Download NR 507 EDAPT Week 4 Urinary System Pathologies Verified Assignment 2024-2025 and more Assignments Nursing in PDF only on Docsity!
NR 507 EDAPT Week 4 Urinary System
Pathologies
Urgency is a common symptom of a lower urinary tract infection (UTI). It is characterized by a strong and sudden need to urinate. The other options (decreased urination, fever, and flank pain) are not typical symptoms of a lower UTI
Urinary Tract Infections
Bacteria from the gut can invade the urinary epithelium to cause inflammation and infection anywhere along the urinary tract such as the urethra, bladder, ureter, or kidney.
More common for women to develop a UTI especially when pregnant, sexually active, during post-menopause with estrogen-deficiency and when being treated with antibiotics.
Men may develop a lower UTI. An upper UTI is less common in men due to the longer urethra and ureter structures that make it more difficult for bacteria to reach the kidney. A foley can also cz UTI. Finally, ppl who experience urinary obstruction, diabetes or neurogenic bladder are also at risk for UTI.
Complicated or uncomplicated, upper vs. lower tract disorders.
The pathophysiology of a UTI is simple. First, bacteria enter and contaminate the lower urinary tract. This causes the colonization of bacteria in the urethra and the bladder which triggers an inflammatory response in the lower urinary tract. Neutrophils are recruited to the area where the bacteria are present. The bacteria multiply which allows them to evade the immune system due to virulent factors. For example, Escherichia coli can bind to cells in the lower urinary tract and hide from the immune cells. The bacteria can form biofilms. A biofilm is any group of microorganisms that allow them to stick to one another and adhere to surfaces that help them survive. If the UTI progresses or is not treated, or if the patient is immunocompromised, the bacteria can ascend to the kidneys and colonize there. At this point, the infection becomes an upper UTI. If left untreated, the bacteria can spread into the circulation via the renal veins causing bacteremia or septic shock.
UTI Risk Factors
Pregnancy: During pregnancy, progesterone relaxes smooth muscle that causes stasis of urine, allowing the bacteria to colonize. Also, the female ureter is shorter and allows for the entrance of bacteria into the urethra. Post-menopausal: The lack of estrogen results in vaginal and urethral dryness that promotes an environment for bacteria to grow. Sex: bacteria can be easily introduced into the urethra. If spermicides are used during sexual intercourse, this also puts the woman at risk for a UTI. Catheterization: especially in females. The catheter itself can introduce infections directly into the bladder. The neutrophils enter the area to further promote inflammation. Fibrinogen accumulates on the catheter which provides an ideal environment for the attachment of uropathogens that express fibrinogen-binding proteins. After the initial attachment to the fibrinogen-binding proteins on the catheter, the bacteria multiply to form biofils. This results in epithelial damage to the urinary tract that leads to a kidney infection.
Lower vs. Upper Tract Disorders
A UTI can occur anywhere along the urinary tract and can be associated with another issue in the area. For ex, if the infection occurs at the opening of the urethra, then the condition is termed urethritis. Cystitis (bladder) is a condition of the lower urinary tract that denotes a bladder infection. Cystitis can occur in both females and males. In males, the cystitis may be a/w prostatitis.
It just provides an indication of enzyme activity and the presence of inflammation. Using the urinalysis to diagnose a UTI is covered in a section below. Initially, a urine dipstick can be performed to identify hematuria,
proteinuria, and the presence of nitrites. The presence of nitrites is
highly specific for bacterial infection. Person can have a negative urine dipstick but still present with s/s of a UTI. If this is the case, then the NP can send the urine for a culture and sensitivity (C&S) test and microscopy. On microscopic exam , a patient with cystitis will have a **WBC
5000 high power field (hpf) and hematuria**. For the pt w/ pyelonephritis , the urine will present with WBC casts. The presence of casts in the urine indicates that the protein in the lumen of the kidney tubules has solidified, especially in the nephron. This indicates kidney disease rather than a lower UTI.
(LOWER) Cystitis (bladder infx): WBC>5000 &
Hematuria
(UPPER) Pyelo: WBC casts
Uncomplicated vs. Complicated Urinary Tract
Infections (UTI)
Uncomplicated UTI: the urinary tract and renal function is normal. Complicated UTI: there is decreased renal function and an abnormal UT.
WBC casts = presence of kidney involvement which requires a more complicated treatment plan.
The severity of the UTI can also be determined based on the interventions that are necessary to treat the infection. The more intervention required, the more complicated the infection. In general, ppl are treated for a UTI only when they are symptomatic. Although the urine results may confirm a UTI, if the patient denies symptoms, then an antibiotic is not prescribed. *** The exception would be during pregnancy due to the ureteral dilation that occurs that increases the risk for pyelonephritis. Even though she may be asymptomatic, treatment would be initiated to prevent damage to the fetus in utero.
Uncomplicated, symptomatic UTI (cystitis): 3-7 days of abx.
Complicated UTI (pyelo): IV abx until the patient is afebrile, followed by a course of oral antibiotics.
A referral to a urologist is necessary if the individual does not respond to antibiotic treatment or if there are recurrent UTIs (>= 3/year). Bc upper UTI is uncommon in males, they should be referred to a urologist. Hematuria would warrant a referral to the urologist to determine the presence of significant renal disease. If vaginal discharge or itching, the NP may need to include a genital exam as well to r/o a STI.
Common Organisms that Cause Urinary Tract
Infections
E. Coli, Staphylococcus saprophyticus, Proteus Mirabilis, and Klebsiella.
E. coli 80%, fecal matter. In healthy individuals, they can maintain a sterile urinary tract and bladder. Even when bacteria enter the bladder, the immune defenses can prevent it from clinging to the walls of the bladder or the upper UT. A UTI will occur when bacteria overwhelm the defense mechanisms allowing it to quickly reproduce.
A UA is used to diagnose a UTI. If nitrites are present, this indicates that the causative organism is gram negative. A urine culture may also be performed to determine infection. A positive culture indicates >100,000 colony forming units/ml.
Using the Urinalysis to Diagnose a Urinary Tract
Infection
A dipstick can be used to identify leukocyte esterase and nitrites. Nitrites detect the presence of the Enterobacteriaceae ( gram negative bacteria) family that converts nitrates into nitrites. But some bacteria are unable to produce nitrites (Enterococcus). Therefore, person may still have a UTI even if nitrites are not present via the dipstick. The presence of nitrites is the most specific finding and has the highest positive predictive value. (Nitrites: causative bacteria is gram-negative) Leukocyte esterase, WBCs and even bacteria on microscopic exam are not specific and therefore, do not necessarily indicate infection. The dx of a UTI needs to also consider the presence of symptoms and a
Benign Prostatic Hyperplasia
The purpose of straining in BPH is to overcome the obstruction encountered during urination. True. Person strains to overcome the obstruction in order to release the urine. BPH does not lead to prostate cancer. The peripheral zone of the prostate is the largest zone. On a digital rectal exam to assess the quality of the prostate, the NP would be concerned with which of the following findings? A rubber-like quality of the prostate. A hard nodule - can indicate prostate cx A lack of pain on palpation. A soft-smooth prostate.
Pathophysiology of BPH
In BPH, there is enlargement of the prostate gland by an increased number of benign cells. It is common in men >50 yrs. It is considered a normal part of aging. The prostate is a small gland that is shaped like a walnut located under the bladder and in front of the rectum. The urethra passes through the prostate before reaching the penis. This portion of the urethra is called the prostatic urethra.
Location of the Prostate
The prostate is covered by tough connective tissue and smooth muscle and can be divided into zones. Peripheral zone: largest, located in the outermost posterior area. Most (75%) of the prostate’s glandular tissue is in the peripheral zone. Central zone: 25% of the glandular tissue. The ejaculatory ducts that form with the urethra is also located here. Transitional zone: 5% and a portion of the prostatic urethra. This area also contains transitional cells that can also be found in the bladder.
which converts testosterone into the more potent dihydrotestosterone.
Since androgens are steroids, they can cross the cell membrane and bind to the androgen receptors in the cell’s nucleus. This inhibits apoptosis. This allows the luminal and basal cells in the prostate to keep growing and multiplying. Dihydrotestosterone is much more potent than testosterone because it can combine to androgen receptors much longer.
After 30, men produce about 1% less testosterone/year. But 5-alpha reductase activity increases with age. Even with less testosterone, dihydrotestosterone can increase. Normal prostate cells respond to the increase in dihydrotestosterone by living longer and multiplying. That is the underlying cause of BPH. This is a normal process of aging. By age 60, the majority of men will develop BPH and over 90% have it by the age of 85 years of age.
No risk to develop cellular mutations that lead to prostate cancer. Instead, the entire prostate gland enlarges in a uniform fashion with the formation of hyperplastic nodules. On palpation, they feel smooth, elastic, and firm, can be mistaken for prostate cancer. The hyperplastic nodules is in the inner portion of the gland, around the prostatic urethra in the periurethral zone. When the nodules and prostate tissue compress the prostatic urethra, it becomes more difficult for urine to pass through. In response, the smooth muscle of the bladder will contract harder, which leads to bladder hypertrophy, where the bladder walls thicken and become irritated. The stagnation of urine -> UTI.
Clinical Presentation of BPH
Symptoms of BPH may become prevalent when the prostatic urethra becomes obstructed. Dribbling (weak and inconsistent urine stream). Straining as an attempt to overcome the obstruction during urination. Pain on urination (dysuria) Initiating urination (hesitancy). Constant sense of incomplete bladder emptying, increases the frequency of urination at night (nocturia).
DX:
BPH can be dx by performing a digital rectal exam (DRE): The NP palpates the anterior wall of the rectum which lies along the posterior prostate. If enlarged, the NP can suspect BPH. If hard nodules are palpated, this could be a sign of prostate cancer. Levels of Prostate Specific Antigen (PSA) that is produced by healthy prostate cells are also elevated in BPH since there are more cells around to produce it.
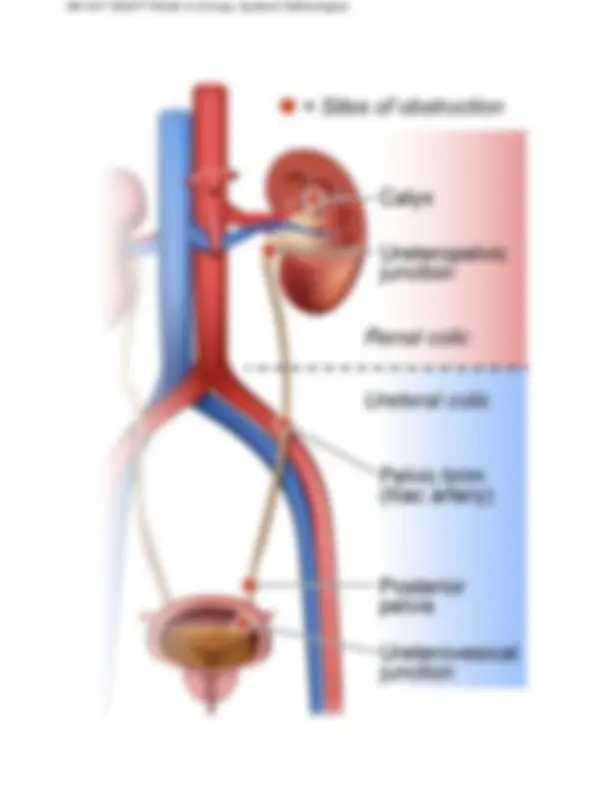
without difficulty. Stones that are > 1.0 cm are likely to cause an obstruction. The most common sites of stone obstruction: ureteropelvic junction, intersection of ureter and iliac vessels, and the ureterovesicular junction.
obstruction and spasm. The characteristic of this pain begins mild and then greatly increases. The pain begins in the flank and radiates to the groin. As the stone moves, the pain will be in the location of where the stone is located. Hematuria : found in 90%! While passing through the urinary tract, the stone will injure the urinary structures. It can also be a/w N/V.
Diagnosis of the renal stone is confirmed through urinalysis. The
patient can have either microscopic or gross hematuria. The pH of the urine will be identified to help determine the type of stone. If the patient passes the stone, it should be taken for analysis to determine the type of stone. X-ray of the kidney, ureter, and bladder (KUB) will also be performed to help determine the type of stone. Uric acid and cysteine stones will not be visible on x-ray since they are radiolucent.
The gold standard for diagnosing a renal stone is CT scan because all types of stones can be seen. An ultrasound can be performed for those individuals that cannot tolerate radiation (pregnancy). It is not the best test for diagnosing a kidney stone because it poorly isolates the stone.
TX:
Treat pain and increase fluid intake. Lithotripsy : a non-invasive procedure, performed if the stone lodges on the way out. It breaks the stone down into smaller fragments. Percutaneous nephrolithotomy: invasive, If lithotripsy fails. *Discuss prevention measures with pts since 1/2 with renal stones will have a reoccurrence w/in 10 yrs again.
Encourage: adequate hydration, a balanced diet. Calcium restriction is not recommended because it can increase oxalate absorption and decrease urinary excretion of calcium.
Urinary Incontinence
The location of the internal sphincter is under the urogenital diaphragm. False. The internal sphincter is located in the bladder.
The levator ani muscle plays a major role in constriction of the external sphincter. True. When the abdomen contracts, especially when abdominal pressure is exerted on the bladder.
The relay station in the brain that plays a major role in regulating micturition is: pontine micturition center (PMC) located in the brainstem
Which of the following actions will relax the detrusor muscle of the bladder? Activation of Beta-2 receptors by the sympathetic nervous system.
When the bladder is empty, there is detrusor muscle relaxation and internal and external sphincter constriction. True.
Bladder Anatomy
The levator muscle is the most important in the urogenital diaphragm.
Bladder Physiology
There are 2 ways to relax the detrusor muscle :
- Activation of Beta-2 receptors by the sympathetic nervous
Atrophic vaginitis: this is atrophy of the vaginal walls, bladder and urethra that occurs in estrogen-deficient post-menopausal women. With estrogen replacement, UI symptoms may subside.
Drugs: many: anticholinergics prevent relaxation of the bladder; Anti- Parkinson drugs, alpha-agonist/antagonist (remember that alpha receptors are found in the internal sphincter). Alpha- agonist -> over -contraction -> over flow incontinence; an alpha- antagonist -> stress incontinence. Diuretics and ACE inhibitors increase frequency of urination -> urge incontinence, Ca channel blockers prevent the internal and external sphincters from contracting; sedatives and hypnotics.
Psychological issues: depression.
Excessive fluid intake or excessive urination in the case of polydipsia experienced by the diabetic patient.
Restricted mobility: has the urge to urinate but is unable to ambulate to the bathroom ( functional incontinence).
Stool impaction: severe constipation can compress the bladder and lead to urination.
Stress Incontinence
Urine leakage a/w abdominal pressure. Increased abdominal pressure occurs with coughing or sneezing. When pressure is increased there will typically be a small amount of urine released. In men , the main cause of stress incontinence is surgery, especially after a TURP. In women , the major cause of stress incontinence is hypermobility of the external sphincter. The external sphincter moves downward. A vaginal delivery is the most common cause of the downward movement of the external sphincter. The levator ani muscle usually contracts with the abdominal muscles as when the individual coughs. Pressure is placed on the bladder. At the same time the levator ani muscle contracts and cause constriction of the external sphincter that will constrict the urethra to prevent urine leakage. In women with stress incontinence, the levitar ani is above the sphincter because the sphincter has moved downward. The levator ani, therefore, will not be able to contract, which will allow the urine to leak all the way through. Women may also have stress incontinence due to sphincter deficiency caused by vaginal atrophy. This is common in estrogen-deficiency post-
menopausal women. Suggest pelvic floor exercises
Urge Incontinence
Sudden urge to urinate but is unsuccessful on attempt to urinate, or urination occurs rapidly when en-route to the bathroom. The cause is usually due to overactivity or hypersensitivity of the detrusor muscle. Urge I. may be r/t decreased bladder compliance that prevents the bladder from holding enough urine. UI can be differentiated from an overactive bladder. An overactive bladder is where the individual has urgency and frequency but may or may not have urge incontinence.
TX : bladder training to increase bladder capacity and increase pelvic muscle tone. Lifestyle changes: fluid management and dietary changes. Avoid spicy foods that increase urination. Oxybutynin to decrease bladder hypersensitivity.
Overflow Incontinence
Bladder distention c/b sphincter malfunction that prevents urine from flowing out of the bladder or a problem with bladder contraction. It is r/t partial obstruction of the bladder neck (e.g. BPH in men and pelvic prolapse in women). It may also be c/b medications, fecal impaction, diabetes spinal cord injury or urethral stricture. In OI, there is decreased detrusor muscle contraction. Medications can weaken the detrusor muscle; a spinal cord lesion can decrease the signal going to the detrusor muscle, and long-standing overdistention of the bladder reduces its ability to contract. The patient will present with frequency, urgency, dribbling and hesitancy.