Download NURSING 101Complete Hurst Packet and more Exams Nursing in PDF only on Docsity!
TABLE OF CONTENTS
- Fluids and Electrolytes.............................................................................................
- Acid-Base Balance...................................................................................................
- Burns…....................................................................................................................
- Oncology…..............................................................................................................
- Endocrine.................................................................................................................
- Cardiac.....................................................................................................................
- Psychiatric Nursing….............................................................................................
- Gastrointestinal.......................................................................................................
- Neuro…...................................................................................................................
- Maternity Nursing…..............................................................................................
- Respiratory…..........................................................................................................
- Orthopedics….........................................................................................................
- Renal........................................................................................................................
- Questions.................................................................................................................
- Final Thoughts........................................................................................................
- Evaluations..............................................................................................................
- Table of Contents for CD.......................................................................................
- Pediatric…...............................................................................................................
Hurst Review does not condone the discussion of the NCLEX-
RN exam post- test. Thank you.
NOTICE TO FACULTY
All materials used during any Hurst Review Services seminar are copyrighted
and are not for use without the sole permission of Marlene Hurst in any form
or fashion.
This material is not intended for lecture use by any School of Nursing without
permission.
NOTICE TO STUDENTS
If you are a student who has obtained this book from a past participant of
my workshops...SHAME, SHAME, SHAME!!!
Please understand that this book is written to accompany the live or video
lectures presented in the class itself or my Internet Tutorials.
This book is only an outline of what is needed to pass NCLEX.
I hope you will join me in a live or video class or on the Internet to reap the
full benefits of my materials.
General Class Information
- Please turn off ALL cell phones and pagers.
-This class MAY NOT be recorded in any manner.
(This included tape recording or videoing.)
-Class Time: 8AM-4PM
* Please note that each class is presented in a particular sequence if your
instructor completes the material for that day, you may get out prior to 4
PM.
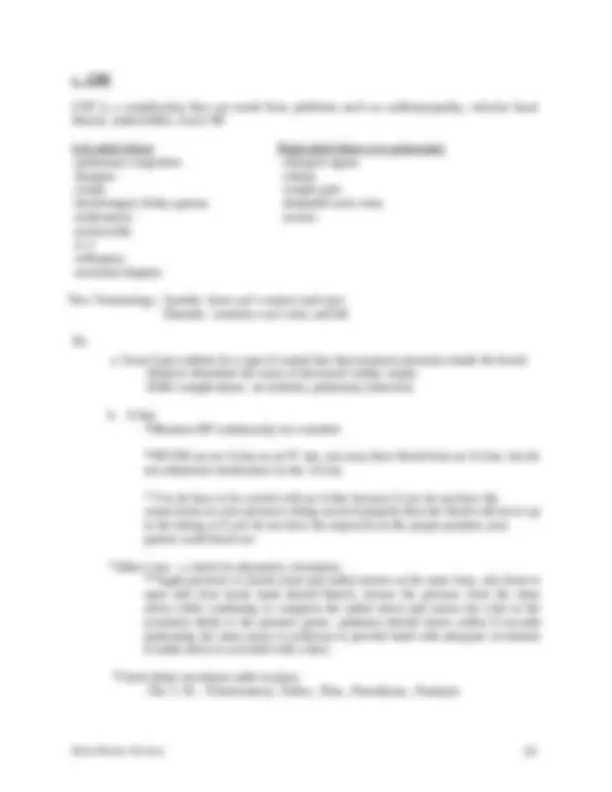
e. ADH (anti-diuretic hormone) Normally makes you retain or diurese? Retain? 2 ADH problems Too Much Not enough Retain Lose (diuese) Fluid Volume Fluid Volume SIADH DI Syndrome of Inappropriate ADH Secretion Diabetes Insipidus Urine Urine Blood Blood *Concentrated makes #’s go up specific gravity, Na *Dilute makes #’s go down ADH lives in pituitary; key words to make you think potential ADH problem: craniotomy, head injury, sinus surgery, transphenoidal hypophysectomy *Another name for anti-diuretic hormone (ADH) is Vasopressin. The drug Vasopressin (Pitressin or DDAVP (Desmopressin acetate) may be utilized as an ADH replacement in Diabetes Insipidus.
f. S/Sx of FVE: Distended neck veins/peripheral veins: vessels are Peripheral edema, third spacing: vessels can't hold anymore so they start to CVP: measured where? ; number goes More..........................................More Lung sounds: Polyuria: kidneys trying to help you Pulse: ; your heart only wants fluid to go If the fluid doesn't go forward it's going to go into the BP: move volume....more Weight: any acute gain or loss isn't fat-it’s fluid g. Treatment: Low Na diet Diuretics Loop *Bumex® may be given when Lasix® doesn’t work. Thiazide (HCTZ) * Watch lab work with all diuretics *Dehydration and electrolyte problems K-sparing Bed rest induces *when you are supine you perfuse your kidneys more h. Interventions: Physical Assessment Give IVF’s slowly to elderly
Quickie IV Fluid Lecture Isotonic: Go in the vascular space and stays there! Examples of Isotonic Solutions: , , Hypotonic: Go in the vascular space, hang out a little while and rehydrate, but they do not stay in the vascular space.....If they stayed in the vascular space they wouldn't be hypotonic...they would be.........................................These solutions go in and hang out and rehydrate, then they move into the cell and the cell burns the remainder up in cellular metabolism. They are hydrating solutions, but they won't drive your pressure up because they do not stay in the vascular space. Hypertonic Solution:
- Volume expander and solution that draws fluids into the vascular space.
- Examples: D10W, 3% NaCl, 5% NaCl, D5 LR, D5 ½ NaCl, D5 NaCl, TPN Hypotonic Solution:
- Causes a fluid shift from the vascular space into the cells.
- Examples: D2.5 W, ½ NaCl, 0.33% NaCl
MAGNESIUM AND CALCIUM
Fact: Magnesium is excreted by kidneys and it can be lost other ways, too (GI tract) Hypermagnesemia Hypercalcemia Causes: Renal Failure Causes: Hyperparathyroidism: too much Antacids Thiazides (retain ) DTR's Muscle Tone Immobilization (you have to bear weight to keep Ca in ) Flushing Arrhythmias bones Warmth LOC Mg makes you Pulse kidney stones Respirations *majority made of calcium Tx: Ventilator Tx: Move! Dialysis Calcium gluconate Fluids! *Calcium gluconate in the presence of magnesium- they inactivate each other Phospho Soda & Fleets enema -both have phosphorous *Ca has inverse relationship with. *When you drive Phos up, Ca goes. Steroids Add what to diet? Safety Precautions? *Must have Vitamin to use Ca. *Calcitonin serum Ca HINT: If you want to get Mg & Ca questions right, think muscles 1st. When your serum calcium gets low parathormone (PTH) kicks in and pulls Ca from the and puts in the blood....therefore, the serum goes up.
SODIUM
Your Na level in your blood is totally dependent on how much water you have in your body. Hypernatremia=Dehydration Hyponatremia=Dilution Too much Na; not enough water Too much water; not enough Na Causes: Causes: hyperventilation -vomiting, sweating then drinking H2O *this only replaces the water heat stroke -psychogenic polydypsia DI *loves to drink S/Sx: -D5W (sugar & water) Dry mouth -SIADH Thirsty - already dehydrated by the time you're thirsty Swollen tongue Neuro changes
- Brain doesn't like it when Na's messed up Tx: Tx: Restrict. Pt needs Dilute pt with IV Fluids Pt doesn't need. Diluting makes serum Na go (^) If having neuro probs: Needs hypertonic saline Daily weights -means "packed with particles" If you've got a Na problem you've I & O got a problem. 3-5% NS Lab work Feeding tube pts - tend to get
Sodium and Potassium have an relationship
POTASSIUM
Excreted by kidneys Kidneys not working well, the serum potassium will go Hyperkalemia Hypokalemia Causes: Causes: kidney troubles -vomiting aldactone - makes you retain. -NG suction -diuretics -not eating S/Sx: Begins with muscle twitching Life- S/Sx: Muscle Cramps Then proceeds to weakness, Threatening & weakness Then flaccid paralysis Arrhythmias Tx: Tx: Dialysis - Kidneys aren't working Give K! Calcium gluconate Aldactone -decreases Eat K Glucose and insulin
- Insulin carries & into the cell
- Any time you give IV insulin worry about & Kaexalate®
- given for hyperkalemia
- exchanges Na for K in the GI tract We have lots of K in our stomach
ACID-BASE BALANCE
Major chemicals you have to remember = Bicarb, Hydrogen, CO 2 Lung chemical→CO 2 Kidney chemicals →B and H There's only one way to get rid of CO 2. What is it? These chemicals can either make you sick or compensate. It depends on which imbalance you have. In respiratory acidosis/alkalosis, which organs are sick? Who's going to fix everything (compensate)? What are the chemicals the kidneys use to compensate with? In metabolic acidosis/alkalosis which organs are sick? If they are sick, who's going to fix things (compensate)? What is the only chemical the lungs have to compensate with? Do the lungs compensate slowly or quickly? Do the kidneys compensate slowly or quickly?
Hypoxia may be one of the first signs of Respiratory Acidosis Compensation acidosis metabolic respiratory lungs compensate kidneys compensate RR to blow off C0 2 retain/secrete B PCO 2 alkalosis excrete H Bicarb on ABG’s metabolic respiratory lungs compensate kidneys compensate RR to save C0 2 excrete B PCO 2 Respiratory Acidosis (hypoventilating) Is this a lung problem or a kidney problem? What's the problem chemical? Do we have too much or too little of this chemical in the body? How did this happen? Who's going to compensate? Increased C0 2 →Decreased LOC retain H Bicarb on ABG’s Increased C0 2 → Decreased 02 early hypoxia late hypoxia Treatment→ Fix the problem!!!! Drug to help correct acidosis? Be aware of drugs that decrease RR. Restless pt? Restlessness think Hypoxia FIRST
BURNS
-The risk of death increases in the very and the very. -Where do most burns occur? -After a burn many different pathophysiological changes occur. WHY? a. Why does plasma seep out into the tissue? Increased permeability b. When does the majority of this occur? c. Why does the pulse increase? Anytime you're in a FVD, Pulse d. Why does the cardiac output decrease? Less to pump out. e. Why does the urine output decrease? Kidneys are either trying to hold on or they aren't being f. Why is epinephrine secreted? Makes you , shunts blood to vital organs g. Why are ADH and aldosterone secreted? Retain & with aldosterone and Retain with ADH Therefore your blood volume will go -What is the most common airway injury? poisoning -Normally oxygen should bind with hemoglobin. Carbon monoxide can run much faster than oxygen.... Therefore, it gets to the hemoglobin first and binds.......Can oxygen bind now........yes/no
- Carbon monoxide poisoning cannot be determined with O2 saturations; the sat monitor picks up anything that is bound to hemoglobin so if carbon monoxide is bound to the Hb then the sat may appear normal
- Carboxyhemoglobin: blood test to determine carbon monoxide poisoning Now the patient is. Tx:
From this information do you think it would be important to determine if the burn occurred in an open or closed space? -When you see a patient with burns to the neck/face/chest you had better think what? -A patient is burned over 40% of their body. How do you think this is determined? *Estimate of Total Body Surface Area Head= Each arm= Each leg= Anterior trunk= Posterior trunk= Genitalia= -One of the most important aspects of burn management is. -It is not uncommon for albumin to be given after a major burn. (Not given during the first 24 hours). You know that albumin holds onto in the vascular space. -This will increase/decrease the vascular volume. -What will it do to kidney perfusion? -What will it do to BP? -What will it do to cardiac output? -Will this help correct a fluid volume deficit? -When you start giving a patient albumin you know that the vascular volume will increase. What will happen to the work load of the heart? -If you stress the heart too much you know that the patient could be thrown into fluid volume . -If this occurs what will happen to CO? -What will the lung sounds be like? -On any patient who is receiving fluids rapidly, what is a measurement (hint: heart) you can take hourly to make sure you’re not overloading them? -Is it important to know that the burn occurred at 11:00 p.m.? Why? Because you know that fluid therapy (for the first 24 hours) is based on the time the injury occurred, not when treatment was started.
Antacids: aluminum hydroxide, Amphogel®, or magnesium hydroxide, Milk of Magnesia® H2 Antagonist: Zantac ®, Pepcid ®,Axid ® Proton Pump Inhibitors: Protonix ®, Nexium® -What kinds of things do you look for to determine if any airway injury has occurred? -A foley catheter was inserted so you could measure urine output. -How often will this need to be monitored? -Is it possible that when you insert the catheter that no urine will return? Why? Kidneys are either attempting to the fluid or they might not be being perfused adequately. -What would you do if the urine was brown/ red? -If there is no urine output or if it is less than 20cc/hour, what would you start worrying about? -What drugs might be ordered to increase kidney perfusion? -After 48 hours, the patient will begin to diurese. Why? Because fluid is going back into the space. Now we have to worry about fluid volume. What will naturally happen to urine output during this time? -The patient’s serum potassium level is 5.8. You know that potassium likes to live inside or outside of the cell? With a burn, what happens to cells? So, what happens to the number of potassiums in the serum (vascular space)? Therefore, you better monitor your patient for which electrolyte imbalance? hypokalemia or hyperkalemia -Why do you think Mylanta®, Protonix®, Pepcid®, and Reglan® are ordered? -Why do you think the doctor wants the patient to be NPO and have an NGT hooked to suction? -If a patient doesn’t have bowel sounds, what will happen to the abdominal girth? -Do you think the patient will need more or less calories than before? -The NGT will be removed when you hear what?
-When you start GI feedings, what could you measure to ensure that the supplement was moving through the GI tract ok? -What is some lab work you could check to ensure proper nutrition and a positive nitrogen balance? -Since the patient has 2 nd^ and 3 rd^ degree burns, is it possible that they could have problems with contractures? -Since they have burns on their hands, what are some specific measures that may be taken? -Neck? -If a patient has a perineal burn, what do you think the number one complication will be? -What is eschar? -Does it have to be removed? -If it’s not removed can new tissue regenerate? -What likes to grow in eschar? -What type of isolation will you use with the patient? -Travase® or Collagenase®: enzymatic drug→ eats dead tissue -Don’t use on face -Don’t use over large nerves -Don’t use if pregnant -Don’t use if area opened to a body cavity -Hydrotherapy is also used to debride.