


Collection of Oropharyngeal
and Nasopharyngeal Swabs for
Respiratory Infections





Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
NPSOPS SPECIMEN COLLECTION PROCEDURE
Typology: Summaries
1 / 15

This page cannot be seen from the preview
Don't miss anything!
(^) The success of respiratory viral detection depends largely on the quality of the Oropharyngeal Swab and Nasopharyngeal Swab specimens and the condition during transport and storage (^) NPS and OPS are the preferred specimens (^) Two specimens are required to maximize sensitivity for detecting viruses, therefore, collecting combined NPS and OPS specimens would be the most effective approach
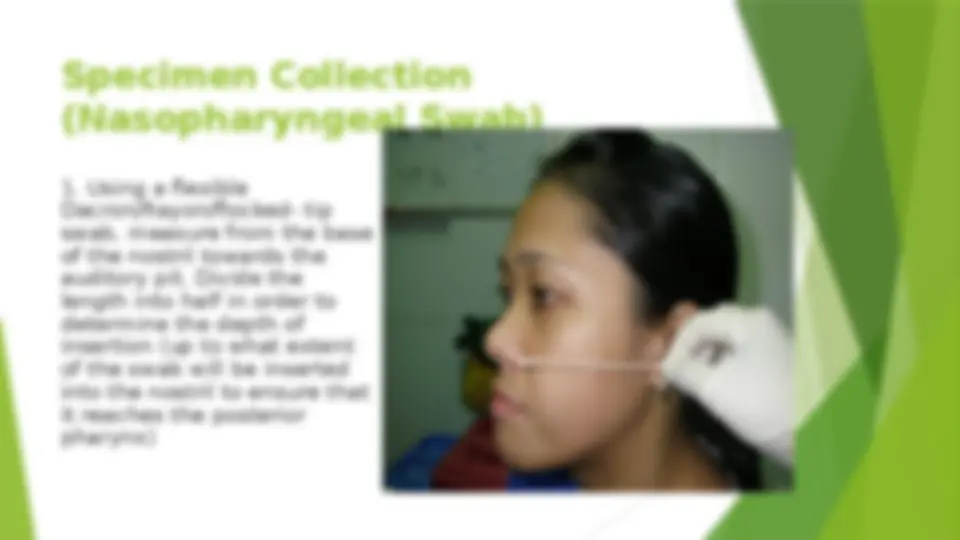
Only sterile Dacron, Rayon, or flocked tip swabs with plastic shafts shall be used Flocked swabs shall be used for NPS collection because it comprise of many thousands of perpendicularly sprayed on short nylon fibers to the tip of an applicator, thus it collect more sample than traditional swabs, and very efficiently release the sample when in contact with liquid.
(^) Label the UTM tube using a marking pen with the Patient’s Full Name, age, gender, specimen type and date and time of collection. The information on the label must be legible. Labels must remain attached under all conditions of storage and transport.