Download N5315 Advanced Pathophysiology and more Study Guides, Projects, Research Nursing in PDF only on Docsity!
N5315 Advanced Pathophysiology
Inflammation, Altered Immunity and
Infection
Core Concepts Objectives with Advanced Organizers
IMMUNE SYSTEM: FIVE TYPES
The first four types are all ADAPTIVE
- **Cell-Mediated immunity
- Humoral immunity
- Acquired immunity** (you may see it written as Active Acquired immunity ) - Passive Acquired immunity {both natural & artificial} = (borrowed immunity)
- Natural immunity (innate response/ genetic immunity, not from previous
exposure, includes the Inflammation process and NK cells)
- NK-cell=Natural killer cells= part of the Innate/Natural immune system, in lecture and outline They come from the lymphoid stem cell line, like regular T & B cells and are considered a T-cell type, but don’t differentiate further to become specific for any one antigen. They kill via cell lysis or apoptosis without the need for specific antigen receptors (more info later in notes)
- Killer T-cells = Cytotoxic-cells, Tc (Cytotoxic-cells is what Dr. G labeled them on the organizer) These are in lecture and Organizer also. NOTE TO SELF ** NKT-cells =hybrid of the other two (not in lecture or outline) WHO CARES, don’t get confused
Natural/Innate immunity (from book table 7-1 page 192) SKIP Not part of Dr. G outline or objectives
The first line of Defenses
- Occurs constantly (through our natural physical barriers like skin)
- Book calls it Broadly specific aka, not specific!
- No memory
- Uses Epithelia cells (like skin) Peptides involved:
- Defensins,
- cathelicidins,
- colectins,
- lactoferrin,
- bacterial toxins Protective factors include:
- Cytokines, lysosomes
- Low stomach PH
- Low Urine Ph
- Ciliary activity
- Skin, mucous membranes Second line: Inflammation :* Immediate*
- Broadly specific “Aka is Broadly activated by most anything, Damage to cell or any foreign antigen”
- No memory Cell type used:
- Granulocytes = ( neutrophils/basophils/eosinophils, mast-cells) (all contain granules inside)
- Monocytes/Macrophages (changes to Macrophages in tissue)
- NK cells =Natural killers (also function as antigen presenting cells) stimulating=the T-B cell action
- Platelets
- Endothelial cells Peptides involved
- Complement
- Clotting factors
- kinins Protective factors include:
- Vascular response, vasodilation
- Cellular components (the cell types listed above)
- Secretory molecules or Cytokines (can be either pro-inflammatory, or anti-inflammatory)
- Activation of plasma protein systems
ADAPTIVE (AQUIRED) Immunity passive &active ( Humoral and cell mediated ) Everything else
Third Line defenses
- Is initiated by the cells of the innate immune system NK=natural killers
- Delay between primary exposure to antigen and maximum response
- Immediate reaction on second exposure to antigen
- Very SPECIFIC
- Memory of antigens from T and B (lymphocytes memory cells) Cells type used:
- T Lymphocytes from Cell mediated Immune system
- B lymphocytes from Humoral Immune system
- Macrophages/ Monocytes
- Dendritic cells Peptides involved
- Antibodies
- Complement Protective factors
- Activated T and B lymphocytes
- Cytokines AND Antibodies
EXAMPLE OF HOW CELL MEDIATED IMMUNITY WORKS.
Antigen enters host cell → Macrophage
- → antigen expressed on MCH (major histocompatibility complex) class II
- → secretes Interleukin 1 to attract T- helper cells/CD
- → presents it to T-helper cell/CD4 cell
- → T-helper/CD4 differentiates into Th1 & Th2 (these are sub groups of T-helper cells)
- → Th1 (subgroup T-helper cells/CD4 cell) releases Interleukin 2 (IL 2)
- → IL 2 activates CYTOTOXIC T-cells: (Tc), CD8, killer T’s, T8 Cells, all the same thing )
- → Tc (Cytotoxic T-cells, CD8) connects with MHC class I receptor on invader
- → Cytotoxic chemicals released → invader killed.
- Th2 (subgroup of T-helper-cell /CD4-cell) releases Interleukin 4 (L4) → activates
the Humoral immune system: AKA call the B-CELLS IN to do their job
Same Idea presented differently
T cell activation: begins with the binding of antigen to specific T cell receptors. The naïve T cell proliferates and differentiates into a functional (effector) T cell, whose functions include: (1) direct killing of foreign and/or abnormal cells, (2) assistance and/or activation of other cells, such as macrophages. The first function is carried out by a subclass of T cells, termed T cytotoxic lymphocytes. Activation of macrophages is performed by a special subset of Th cells. Additional T cells develop into T-regulator cells that regulate the immune response in order to avoid inadvertently attacking self-antigens or to avoid over activation of the immune response
EXAMPLE OF: ACTIVATION OF HUMORAL IMMUNITY / B-CELL immunity /
G.E.M.A.D antibodies creation
- B-cells stimulated by release of IL
- B-cells differentiate into plasma cells that produce Antibodies and memory B-cells.
- Plasma cells produce antibodies ( IgG.IgE.IgM.IgA.IgD) that will bind to the antigen
and form: antigen-antibody complexes
- Memory B-cells will act during secondary immune response and will remember the
antigen and respond quicker in initiating the immunoglobulin (Ig- G.E.M.A.D) creating
process.
- Present antigen antibody complex to the cell mediated immune system
Same Idea presented differently
B cell activation occurs when an immune-competent B cell encounters an antigen for the first time, only those cells with specific BCRs complimentary to that antigens determinant sites are stimulated to proliferate & differentiate (clonal selection), resulting in multiple copies of that particular B-cell. The differentiated B-cell becomes a plasma cell & can be found in the blood, secondary lymphoid organs (sleep & lymph nodes), & some inflammatory sites. Each plasma cell is a factory for antibody production & is dedicated to the secretion of a single class or subclass of antibody with one variable region & therefore specificity against one antigenic determinant.
DIFFERENCE BETWEEN CELL MEDIATED & HUMORAL IMMUNITY
B-Cells come from Lymphoid Stem Cells: that mature in the bone marrow and are initially given
receptors for all possible antigens (Clonal Diversity), then B-cells travel to secondary Lymph
organs where they wait for Clonal selection activated by antigen presence. They are ready to
provide Humoral immunity when needed, by further differentiating into Plasma cells that can
produce antibodies for a specific antigen. Each B-cell is specific to one antigen.
Humoral Immunity is that immunity conferred by the B-Cells. It provides immunity against
- some viral infections,
- toxin induced diseases - diseases caused by : pneumoccoci, meningoccoci, or Haemophilus. Page 1, lecture notes
Humoral Immune Response Is governed by B-Cells.
B-cells (mature in bone marrow) not specific yet, after (2nd^ phase of maturation) They become
Plasma B-cells that then produce Antibodies for specific antigens
There are 5 classes of antibodies (glycoproteins): ( G.E.M.A.D) from lecture notes only
- IgG - is the most prominent immune globulin. - It binds with viruses, bacteria and toxins. - It activates complement and binds to macrophages. - It is the primary antibody in the secondary immune response. - Levels rise in response to subsequent exposure to an antigen. **- It is the only immune globulin that crosses the placenta.
- IgE**
- binds to mast cells, eosinophils and basophils.
- Involved in parasitic infections
- Involved in hypersensitivities reactions. (TB skin tests)
- Least concentrated, least controlled - IgM
- Is the largest of the immunoglobulins
- is the main immune globulin produced early in the primary immune response. (first time antigen is present in a cell) - A high level of IgM antibodies indicates a recent infection.
- Synthesized in neonatal life, and may increase as response to infection in Utero IgA - is the main immune globulin in secretions and mucous membranes
- It prevents the attachment of microorganisms to the mucous membranes.
- Secretions prevent dehydration
- IgD
- is found on the surface of B-lymphocytes. Its function is not understood.
Active Acquired Immunity: adaptive 3 rd^ line defense. State of immunity that is
- acquired after exposure to an antigen.
- improves with repeat exposure
- it is specific.
- Slower
- Long lived
- basis of vaccinations. (encourage Vaccination) Passive acquired immunity : (TWO TYPES ) is that immunity acquired via the transfer
of antibodies , or T-cells to the recipient.
- Natural (Passive acquired Immunity) occurs via mother to fetus. Antibodies cross
the placenta or in the breast milk. (encourage breast feeding)
- Artificial ( Passive acquired Immunity) occurs when Antibodies are given to a recipient to
provide immunity. This is used to treat rabies, tetanus, hepatitis, snake bites. It is a
good way to fight infection, has immediate protection but the immunity only lasts as
long as the Antibodies, approximately 2 weeks.
Natural Immunity (AKA Innate Resistance Immunity/ genetic immunity).
This is resistance that exists prior to exposure to a microbe. We are born with this resistance and
is based on our genotypes and species. For example, humans cannot become
infected with canine distemper. Dogs/cats can’t be infected with West Nile virus.
Natural immunity is provided by nonspecific barriers to infection such as the skin,
mucous membranes and by certain cells like:
- Natural Killer cells NK serve the same function
as CD8 or T-cytotoxic cell except they are not cell mediated and don’t recognize
specific antigens, they don’t need antigen markers they attack any invader seen as
foreign , they can perforate the “skin” of invading antigens and release cytotoxic
chemicals, lysing the cell Or the can kill injured/cancerous cell via apoptosis.
- It also uses certain proteins like (complement, cytokines),
- involves inflammation and phagocytosis.
- It does NOT improve after exposure.
- It functions to kill invading microorganisms and ACTIVATES the Acquired
Immune systems both Active AND Passive ( both natural & artificial ).
TERMS TO KNOW
Antigen: Harmful molecule that can react with antibodies or antigen receptors on B and T cells
- Foreign, “non-self”
- Viruses, bacteria, fungi, parasites
- Can also be found on noninfectious environmental agents (pollens, food,
bee venom, drugs, vaccines, transfusions)
- To function: at least a portion of a molecule’s chemical structure must be
recognized by and bound to an antibody and/or to specific receptors on a
lymphocyte
APC=Antigen Presenting Cell : Cells that process an antigen and present them to the T-helper
cells of the cell mediate immune system or the B-plasma cells in the humoral system, it basically
any cell that can process the invader and put a marker on the outside of the cells surface to alert
the immune system to action. Examples are, from lecture notes
- B-lymphocytes (Humoral system)
- dendritic cells
- Macrophages (Inflammatory system)
Self-antigen - can induce immune response resulting in production of antibodies or functional T cells
that attack
- Most individuals tolerant of their own antigens
- Thought to be Regulated by T regulatory cells (T-reg)
Antibody: AKA immunoglobulins G.E.M.A.D
- (Y shaped protein produced by plasma B-cells)
- used by immune system to neutralize pathogens (bacteria/viruses)
- Recognize a unique molecule of harmful agent called antigen
- Neutralize bacterial toxins > coat bacteria to enhance phagocytosis > formation
of antibody complex > activates complement cascade
Aging and the Immune System
o T-cell Immune function decreases d/t changes in lymphocyte function
o Decreased T-cell activity d/t decrease thymus size
o Decreased B-cell function d/t decrease in antibody production in response to
antigenic challenge, increases in circulating immune complexes and in
circulating autoantibodies (antibodies against self-antigens)
o Shift in the balance of T-cell subsets is observed. These changes may result
in increased susceptibility to infection.
Fetal and Neonatal immune function
Stage of Development Immune Function Differences
Fetal antibody production deficient
- -Last trimester, fetus capable of
producing a primary immune
response (IgM only),
- but is unable to produce a
significant IgG response –
- Active transport facilitates the passage
of maternal antibodies into the fetal
circulation (d/t size of
immunoglobulin, unable to diffuse
across cellular layer)
Neonate At birth, total IgG levels in umbilical cord=
adult levels, but when cord severed, antibody
titers begin to drop
- The maternal antibodies are slowly
catabolized after birth until they
disappear altogether by about 10
months of age. The neonate begins
producing IgG at birth, & the child’s
antibodies reach protective levels
after about 6 months of age.
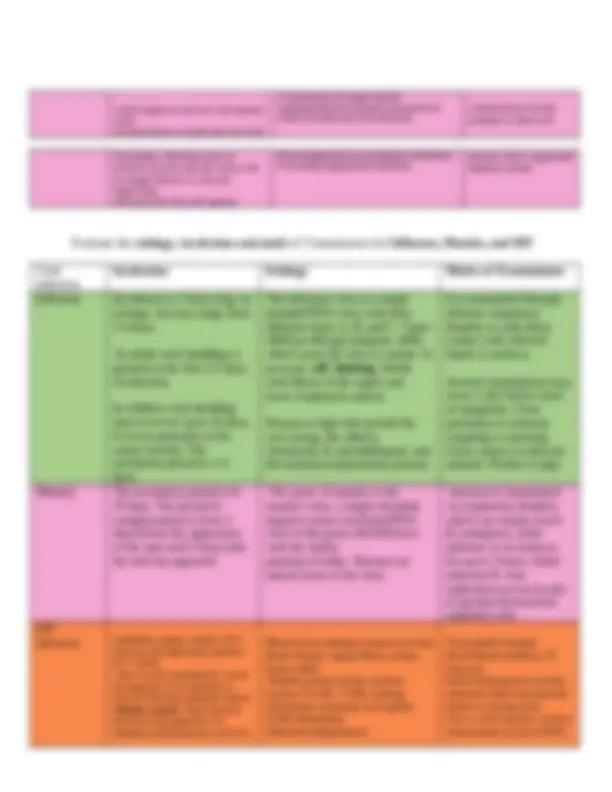
Inflammation ( AKA. Second line of defense )
Key Player Role and Function
Mast Cell “I simply want you to know that mast cell degranulation also
triggers the activation of the acute phase reactants”. (quote from
his lecture notes) Mast cell degranulation results in the release of
four main items: (these are acute phase reactants) histamine,
cytokines, leukotrienes, & prostaglandins ) Histamine is
responsible for causing vasodilation , it increases vascular
permeability , (* sound like sepsis ) it increases blood flow to the site
of injury which ultimately causes erythema and swelling at the site
of injury
Histamine 1 (PRO) Pro-inflammatory
-Present on smooth muscle- especially bronchi (causes muscle to contract=
Broncho restriction)
Histamine 2 (ANTI) Anti-inflammatory (suppresses leukocyte function)
-Found on parietal cells of stomach mucosa and induces secretion of
gastric acid as part of normal physiology of the stomach
Cytokines Cytokines can react quickly or may be more delayed. IL 4 is
released early in inflammation and IL13 is released later in the
inflammatory response.
Leukotrienes Leukotrienes are released when the mast cell degranulates. They are
also known as slow reaction substances of anaphylaxis (SRS-A) and
tend to prolong the inflammatory response. *important for later
stages of inflammation* They cause vasodilation, smooth muscle
contration, and attract neutrophils, monocytes and eosinophils. This
is the target of inhibition for the drug Singulair
Prostaglandins Prostaglandins are also released when the mast cell degranulates and
are produced by the arachidonic pathway. But ultimately, they
function to cause vasodilation, platelet aggregation at the site of
injury, pain and fever AKA reaction substances of anaphylaxis (SRS-A
Chemotactic Factors Attract neutrophils, eosinophils, and (Monocytes that turn into
Macrophages once inside injured tissue). All of these perform
phagocytosis.
Platelet Activating
Factor
-Derived from mast cell
-Produced by removal of a fatty acid from the plasma membrane &
produced during inflammation by neutrophils, monocytes, endothelial
cells, platelets
-Similar to leukotrienes (causes endothelial cell retraction to increase
vascular permeability, leukocyte adhesion to endothelial cells, platelet
activation)
Neutrophils Neutrophils will show up at the site of injury in 6-12 hours are
responsible for phagocytosis. * First responders*
ingest bacteria, dead cells, cellular debris
-Short lived (mature cell, cannot divide, sensitive to acidic environment) >
becomes component of purulent exudate/pus > removed from through
epithelium or lymphatic system
Analyze the steps of the arachidonic acid pathway and describe the implications for
treatment of inflammation.
The arachidonic pathway is the biochemical process which is responsible for the
synthesis of prostaglandins. It is a separate arm of the inflammatory process & has a significant
role in maintaining homeostasis. Arachidonic acid is made from linoleic acid which is part of
the phospholipid cell membrane. see algorithm page This is on OBJECTIVES for Module#
and appears Important. This is not a complete study guide, will need to look at it more in depth,
maybe draw it out.
The arachidonic pathway is the biochemical process which is responsible for the synthesis of prostaglandins. It is a separate arm of the inflammatory process and has a significant role in maintaining homeostasis. Arachidonic acid is made from linoleic acid which is part of the phospholipid cell membrane. The enzyme phospholipase A2 is responsible for the conversion of linoleic acid to arachidonic acid. Arachidonic acid is then converted by the COX 1 & COX2 enzymes to prostaglandin H2. Prostaglandin H2 undergoes further conversion to form prostaglandins, thromboxane A2, and prostacyclin. The prostaglandins formed by the COX pathway function to maintain homeostasis. They maintain the gastric mucosa, fluid and electrolyte balance, and platelet aggregation. The prostaglandins made from the COX2 pathway function mainly in the inflammatory process and produce pain and fever. However they too have a role in maintaining homeostasis (renal function, tissue repair, reproduction development). Because the prostaglandins made from the COX2 pathway function mainly in a pathologic manner drugs were developed to inhibit the action of COX2. COX2 inhibitors (NSAIDS) were developed to help preserve the gastric mucosa (prevent ulcers & bleeds) while at the same time inhibit the effects of inflammation. All of the COX2 inhibitors (except for one) have been removed from the market secondary to an increase in cardiac events which were associated with their use. Celebrex is the only COX2 inhibitor which is still available for use. A note of caution… while COX2 inhibitors block the inflammatory functions of prostaglandins, they can also impair renal function. There is a risk of renal impairment because those prostaglandins made from COX2 have a role in maintaining renal function. Non selective NSAIDS inhibit both COX1 and COX prostaglandin synthesis hence the risk of gastric ulcerations, GI bleeds, increased risk of bleeding and edema. These are common side effects of NSAIDS as is renal impairment. Aspirin blocks both COX1 and COX2 but its inhibition of these two enzymes result in the additional effect of inhibiting the formation of Thromboxane A2 and prostaglandins, unlike other NSAIDS. Corticosteroids inhibit the action of phospholipase A2 thus preventing the formation of prostaglandins, thromboxane A2, prostacyclin and leukotrienes. Please review the process of prostaglandin synthesis in the concept map below.
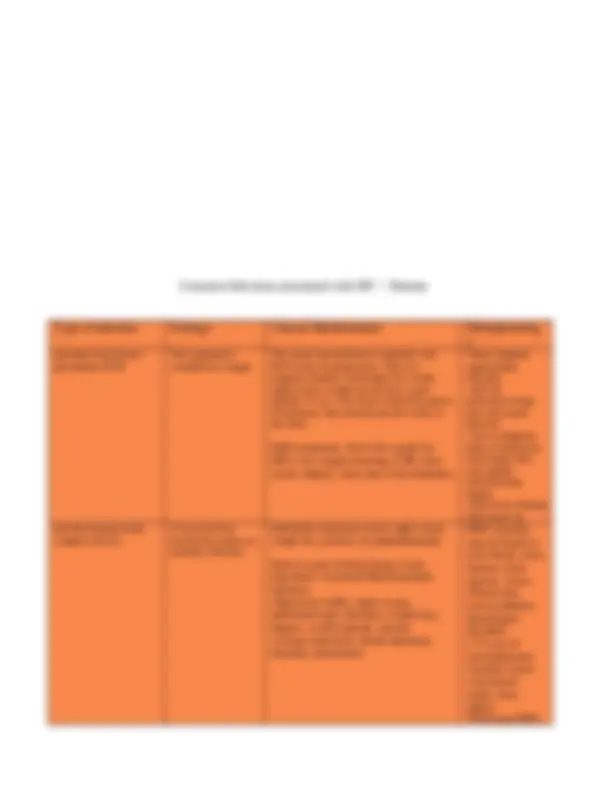
Disorders of the Immune System Autoimmunity- is a breakdown of tolerance in which the body’s immune system begins to recognize self-antigens as foreign. disturbance in the immunologic tolerance of self-antigens (immune system usually doesn’t recognize individual’s own antigens.) Reaction causes person’s own tissues to be damaged by autoantibodies (low quantity of antibodies against their own antigens) or autoreactive T-cells. AKA autoimmune disease Etiology Clinical Manifestations Pathophysiology Systemic Lupus Erythematosu s It is a chronic multisystem, inflammatory disease. It affects primarily women between the ages of 20-
- Diverse maternal autoantibodies induce anomalies (ie: congenital heart defects) in the fetus or cause pregnancy loss -Maternal alloantibody transported across placenta to fetal circulation -Disease process develops slowly, up to 10 years from occurrence of first antibody until diagnosis Clinical manifestations include a butterfly rash to cheeks, photosensitivity, nonerosive arthritis of There is no cure. The goals of treatment are to control symptoms and prevent further damage at least two peripheral joints, etc. -Large antibodies produced nucleic acids (*DNA, RNA), erythrocytes, coat proteins, phospholipids, lymphocytes, platelets-T DNA in circulation from cellular damage in response to trauma, drugs, infections that are usually removed by the liver
T for deposition in the kidneys -*NO CURE, tx symptoms -Nsaids (ASA, ibuprofen) to reduce inflammation, relieve pain -Protect from sun exposure -Immunosuppressive drugs (IVIg) Characterized by the large production of auto antibodies against DNA, erythrocytes, coagulation proteins, phospholipids, lymphocytes, platelets, & many other self-components. The most characteristic autoantibodies produced in SLE are against DNA, histones, ribonucleoproteins & other nuclear proteins. Complement participation -Neutrophils involved -IgG, IgM -Type II (tissue specific hypersensitivity) -Can cause inflammatory lesions -More often in women -Flares up from environmental agents (UV light, infections) -Difficult to diagnose (4/11 to be diagnosed on list) Rheumatoid Arthritis is a systemic autoimmune disease that causes chronic inflammation of connective tissues primarily in the joints. It affects 1-2% of adults & is more common in women. The incidence increases after age 30 Chronic inflammatory disorder that affects joints + wide variety of body systems (skin, eyes, lungs, heart & blood vessels) -Autoimmune disorder -Immune system mistakenly attacks your own body’s tissues This is a progressive disease & the damage is irreversible, leading to deformity & disability. Widespread, symmetrical joint swelling, erythemic joints which are warm to touch of function in the joints, morning stiffness that improves with movement, weight loss, & anorexia. There is no cure. The goals of treatment are to control symptoms and prevent further damage Affects lining of your joints -RA has acute onset with general systemic symptoms of inflammation -Local manifestations occur gradually over weeks/months -Causes painful swelling that can eventually lead to bone erosion and joint deformity, may lose mobility/ ROM -Stiffness lasts for ~1 hour in the morning, may be caused by synovitis- associated Inflammation is what can damage other parts of the body as well In the disorder IgM autoantibodies are formed against IgG antibodies & they bind together & form an antigen complex. These antigen antibody complexes are deposited in the synovial membranes. The membranes are then infiltrated with T cells, plasma cells, macrophages, & the inflammatory process is started. This causes tissue damage which results in the characteristic joint inflammation, pain & destruction of synovial membrane. During inflammation, argine (an amino acid) can be enzymatically modified into another amino acid (citrulline)= changes structure and function of protein and cause cell death -Promotes osteoclast formation, causing bony erosion
compounds thereby significantly limiting DNA and RNA synthesis. This medication can only be used to prevent rejection.
Corticosteroids
Prednisone and Methylprednisolone Corticosteroids prevent:
- RNA and DNA synthesis
- cytokine release
- IL-2 production
- IL-2’s activation of T-cells
- cytokine induced B cell stimulation
- the action of macrophages
- leukocyte chemotaxis
- complement release
- phospholipase A2 from producing prostaglandins *This group of medications inhibits multiple levels of the immune and inflammatory response. They can be used to treat rejection. *
Describe the role of the human leukocyte antigen (HLA) in solid organ rejection.
The histocompatibility genes are responsible for the coding of these proteins & are located on
chromosome 6. The location of the histocompatibility genes is known as the major
histocompatibility complex. HLA is the targeted response for transplant organ rejection. Tissue
typing occurs prior most transplants to identify the HLA of both the recipient and the donor to
match them as closely as possible to decrease the risk of rejection. Class I antigens are HLA-A,
HLA-B, HLA-C & are found in most human cells. They are primarily responsible for organ
rejection. Class II antigens are found on macrophages, dendritic cells, Langerhans cells, B cells
& T cells. Some diseases such as ankylosing spondylitis are associated with the presence of a
specific HLA antigen. Persons with HLA-B27 are at an increased risk of developing
ankylosing spondylitis. Human leukocyte antigen (HLA) : Immune response against antigens
on donated tissue. Type IV cell mediated reaction (rejection within 2 weeks w/o
immunosuppressive drugs
Matching HLA-DR locus appears to be most critical for graft acceptance
EXTRA INFO ABOUT ALLERGIC REACTION, MAY NOT NEED MOST OF IT
Hypersensitivity Etiology Clinical Manifestations Pathophysiology Type I (Hypersensitivity Response) It is an immediate hypersensitivity response to an environmental allergen. Most of the reactions are attributed to allergies to food, medication, pollen, etc. The reaction occurs in minutes to hours from the time of the exposure to the allergen. Environmental allergies: asthma, asthma exacerbation, food, drug, animal, & insect venom allergies. Angioedema: which may be idiopathic or related to medications, causing swelling of the lips, eyes & larynx. (Anaphylaxis). Atopic Disorders: type I reaction & include hay fever, asthma, eczema, & urticaria. They have strong genetic disposition. Pathogenesis begins with the antibody IgE. Upon initial exposure to the allergen IgE binds with the allergen. This primes the stage for a reaction to later occur. Upon re-exposure, the allergen (antigen) binds with the previously formed antigen-IgE complex. The mast cell detects the complex & begins to degranulates. It releases histamine & triggers the inflammatory cascade. Clinical manifestations are dependent on the route the allergen entered the body. Type II (Antibody mediated or Cytotoxic Hypersensitivity) It is a reaction which is mediated by antibodies directed against fixed antigens on the plasma membranes of the cells. This is an IgG & IgM antibody mediated reaction. Alloimmune reactions: to blood transfusions result from the wrong blood type being administered. ABO incompatibility is a good example.. ****Organ Transplant reactions***** Rh incompatibility: is another example of a type II reaction. A person who is Rh + has the Rh antigen. If they are negative, they do not have the antigen & are Rh-. Giving blood that is Rh- to a patient that is Rh+ will cause a transfusion reaction. Autoimmune Examples: Graves’ dz is a type of hyperthyroidism. In this disorder autoantibodies are formed against thyroid cells. They bind to thyroid cells & mimic the action of TSH. The pathogenesis begins with the binding of IgG & IgM to an antigen on a plasma membrane. This activates complement & it forms the membrane attack complex (MAC) which causes cell lysis. IgG & C3b may also bind to the antigen & the macrophages & trigger cell lysis through phagocytosis. Both IgG & complement attract neutrophils to the tissues. Neutrophils perform phagocytosis & release granules which cause tissue damage. NK cells also located in the area recognize the target cell antigen & release a toxic substance to destroy the target cell. Antibodies reacts with the target cell’s receptor, or inappropriately stimulates the receptor. Type III (Immune Complex Hypersensitivity) Antibodies are formed against & bind to circulating antigens. Examples include: Systemic Lupus Erythematosus & Rheumatoid Arthritis This forms an antigen-antibody complex. Once the complex is formed they are the deposited in vessel walls or extra vascular tissue & trigger an immune & inflammatory response. The immune & inflammatory response causes cellular & tissue damage. This is an IgG & IgM mediated response. It is similar to a type II reaction; however, it is not specific to a cell or tissue. The antigen antibody complexes are spread via circulation throughout the body & generate a more diffuse reaction. Type IV (Delayed Cell- Mediated Hypersensitivity) It is a reaction that is mediated by T cell lymphocytes & does not require antibody participation. It is a delayed reaction that occurs 24-72 hours’ post- exposure to an antigen. Contact Dermatitis: is a T cell mediated reaction to antigens such as poison ivy, topical drugs, chemicals such as nickel, or formaldehyde. A Reactive Tuberculin Skin Test: The PPD will cause a reaction only if the person was previously exposed to the tuberculin antigen. Solid Organ Transplant Rejection: A T cell mediated reaction that occurs 11- days after first exposure & 5-6 days after the second exposure. Contact Dermatitis: In this reaction antigens too small to cause the rash, red bumps, itching & blisters. A Reactive Tuberculin Skin Test: The T memory cells recognize the tuberculin antigen & initiate a local response & cause an induration in 24-72 hours. Solid Organ Transplant Rejection: This results in mononuclear infiltration, decreased circulation & tissue necrosis.
Organism (^) Structure Pathogenic Properties Bacteria Bacteria are unicellular, prokaryotic (no nucleus, humans are eukaryotic cells) organisms about the size of our mitochondria. They do not contain any organized intracellular organelles, but they do have a cytoplasm, ribosomes, lipid plasma membrane and outer rigid wall composed of peptidoglycan. Peptidoglycan is made up of sugar and peptides. It provides protection against osmotic pressure. It is produced only by bacteria and is the site of action for some antibiotics. Bacteria have a single chromosome of DNA coiled in the center of cytoplasm and RNA that functions to produce protein. Bacteria are found in multiple shapes. Cocci is a round/spherical shape which is common of Strep and Staph. Bacilli is a rod shape bacterium, such as E. Coli. Spirochetes are helical in shape such as Treponema Pallidum (syphilis). Then some bacteria are pleomorphic and have no particular shape and do not have a rigid cell wall such as Mycoplasma Pneumoniae. Bacteria may be arranged in a diplococci fashion which means they occur in pairs. Bacteria which forms chains of cocci is typically strep when they form clusters which look like grapes that is normally staph. Info from lecture
- Have a Capsule a polysaccharide that surrounds the bacteria and provides extra protection against phagocytosis
- Plasmids are extra chromosomal DNA molecules that multiply independent of DNA. It carries the genes for antibiotics resistance and toxin production
- Pili- hair like filaments that assist with attachment of the bacteria to cell surface such a N. gonorrhea
- Glycocalyx which is a slime layer secreted by bacteria, to assist with adherence to structures like the skin, heart valves, or catheters. Streptococcus Mutans which is located in the mouth, attaches to teeth via glycocalyx → formation of plaque and carries.
- Some bacteria are spore forming bacteria. This allows the bacteria to become dormant and impervious to host defenses. Clostridium species are known as spore forming bacteria. When the conditions are right they will become active again.
- Strep & staph part of normal skin flora and reside on healthy skin or nares- but can also initiate skin infections Virus Viruses are small pathogens (20-30 nanometers) with no organized cellular structures.
The stages of Replication are as follows:
First the virus binds to specific receptor on host’s cell
membrane. It then penetrates the cell membrane by fusion
with cell membrane receptor or directly crossing the
membrane. The Capsid is then shed so the genetic material is
fre
e
to
us
e
the
cel
ls’
or
ga
nel
les
to
rep
lic
ate
Th
e
pr
oc
ess
is