols, Erin Rottinghaus, Kimi Sato, Nadia Solehdin, Heather Watts, Vamsi Vasireddy, Pooja Vinayak, Sherry Yin Headquarters Subject Matter Experts: Thank you to the many SMEs that contributed their time and expertise into developing and refining the MER indicators. 8
PERSON-CENTERED MONITORING The MER strives to drive program monitoring to a more patient-centered approach. Per the 2017 WHO Consolidated Guidelines on Person-Centered HIV Patient Monitoring and Case Surveillance, person-centered monitoring refers to a shift from monitoring measuring services (e.g., the number of HIV tests or people on treatment) to monitoring people at the center of their access to linked HIV and health services. In National Environment Local Environment PEPFAR Systems HIV Prevention and Treatment Services System Person Figure 2: Patient-Centered Monitoring in PEPFAR essence, this marks a shift to better support the clients accessing services by focusing more on their individual health outcomes. PEPFAR’s commitment to person-centered monitoring is evidenced throughout this guidance document through: Indicators (i.e., HTS_RECENT) that allow programs to better understand clusters of recently-infected patients and spur programmatic action in order to intervene to stop active infections (i.e., through interventions such as index testing services and test & start). Outcome-focused cascade analyses (e.g., index testing, prevention). Further modernizations to treatment indicators to continue to understand ART patient outcomes and retention in the era of differentiated care (i.e., TX_ML, TX_RTT). A continued commitment to ensure data disaggregation by standard five-year age bands in order to further enhance programmatic focus on strengthening patient-level monitoring systems. Ensuring COP-funding for health information systems projects is impactful and supports: (1) interoperability between systems; (2) the adoption of standardized disaggregations; (3) shifts away from paper-based to electronic reporting; and (4) the adoption or expansion of HIV surveillance systems for public health response. Person-centered monitoring and care is best practice in serving both the needs of the patient and the goals of reaching epidemic control program more broadly. To reach epidemic control, all people living with HIV (PLHIV) must be identified, linked immediately to treatment, and retained on treatment with viral suppression. If PLHIV are not retained in care, they are at risk of continued transmission and costly interventions are needed to track them. Interruptions in antiretroviral treatment can cause viral load to rebound in as little as one to two weeks in HIV+ patients that were previously suppressed on ART therapy. The longer a patient remains off treatment, the greater the likelihood that their viral load will rebound to a point of no longer being undetectable. Because undetectable viral load means that patients cannot onward transmit HIV (U=U), it is important to get patients back on treatment not only for their own health, but for the health of others in the community. Expeditious action in defaulter tracing to bring clients back to treatment well before their viral load has the opportunity to rebound is a key example of how patient centered monitoring ensures the best outcome for both the patient and towards our shared goal of epidemic control. However, some countries are struggling to maintain gains towards epidemic control because of the inability to retain patients. Providing services in a manner that keeps people on life-long ART is fundamentally the way HIV services should be planned for and delivered. Figure 3 below is an illustrative example of client loss in one PEPFAR program from FY 2018 Q4 to FY 2019 Q3. While the program reports an annual TX_NEW result of 101,189 and an annual TX_CURR result of 1,110,051, there is only a reported net new on treatment of 25,951. This means that roughly 75,238 patients from the total treatment cohort did not remain on treatment due to retention issues, data quality issues, etc. Furthermore, 25,071 patients tested positive for HIV and were not linked to treatment. Even with the understanding that this analysis is based on aggregate data, these numbers symbolize programmatic failures in linkage and retention that require immediate programmatic action. 10
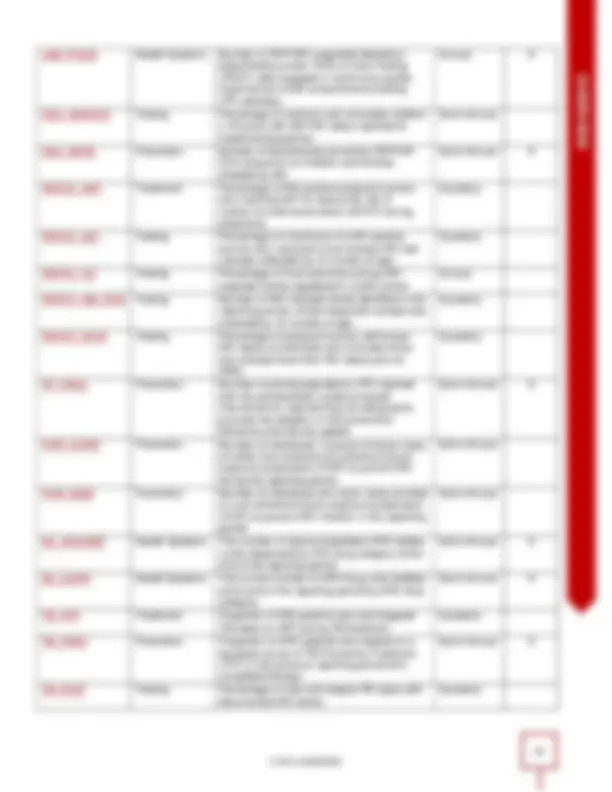
Figure 3: Potential treatment client loss in one PEPFAR program from 2018- 2019 MER REPORTING REQUIREMENTS Quarterly program results document site-level achievements realized in each quarter of the U.S. government fiscal year (October 1 – September 30). MER data is due on a standard cycle approximately 45 days after each reporting period ends. Refer to the PEPFAR Data Calendar for key deadlines and data cleaning dates. PEPFAR MER indicators vary in periodicity of reporting. Different indicators reflect different time periods for services being provided. Quarterly indicators are those indicators focused primarily on the clinical cascade: HIV case finding, diagnosis, linkage, treatment, retention, and viral load suppression. Semi-annual indicators are those focused primarily on HIV prevention and supply chain monitoring. Annual indicators are those focused primarily on health systems and host country reporting. OVERVIEW 11
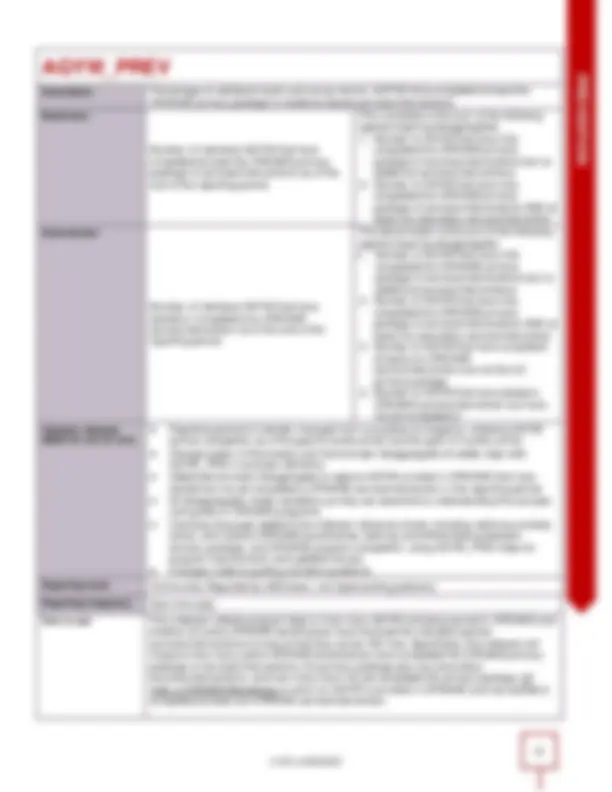
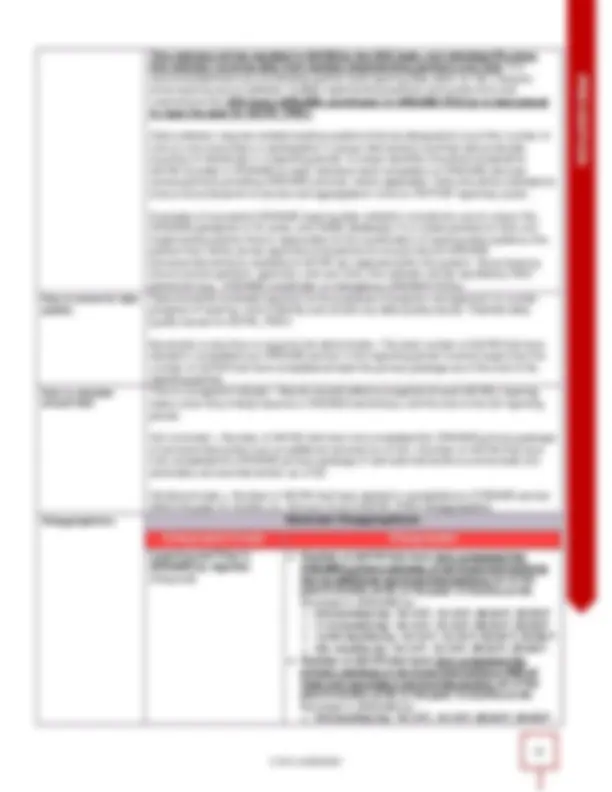
to note that an individual’s inclusion in some key populations is subject to change over time (e.g., an individual may engage in sex work or inject drugs for specific periods in their life) and should be assessed at each clinical encounter to ensure accurate reporting of these disaggregations on indicators such as TX_CURR. The PEPFAR key populations reporting guidance is designed to avoid double-counting and ensure that the KP data reported can be meaningfully interpreted. Despite persons potentially falling into more than one KP disaggregate (e.g., an FSW who injects drugs, MSM that is currently incarcerated), implementing partners should be instructed to report an individual in only one KP category with which s/he is most identified. This guidance applies to all key populations-associated indicators. Refer to the key populations classification document found in Appendix A for additional information on how to assess the needs of key populations client. Priority Populations: PP_PREV includes a series of optional priority population types for reporting. Please note that although reporting of the priority populations disaggregation is optional – it is highly recommended. Types of PEPFAR Support: To understand the level of support and the type of investments being provided, data are disaggregated by either direct service delivery (DSD) or technical assistance for service delivery improvement (TA-SDI). More information on these categories is provided in the section below. DISAGGREGATION TYPES: There are three categories of MER indicator disaggregations, which can be seen in the indicator reference sheets and the DATIM data entry screens. Required Disaggregations: Required indicates that this indicator disaggregate is required for all countries that have programming for this area. This means that if the country supports a program area, defined by budget and targets set during the COP process, then it is required to report results. Conditional Disaggregations: Conditional disaggregates include those for which some additional condition must be fulfilled. There are two main types of conditional indicator disaggregations: a. Disaggregations for those programs that have received initiative-specific funds for special programming such as DREAMS. There is also one full indicator, AGYW_PREV, that is conditional and based on DREAMS funding. b. Disaggregations for which field teams have received permission or a waiver from their PEPFAR Program Manager to report on, such as reporting on the coarse age disaggregations instead of the finer age disaggregations. In this case reporting is considered conditional based on written approval from OGAC. Optional Disaggregations: Optional disaggregates should be completed by those for which the indicator is useful to determine the success of their program (e.g., priority population disaggregations in PP_PREV). PEPFAR SUPPORT TO COMMUNITIES AND SITES Completing the fourth full year of quarterly site-level monitoring by all PEPFAR implementing agencies and partners has provided granular data that demonstrate important differences in patient outcomes and site performance. These results should be used to prioritize resources, staff, and interventions among sites to determine the appropriate extent of support and monitoring needed based on site-level outputs and quality outcomes. There are three categories of PEPFAR support that correspond to attained, scale-up, sustained and centrally supported areas. In areas where PEPFAR is supporting attained, scale-up, and sustained services the type of support should be categorized as Direct Service Delivery (DSD) or Technical Assistance-Service Delivery Improvement (TA-SDI). In areas where PEPFAR is not providing support at the site level but is providing financial support at the national or subnational levels, then this support should be characterized as Central Support (CS). DSD and TA-SDI include all sites receiving one or more PEPFAR-supported visits during the year. Importantly, site-level quarterly results and SIMS data should be analyzed and used to determine the number of program support visits needed each year to optimize the quality of HIV/AIDS services and impact. PEPFAR teams should work with implementing partners to ensure that programmatic data (including MER and SIMS results) are being used in this way. The key is to ensure that PEPFAR-supported sites receive the appropriate number of technical OVERVIEW 13
assistance visits based on their performance. Refer to the “PEPFAR-support definition” section within each indicator reference sheet for indicator-specific DSD and TA-SDI descriptions. DSD: Individuals will be counted as receiving direct service delivery support from PEPFAR when BOTH of the conditions below are met: Provision of key staff or commodities AND support to improve the quality of services through site visits as often as deemed necessary by the partner and country team. TA-SDI: Individuals will be counted as supported through TA-SDI when the point of service delivery receives support from PEPFAR that meets the second criterion ONLY: support to improve the quality of services through site visits as often as deemed necessary by the partner and country team.
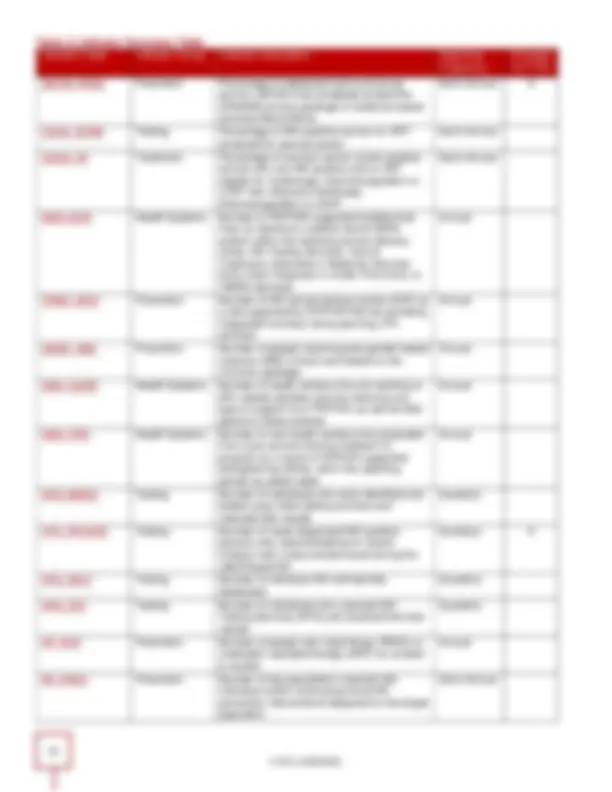
HOST COUNTRY TARGETS Targets for the host country national and subnational indicators should be reported into DATIM during COP. Developing targets for the next year at the national and subnational levels is an important step in understanding the national program and determining geographic investments (including host country, The Global Fund and other donors). When PEPFAR better understands the target setting process of the national program, then it is better placed to support the program and to fill necessary impactful programmatic gaps. Please describe the target setting process that the host country employs in the narratives and partnering donors). The national targets should cover the next calendar or fiscal year; the timeframe should be indicated in the narratives. HOST COUNTRY RESULTS At Q4 of the USG fiscal year, results from the host country systems should be reported up until the most recent month of collection and include 12 months of data. These may not align with the USG fiscal year end results. These data should be collected continuously at the subnational level. Data should be in line with GARPR and UNAIDS reported data, where available, although they may differ due to different reporting periods. In the narratives, please indicate what months the data include (e.g., October 2018 - September 201 9 ; or July 201 8 to June 201 9 ). Results should be consistently reported on the same time period to be able to monitor trends over time. Table 2: Host Country indicators by reporting level, targets, and results Host Country indicators by reporting level, targets, and results Host Country Indicator Reporting Level Results vs. Targets Requirements Indicator Name National Subnational Facility Targets Results DIAGNOSED X X X HTS_TST X TX_NEW X TX_CURR X X X X X TB_PREV X VL_SUPPRESSION X X X X PMTCT_STAT X X X X X PMTCT_ART X X X X X VMMC_CIRC X X X X VMMC_TOTALCIRC X X X X HRH_STAFF X X KP_MAT X^ X^ X Red X: Designates those indicators collected through the annual MOH data alignment process REPORTING MER RESULTS IN DATIM MER program results are reported in DATIM (Data for Accountability, Transparency, and Impact). Data are reported into DATIM by both implementing partners (IP) and USG staff in country depending on the type of indicator. Please refer to the indicator-specific requirements in the MER for more details. If you are an implementing partner or USG agency or HQ staff member that needs to access DATIM, visit the following link to request an account: https://register.datim.org/. Results in DATIM are entered at the facility and community-levels in DATIM and aggregate up to the district, regional and national levels as shown in the data flow diagram below. 16
Figure 5. MER data flow from the site to country level ROUTINE DATA CLEANING & COMPLETENESS CHECKS PEPFAR programs are expected to have reviewed, cleaned, analyzed, and interpreted their program results data prior to submission of their results to headquarters. Country teams are expected to conduct routine data cleaning and completeness checks using the Data Review Tool before submitting results in DATIM. There are several levels for data quality checks to be initiated by the responsible person at the site, implementing partner, PEPFAR country agency and interagency, and the headquarters levels. The data quality checks and review include both completeness and logic checks. Completeness checks begin at the site level with routine review of patient level data at the source of collection such as registers, EMRs or patient charts. These patient monitoring tools should be reviewed for entry completeness at each reporting period. Once implementing partner staff have completed data entry for the reporting period, the IP should confirm the overall completeness of data by reviewing a set of DATIM “Favorites” that display MER indicators’ “numerator” value and “denominator” values by disaggregation totals (e.g., total by age/sex, total by service delivery point/test result, total by age/sex/service type, etc.). An overview of DATIM completeness favorites and instructions on how to use them can be found below. When USG agency staff “Accept” MER results data from IPs within DATIM, these same DATIM Favorites should be reviewed to verify data completeness; if any issues are identified, these should be flagged by the AOR/COR, Activity Manager, or SI point of contact and returned to the IP for corrections or revisions. A set of data validation and logic checks should also be carried out between indicators before data is submitted to Interagency. DATA ENTRY AND REVIEW PROCESS OVERVIEW The in-country review of data completeness is a shared responsibility across all stakeholders, including data entry and review by implementing partners, review by agency, and further review and de-duplication data at the Interagency level. OVERVIEW 17
USG Interagency staff should review all submitted data using the DATIM Data Completeness Favorites prior to submission to headquarters; with three levels of accountability (IP, agency, interagency), it is expected that data completeness challenges should be identified, addressed, and/or explained as part of the USG technical area indicator narratives. If any data inconsistencies are identified and have not already been documented in the narrative, data must be sent back down to the agency and then to the IP level for the inconsistency to be either reconciled or, if irreconcilable, documented in the narrative. DATA REVIEW COMPLETENESS TOOLS MER Data Cleaning and Completeness Review Favorites (or “Favorites”) are saved data query outputs generated from live data within DATIM as submitted by implementing partners. S/GAC has created and shared a list of standard “favorites” globally to help DATIM users validate data for completeness and consistency of entry across their program. These reports emulate the MER data entry screens and allow all DATIM users to review the totals of MER indicators. If the totals are not equal to the users’ expected result, users can look at the disaggregated data to see where a data error is present. These favorites are tagged to the “MER Result & Target Review Favorites” dashboard that is accessible to all DATIM users on the main landing page when a user logs into the system as seen in the screenshot below. Figure 7. MER result and target review favorites in DATIM In addition to their availability on the dashboard, the data cleaning favorites can also be found in DATIM’s pivot table app. Each canned cleaning favorite uses the following naming convention: Figure 8. Naming convention for MER result and target review favorites in DATIM OVERVIEW If an indicator is calculated by auto-summing other indicators and/or disaggregates, AUTO-SUM” will be present in the favorite’s name (as seen underlined in the example for HTS_SELF found below). Also, for testing 19
indicators, “Facility” or “Community” will appear after the fiscal year and reporting section of the favorite name to easily discern testing modalities. For example, the DATIM favorite to review the results for the distribution of HIV self-test kits (i.e., HTS_SELF) by age, sex, and test kit distribution method is named: PEPFAR FY19Q1 Results HTS_SELF N AUTO-SUM Age/Sex/HIVSelfTest Directly Assisted/Unassisted Completeness Review Pivot AUTO-POPULATION OF HTS_TST MODALITIES: The definitions for the PMTCT (ANC1), TB, VMMC, and index HIV testing services modalities have been aligned with their respective parent status indicators (i.e., PMTCT_STAT, TB_STAT, VMMC_CIRC, and HTS_INDEX). Results are no longer entered for these modalities through the HTS_TST indicator directly but are instead entered into the parent indicator and then auto-populated into HTS_TST in an effort to reduce data entry redundancy and reinforce the relationships between indicators. For example, results entered for TB_STAT newly tested positives will auto-populate into the TB modality for HTS_TST within DATIM. DATIM users will still see these modalities on the data entry screen but will no longer be able to enter data directly into the modalities. Once data is entered for the parent indicator, it will be copied into the relevant data entry form for the corresponding HTS modality. For further details, see the diagram below and review the HTS_TST reference sheet. Figure 9: Auto-Population of HTS_TST from Associated Indicators 20