



NR507 week 1 edapt guide updated
version
Advanced Pathophysiology

















































































Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
NR507 week 1 edapt guide updated version
Typology: Study Guides, Projects, Research
1 / 91

This page cannot be seen from the preview
Don't miss anything!
-Immediate hypersensitivity is mediated by IgE antibodies, which resulting an allergy, anaphylaxis, or atopic disease. The NP should expect the client to have a type 1 hypersensitivity to recent medication use, which can include these immediate reactions as clinical manifestations: urticaria, wheezing, vomiting, and diaphoresis.
Type 4 = mediated by cellular response.
Pathophysiology of Type 1 Allergic Reaction Types of Hypersensitivity Reactions Localized Effect: When the immune system is first exposed to the antigen, it responds by forming IgE, which sensitizes the basophils and mast cells in tissues. During the second exposure to the same antigen, the immune system releases mediators (histamine). Vasodilation and increased permeability of blood vessels leads to inflammation, including edema, redness, and pruritus. Systemic Effect: When subsequent exposure to the same antigen occurs, the antigen binds with IgE antibodies. Mast cells release large amounts of histamine into general circulation. Cardiovascular system: Vasodilation and increased capillary permeability cause decreased blood pressure, faintness, or weakness. Skin nerve endings are irritated, leading to itching. In the lungs, constriction of bronchioles and release of
J.S. is a 64-year-old-female who presents to the primary care office with complaints of low back pain and burning on urination. She also indicates that she has been urinating frequently and has had to wear a pad because she also is experiencing urgency and she is afraid she might “leak.” She tells the NP that she suspects that she has a UTI. She reported that is has been at least 2 years since she had a UTI and was treated with an antibiotic but cannot remember its name. She denies any medication or food allergies. After conducting a thorough health history and physical exam, the NP diagnosed the client with uncomplicated UTI and orders a course of sulfamethoxaole/trimethoprim (Bactrim DS). The next day, J. S. returns to the office in a panic to report she has just taken her first dose of the medication about an hour ago. She began to feel anxious followed by wheezing in the chest and dizziness. She first called her daughter, who reminded her that she is allergic to sulfa drugs. J. S. is immediately examined by the NP. The subjective and objective findings are: Subjective:
At this point, inflammatory mediators are released. These include histamine, leukotrienes, and prostaglandins. Constriction of bronchial smooth muscle also occurs, which explains her respiratory symptom of wheezing. Based on the localized and systemic symptoms, the NP can diagnose the client with anaphylactic reaction, a Type I hypersensitivity reaction.
Camille Rutherford, 45-years-old Chief Complaint: red, dry, itchy skin on arms and legs, shortness of breath, wheezing, and cough Medical History: presents with a nonproductive cough, expiratory wheezing, and shortness of breath upon exertion; reports a gradual onset of these symptoms and mentioned that they have been progressively worsening when walking their dog outside Past Medical History: eczema, hypertension Social History: lives at home with daughter and their dog Allergic rhinitis attacks are related to ongoing exposure to specific offending agents. The strongest risk factor for developing asthma is a history of atopic disease (the client has eczema, a form of atopic dermatitis). Environmental factors and allergens—such as high humidity, cold, dry weather, house dust mites, pet fur, and pollen—can place a client at risk for a new diagnosis of allergic asthma. With prior exposure to allergens, Camille was sensitized. Chronic exposure to allergens mediated IgE antibodies to attach to sensitized cells, and with further exposure, IgE caused sensitized cells to degranulate. When degranulation occurs, inflammatory mediators like histamine, leukotrienes, and prostaglandins are released to produce several effects on the body, such as shortness of breath and wheezing. Constriction of bronchial smooth muscle also occurs, which explains her respiratory symptoms: shortness of breath, cough, and wheezing. The NP can diagnose the client with a type I hypersensitivity reaction based on localized and systemic symptoms. The client’s age and history of hypertension are not risk factors.
Type 2 hypersensitivity reactions are immune reactions against a specific cell or tissue. Cells express various antigens on their surfaces, while others are expressed on the membranes of only specific cells (called tissue-specific antigens). Altered tissue-specific antigens are bound by autoantibodies, resulting in tissue destruction by macrophages, neutrophils, natural killers, or complement cells. The symptoms of many type 2 reactions are determined by the tissue or organ
Cytotoxic hypersensitivities can occur with hemolytic transfusions. The client’s blood must be typed and cross-matched to prevent possible cytotoxic hypersensitivities. Type 2 Cytotoxic Hypersensitivity
Macrophages are the primary effector cells of type 2 responses. A type 2 hypersensitivity response begins with the antibody binding to the antigen and may cause the following:
Graves’ disease symptoms include bulging eyes, enlarged thyroid (goiter), arrhythmia and tachycardia, nausea and diarrhea, tremor, change in menstrual cycles (in females), muscle weakness, headache, weight loss, anxiety and irritability, and increased perspiration. Clinical Application: Type 2 - Hemolytic Transfusion Reaction A hemolytic transfusion reaction is a severe complication that can occur after a blood transfusion. The transfused red blood cells (RBCs) are destroyed by the client’s immune system. M. G., a 27-year-old healthy female, required a blood transfusion 4 hours post- partum after undergoing a C-section. Twenty-four hours later, she and her newborn were released from the hospital in good health. Approximately 1 week later, she came to the primary care office complaining of fever, chills, shortness of breath (dyspnea), and a backache. The NP conducts an exam and the subjective and objective findings reveal the following: Subjective:
Type 3 reactions are not organ-specific and use neutrophils as the primary effector cell. In Type 3 hypersensitivity reactions, immune-complex deposition (ICD) causes autoimmune diseases, which is
often a complication. As the disease progresses, immune complexes accumulate, deposit, and overload the tissue. As the phagocytes, erythrocytes, and complement systems fail to remove excess immune complexes, inflammation sets in. Common immune system-complex reactions include systemic lupus erythematosus (SLE), serum sickness, and what is known as the Raynaud phenomenon (a form of serum sickness). Type 3 Immune Complex Hypersensitivity
Systemic lupus erythematosus (SLE) is an autoimmune, type 3 hypersensitivity reaction in which the body’s immune system attacks its own tissues and organs. In SLE, B- and T-cells become overactive, increasing the production of autoantibodies and activating the complement system and neutrophils. This results in widespread inflammation, tissue destruction, and scar formation and can affect many body systems. Clinical manifestations may be mild, develop slowly, come on suddenly, and be severe enough to require hospitalization.
Drag and drop the pathophysiological processes of a type 3 immune complex hypersensitivity into the correct order. Your response is correct! The pathophysiological processes of a type 3 immune complex hypersensitivity in the correct order are as follows:
Type 4 hypersensitivity reactions are delayed, cell-mediated responses mediated by T- lymphocytes and macrophages. When the individual encounters the antigen, T-cells are activated and move to the area of the antigen. The antigen is taken up, processed, and presented to macrophages, leading to epidermal reactions characterized by erythema, cellular infiltration, and vesicles. T-cells and macrophages sometimes cannot destroy or remove an offending antigen, leading them to encase and contain the invader by forming a granuloma. The formation of multiple granulomas can lead to tissue damage and organ dysfunction. A type 4 reaction can also be present in other autoimmune diseases. For example, T-cell response to type 2 collagen can lead to joint damage in clients with rheumatoid arthritis (RA). T-
cell response to an antigen on the surface of pancreatic beta cells contributes to beta-cell destruction in clients with insulin-dependent (type I) diabetes mellitus. Type 4 Cell-Mediated or Delayed Hypersensitivity
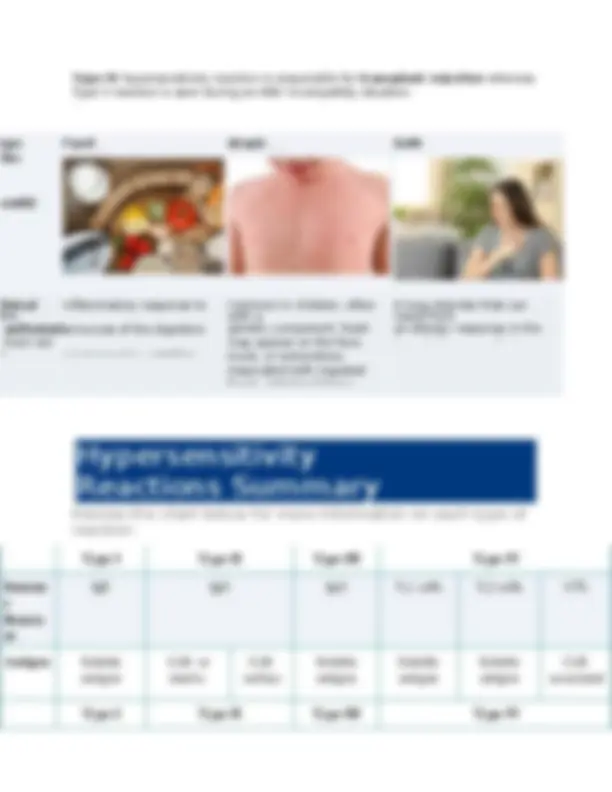
Contact dermatitis is an eczematous, cutaneous skin condition exacerbated by exposure to various foods and environmental allergens. Clients report dryness with pruritus, in which scratching can create or exacerbate open lesions, putting them at risk for infection. J. S. is a 17-year-old male who plays high school football. Last weekend, the team played an out of town game. On the way home from the game, the team bus was stopped because of a fallen tree and other types of brush blocking the road after a severe thunderstorm. J. S. and his teammates removed debris from the road and then proceeded on their trip home. Three days later, while sitting in his math class, he develops severe itching and a rash over his hands, arms, and neck. Later that day, his mother takes him to see the nurse practitioner (NP) at the primary care office. She asks him to share any unusual exposures that he has recently encountered, and he informs her about contact with the road debris a few days earlier. The NP conducts an exam and the subjective and objective findings reveal the following: Subjective:
Anaphylaxis is caused by the body's immune response to an allergen. Allergens are harmless substances that cause an overreaction response in some individuals. Common allergens include foods such as nuts or shellfish, certain medications, insects, or latex. When a person with an allergy comes in contact with their allergen trigger, white blood cells, such as mast cells, released during anaphylaxis is histamine. Histamine causes the dilation of blood vessels and increases heart rates and gland secretion. Other chemicals released during the immune response cause constriction of the airways and increase the permeability of blood vessels. Together, these chemicals cause the suite of symptoms associated with anaphylaxis.
Algorithm for Anaphylaxis Treatment Manage exposure
For each hypersensitivity reaction, click to specify which immunologic mechanism (type 1, 2, 3, 4) causes the clinical condition. Allergic rhinitis = 1 Asthma =