Download Nursing Bundle all systems and more Cheat Sheet Medical Microbiology in PDF only on Docsity!
Med-Surg Study Guide
- Burns
- Cancer
- Cardiac
- Cardiac Basics
- Heart Failure
- Coronary Artery Disease
- Angina Pectoris
- Myocardial Infarction
- Electrolyte Imbalances
- Sodium
- Potassium
- Calcium
- Magnesium
- Phosphorus
- Chloride
- Relationships
- Endocrine
- Endocrine System
- Thyroid Gland and Disorders
- Hyper- and Hypoparathyroidism
- Adrenal Glands and Disorders
- DI vs SIADH
- Diabetes Mellitus
- Gastrointestinal
- The Digestive System
- Gastroesophageal Reflux Disease
- Peptic Ulcer Disease
- Inflammatory Bowel Disease
- Diverticulosis and -itis
- Celiac Disease
- Hepatitis
- Cirrhosis
- Pancreatitis
- Cholecystitis
- Appendicitis
- Hematologic Disorders Table of Contents
- Musculoskeletal
- Musculoskeletal System
- Fracture
- Osteoarthritis
- Rheumatoid Arthritis
- Osteoporosis
- Gout
- Neurology
- Brain Anatomy and Physiology
- Stroke
- Seizure
- Increased Intracranial Pressure
- Multiple Sclerosis
- Parkinson's Disease
- Myasthenia Gravis
- Guillain-Barre Syndrome
- Renal
- Kidneys, Nephrons and RAAS
- Chronic Kidney Disease
- Acute Kidney Injury
- Renal Calculi
- Urinary Tract Infections
- Glomerulonephritis
- Nephrotic Syndrome
- Dialysis
- Diuretics
- Respiratory Disorders
- Lung Anatomy and Physiology
- Pneumonia
- COPD
- Asthma
- ARDS
- Pleural Effusion
- Shock
Epidermis
Dermis
Fat Bone Muscle Sweat gland Hair Follicle Superficial partial thickness (1st degree) Deep partial thickness (2nd degree) Full thickness (3rd & 4th degree) Thermal - Most common - caused by flame, flash, scald or contact with hot objects (liquid, steam, fire); e.g. from cooking, burning leaves, smoking Chemical - caused by contact with acids, alkali or organic compounds - no heat needed acids (e.g. hydrochloric, oxalic, hydrofluoric) alkali (e.g. cement, oven/drain cleaners, heavy industrial cleaners); harder to treat because adheres to tissue organic compounds (e.g. phenols and petroleum products) Electrical - caused by intense heat generated from an electric current that passes through the body and damages tissue hard to determine extent of damage because most of damage is below the skin - 'iceberg effect' Cold - caused by cold exposure to skin; frostbite Radiation - caused by sun or cancer treatment Friction - caused by abrasion to skin road rash (car accident) rope burn Damage to the skin's integrity by some kind of energy source BURNS Types of Burns Skin Structure and Degree of Burn Depth of Burn Extent of Burn Calculated in % of TBSA Use Rule of 9s (see next page) Location of Burn Patient risk factors If they experienced an inhalation injury or not Burn Severity Depends on: Location of Burn - potential problems Respiratory - face, mouth, neck, trunk (due to edema or eschar) Disability - Eyes, hands, feet, joints (due to damage to nerves) Infection - Perineum (due to infection from urine/feces) and ears, nose (thin skin) Trouble Healing - Ears, nose (due to thin skin and poor blood supply) Compartment syndrome - Full thickness circumferential burns
st Degree Superficial partial thickness Epidermis only Least severe Heals in 7 days Erythema Blanching on pressure Pain/mild swelling Skin pink/red Warm to touch No blisters Usually no scarring nd Degree Deep partial thickness Epidermis and dermis Very painful Blisters Redness that blanches Swelling (mild - moderate) Shiny red/pink and moist If severe, may need skin grafting rd Degree Deep full thickness All layers destroyed and extends to muscles, bone, ligaments NO pain sensation Black, charred with eschar Months to heal Will need skin grafts th Degree Full thickness All layers are damaged Not painful due to damage to nerves Skin will NOT heal - needs skin grafting Will take months to heal Dry, leathery hard skin (eschar) May be black, yellow, red, waxy white Depth of Burn Eschar - dead tissue - dangerous if around torso or extremity; will need to be removed via escharotomy In Full Thickness, watch for acute tubular necrosis (ATN), due to the release of myoglobin and hemoglobin that block kidney tubules. Pre-Hospital and Emergency Care At scene - Remove from source of burn Stop the burning process Small thermal burns (10% or less TBSA) Cover with cool, clean, tap water-dampened towel If >10% TBSA or electrical/inhalation burn and patient unresponsive: Focus on CAB C - Circulation - check for pulse and elevate burned limb(s) A - Airway - check for patency, soot around nose and on tongue, singed nasal hair, darkened oral or nasal membranes B - Breathing - check for ventilation If patient is responsive, do A → B → C Cool large burns no longer than 10 minutes Do not immerse in cool water Do not cover with ice Do remove as much burned clothing as possible Do wrap in sheet/blanket Chemical burns - remove all chemicals from skin; remove clothing containing chemical and then flush skin with water Monitor patient with inhalation injury for signs of respiratory distress
Phases of Burn Management Emergent Phase Onset of burn until 24 - 48 hours post Pathos: Increased capillary permeability causes: Plasma fluid to leave intravascular space Na+ & Albumin follow Fluids shift to interstitial tissue Edema results Blood thickens Interventions: IV access (2) Calculate fluids (lactated Ringer's) using formula Electrical burns need higher fluids and possibly osmotic diuretic (mannitol) Catheter to monitor urinary output Monitor every hr Goal >30cc/hr Albumin may be administered Monitor urine for Hg and Mb (ATN) Time required to resolve the immediate, life-threatening problems Main concerns: onset of hypovolemic shock and edema formation Hypovolemic shock is the greatest initial threat to a patient with a major burn Phase ends when fluid mobilization and diuresis begin Wound Care: Open or Closed Open: open to air with topical antimicrobial - often limited to facial burns Closed: topical antimicrobial and area covered with sterile dressing Debridement - necrotic tissue removed Positioning - no pillows (esp with neck/ear burns); rolled towel under shoulders Elevate extremities - helps prevent edema and contractures Do not let 2 burn areas touch (to prevent webbing) ROM/splints to prevent contractures Premedicate w/pain meds before dressing changes or debridement! Graft types: autograft (self), allograft (cadaver), CEA (grown from pt own skin), artificial skin ↑ Hct, ↑ K+, ↓Na+, ↓ WBC ↓ Fluid may lead to hypovolemic shock: ↑ HR ↓ CO ↓ BP Pain meds via IV initially; opioids May need intubation (esp face/neck burn) Wound care can begin once proper airway, circulation and fluid replacement achieved Monitor for: Hypovolemic shock Electrolyte imbalances Renal failure GI problems
Normal cells proliferate only at cell death or when physiologically necessary (such as infection) and exhibit contact inhibition (respect cell boundaries) Cancer cells proliferate indiscriminately and have no contact inhibition; form tumor Normal cells mature and perform one specific function Cancer cells have a defect and perform more than one function Defective cell proliferation: Defective cell differentiation: Initiation - mutation/change in DNA occurs (exposure to carcinogen) Most cancers not due to inherited genes, but to damage during lifetime Carcinogens (cancer-causing agents) Chemical - e.g. benzene, arsenic, formaldehyde Radiation - e.g. UV radiation Viral - e.g. Epstein-Barr virus, HIV, Hep B Promotion - proliferation of ALTERED cells by promoters (e.g. dietary fat, obesity, cigarette smoke, alcohol consumption); Reversible at this stage Latent period - 1-40 yrs between initial genetic alteration and clinical evidence Progression - Increased growth rate of tumor, increased invasiveness, metastasis (spread of cancer to a distant site). Most frequent sites of metastasis are lungs, liver, bone, brain and adrenal glands Cancer Disease characterized by uncontrolled and unregulated growth of cells Pathophysiology Occurs in all ages, higher in men than women The second most common cause of death in U.S 1/3 of all cancer-related deaths in U.S. due to tobacco use, unhealthy diet, physical inactivity and/or obesity 3 Stages of Cancer Cancer
Leukemias and lymphomas - cancers of the blood and blood-forming tissues Carcinomas - cancers of the cells that line the skin, lungs, digestive tract, and internal organs Sarcomas - cancers of the mesodermal cells (e.g. muscles, blood vessels, bone) Types of Cancer Anatomic Site Histology (grading) - I, II, III, IV, X (better prognosis → worse) Anatomic extent of disease (varies widely per cancer type) Cancer Classification Based on: ↓exposure to carcinogens (smoking, tanning beds, sun) Diet - ↑veggies/fruits/whole grains, ↓dietary fat and preservatives Limit alcohol intake; regular exercise Healthy weight; 6-8 hrs sleep/night;↓stress Regular physical exam; self-exam Follow cancer screening guidelines; know 7 warning signs Prevention ** KEY C hange in bowel or bladder habits A sore that does not heal U nusual bleeding or discharge T hickening or a lump in the breast/body I ndigestion or difficulty swallowing O bvious change in a wart or mole Nagging cough or hoarseness
Diagnosis - Pathologic evaluation of a tissue sample is the only definitive means to diagnose cancer Surgery - to eliminate or reduce the risk of cancer development; includes prophylactic removal of non-vital organs (e.g. mastectomy, thyroidectomy, hysterectomy) Chemotherapy (antineoplastic therapy); a systemic therapy and a mainstay of cancer tx for most solid tumors and hematologic malignancies (e.g. leukemia, lymphomas) Goal is to eliminate or reduce the number of cancer cells in the primary tumor and metastatic tumor site Methods: oral or IV (most common; may cause local tissue breakdown/necrosis) Regional chemotherapy - delivery of drug directly to the tumor site; reduced systemic toxicity Chemotherapy agents cannot distinguish between normal cells and cancer cells Side effects are result of destruction of normal cells, especially rapidly proliferating ones (e.g. bone marrow, lining of GI system, skin/hair/nails) Long-term side effects: damage to heart, lungs, liver, kidneys Radiation therapy - local therapy; high-energy beams delivered into tissue to break the chemical bonds in DNA; only has effect on tissues within tx field Teletherapy - exposed to radiation via machine Brachytherapy - implanting radioactive material directly into tumor Immunotherapy (biologic therapy); uses the immune system to fight cancer; e.g. cytokines, vaccines, monoclonal antibodies (most successful) Targeted therapy - acts on specific targets associated with cancer; does less damage to normal cells than chemo; e.g. tyrosine kinase inhibitors Hormone therapy - can block the effects of certain hormones that enhance the growth of cancer (e.g. corticosteroids, estrogen receptor blockers, androgen receptor blockers) Hematopoietic stem cell transplantation (HSCT)- originally called BMT or PSCT Goal is to eradicate diseased tumor cells and/or clear the bone marrow of its components to make way for engraftment of transplanted, healthy stem cells; used for pt w/tumors resistant to chemo or rad tx Uses high levels of chemo and/or radiation to clear the bone marrow; healthy stem cells are infused afterwards Intensive procedure with high risks Complications: bacterial, viral, fungal infections; graft-vs-host disease Treatment Malnutrition - Seen as fat/muscle depletion Small meals/↑cal/ ↑pro Encourage nutrition supplements (Ensure); ↑cal/↓density foods (e.g. oils, butter) Weigh at least 2x/wk Oncologic emergencies - life-threatening Obstructive - tumor obstruction of an organ or blood vessel (e.g. superior vena cava syndrome, spinal cord compression) Metabolic - hypercalcemia, SIADH, tumor lysis syndrome Infiltrative - Cardiac tamponade Complications of Cancer Cancer cachexia - Wasting syndrome (↑ morbidity risk) Anorexia, unintended weight loss and appetite Tissue wasting, skeletal muscle atrophy, immune dysfunction Cannot be reversed nutritionally Best management is to treat cancer; ↑nutrition intake; Megace may help Infection - a primary cause of death in pt with cancer Instruct - call HCP if temp is 100.4 F or higher Dysgeusia - altered taste sensation Encourage experimenting with different foods and spices
Right Side - Deoxygenated blood Cardiac Basics Superior/Inferior Vena Cava (from body) Superior Vena Cava Right Atrium Tricuspid Valve Right Ventricle Pulmonary Valve Pulmonary Artery Pulmonary Veins Left Atrium Mitral Valve Left Ventricle Aortic Valve Aorta Inferior Vena Cava Pulmonary Veins To body Flow of Blood through the heart
Right Atrium Tricuspid Valve Right Ventricle Pulmonary Valve Pulmonary Artery (to lungs) Left Side - Oxygenated blood Pulmonary Veins (from lungs) Left Atrium Mitral Valve Left Ventricle Aortic Valve Aorta (supplies body)
Heart Sounds S 1 Closing of the atrioventricular valves; high-pitched, use diaphragm. S 2 Closing of the semilunar valves; high-pitched, use diaphragm. S 3 Heart may be in fluid overload or failure; low-pitched, use bell. S 4 Ventricle resistance; low-pitched, use bell.
NORMAL
NORMAL
MAY BE ABNORMAL
ABNORMAL
Murmurs May indicate wall defect or valve problem; low-pitched, use bell.^ MAY BE ABNORMAL To lungs^ To lungs
Cardiac Biomarkers Cardiac Terms Volume of blood in the ventricles at end of diastole The resistance the left ventricle must overcome during systole afterload= cardiac workload Protein released into the bloodstream when the heart muscle is damaged. BEST INDICATOR OF ACUTE MI! Cardiac Troponin: (cTnT) Creatine Kinase: (CK-MB) Enzyme released into the bloodstream when heart, brain or skeletal muscle damaged. Brain Natriuretic Peptide (BNP): Peptide released into the bloodstream when ventricles fill with too much fluid and STRETCH. Myoglobin: (MB) Found in heart and skeletal muscles; released into bloodstream with MI or severe muscle damage. Not a specific indicator of MI, but good to rule out. Preload: Afterload: Stroke Volume: The amount of blood pumped out of the ventricles with each beat Cardiac Output: The amount of blood the heart pumps in 1 minute (in liters) (Normal = 4-8L/min) Ejection Fraction: Volume of blood expelled with every contraction CO = HR X SV 0-0.4 ng/mL
1.5 = critical 0-5 ng/mL <100 pg/mL 5-70 ng/mL Cardiac Index: (CI) 2.5 -4.0 L/min/m Cardiac Output adjusted for body surface area. More accurate measure of cardiac function. Central Venous
Pressure (CVP): 2 - 8 mmHg Measures right ventricular preload. Indicates fluid volume status. Mean Arterial Pressure (MAP): 70 - 100 mmHg Average arterial pressure. Indicates perfusion of organs and tissues. Normal = 60-100 ml/beat Normal = 50-70% Pulmonary Artery Wedge Pressure: (PAWP) 6-12 mmHg Measures left ventricular preload. Indicates left-sided heart function. Normal Cardiac Basics
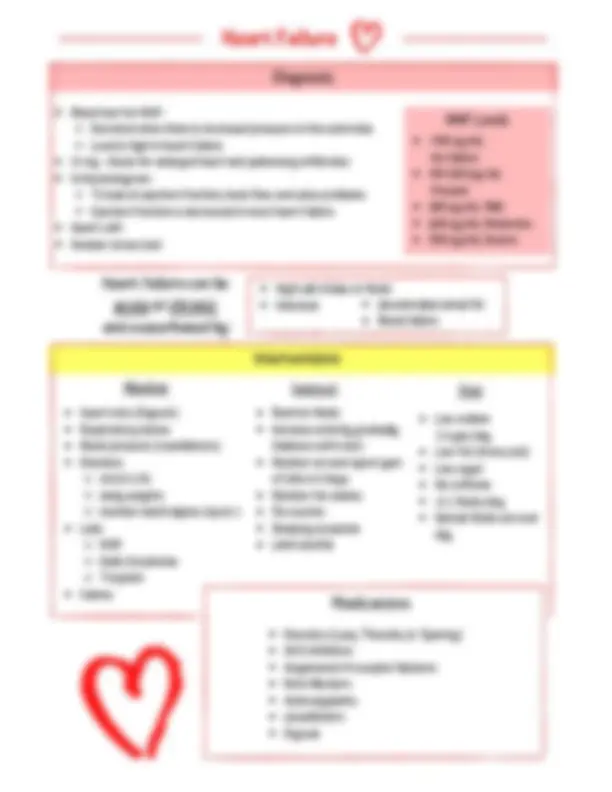
Diagnosis Interventions Blood test for BNP- Secreted when there is increased pressure in the ventricles Level is high in heart failure X-ray - check for enlarged heart and pulmonary infiltrates Echocardiogram - To look at ejection fraction, back flow and valve problems Ejection fraction is decreased in most heart failure Heart cath Nuclear stress test Restrict fluids Increase activity gradually (balance with rest) Monitor wt and report gain of 3 lbs in 2 days Monitor for edema Flu vaccine Smoking cessation Limit alcohol Medications Instruct Diet Low sodium 2-3 gm/day Low fat (trans/sat) Low sugar No caffeine <2 L fluids/day Spread fluids out over day Diuretics (Loop, Thiazide, K+ Sparing) ACE inhibitors Angiotensin II receptor blockers Beta Blockers Anticoagulants Vasodilators Digoxin BNP Levels <100 pg/mL No failure 100-300 pg/mL Present 300 pg/mL Mild 600 pg/mL Moderate 900 pg/mL Severe Heart failure can be acute or chronic and exacerbated by: High salt intake or fluids Infection Uncontrolled atrial fib Renal failure Monitor Heart rate (Digoxin) Respiratory status Blood pressure (vasodilators) Diuretics strict I/Os daily weights monitor electrolytes (esp K+) Labs: BNP BUN/Creatinine Troponin Edema Heart Failure
Risk Factors Atherosclerosis with blood clot Atherosclerosis (Plaque buildup) Normal coronary artery Coronary Artery Disease Build up of fatty plaques due to atherosclerosis in the coronary artery. Can lead to restriction of blood flow to the heart and heart damage or death. Age Gender Men > 45 yrs Women > 55 yrs Race (African American) Family history Diabetes HTN (>140/90) High LDL cholesterol Smoking Sedentary lifestyle Obesity Metabolic syndrome High stress Unhealthy diet Sleep apnea High hs-CRP levels (high- sensitivity C-reactive protein) High TG levels High homocysteine levels Preeclampsia Heavy alcohol use Autoimmune diseases Not Modifiable Modifiable Possible Factors Coronary Arteries Posterior descending artery Left anterior descending artery Left coronary artery Right coronary artery Right marginal artery Left circumflex artery
Chest pain caused by reduced blood flow to the heart. Three types: Stable, Unstable and Variant Stable Unstable Variant Predictable Occurs with exertion or stress Short duration Symptoms relieved by rest or nitroglycerin ** Most common ** Unpredictable Occurs at rest, exertion or stress Symptoms unrelieved by rest or meds ** Most dangerous ** Pain at rest Caused by spasm in coronary artery Reversible ST elevation ** Rare ** Causes Atherosclerosis Coronary artery spasm Thrombosis Heart failure Valve disorders Aortic stenosis **Atherosclerosis Main Cause ** Risk Factors Obesity Sedentary lifestyle Smoking Poor DB management High cholesterol/TG High BP Family history Age Men > 45 yrs Women >55 yrs Emotional stress Weather extremes Heavy meals Atherosclerosis (Plaque buildup) Angina Pectoris
Signs and Symptoms Chest pain that may radiate to jaw, neck, shoulders, back Pressure Squeezing Burning Fullness Interventions BP control Smoking cessation Diet modification Control DB Exercise Flu vaccine Decrease cholesterol levels Medications Surgery Instruct PCI: stent in artery OR CABG: reroute around artery Diagnosis EKG Stress test Echocardiogram Coronary angiography Chest x-ray Blood tests (troponin, lipids) Cardiac catherization Cardiac MRI
SOB
Diaphoresis Weakness/fatigue Pallor Dizziness Nausea/vomiting Feeling of gas, indigestion Women: Nausea SOB Abdominal pain Discomfort in neck, jaw, back (if necessary) Diet Low fat Cholesterol <200 mg/day Adequate fiber Monitor sodium Add in healthy fat (omega-3) Encourage fruits, vegetables and whole grains Angina Pectoris Immediate relief: Nitroglycerin to dilate heart arteries Store pills out of light Patch for unstable Ca channel blockers Beta Blockers Antiplatelet/Anticoagulant Statins
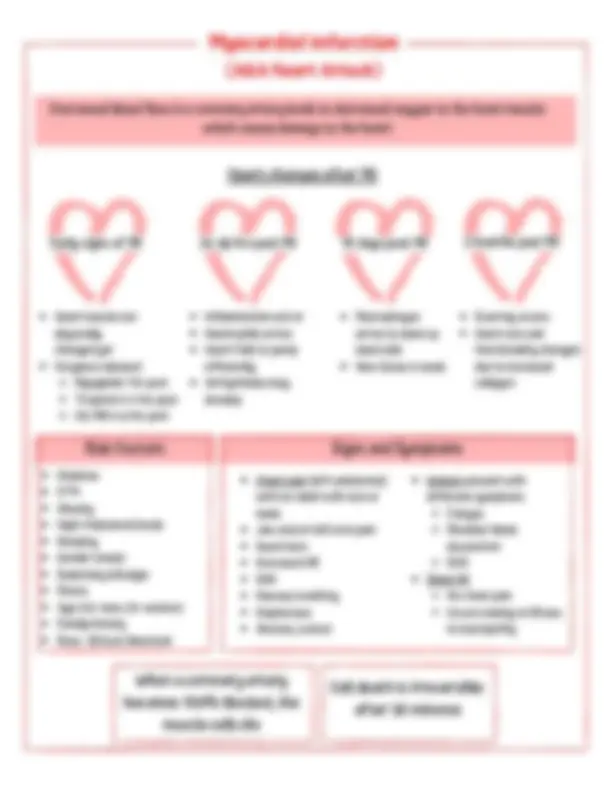
ST Elevation (STEMI) Full blockage (No O2) Normal EKG ST Depression Partial Blockage (Low O2) Diagnosis EKG ST elevation - full blockage (no O2), worst type of MI b/c most damage ST depression - partial blockage (low O2) Blood tests: Troponin, CK-MB, myoglobin Echocardiogram - to check for damage Heart cath - to check for blockages and muscle damage Stress test Interventions 12-lead EKG Monitor BP/HR Oxygen Bed rest Collect enzymes Administer meds Monitor lungs for 'crackles' Instruct Low salt and fluid Decrease stress, alcohol, caffeine Smoking cessation Increase exercise Weigh daily Medications Antiplatelets Morphine Beta Blockers ACE Inhibitors Immediate Nitrates ARBs Statins Calcium channel blockers Anti-thrombotic agents Surgery If necessary PCI or CABG Potential Complications of MI Cardiogenic shock Dysrhythmias Heart failure Cardiac tamponade Myocardial Infarction (AKA Heart Attack)
Causes IV fluids (hypertonic NaCl, excessive isotonic NaCl) Hypertonic tube feeding w/o water supplements Near-drowning in salt water Unconscious/cognitively impaired (unable to detect thirst) High fever, heat stroke (dehydration) Diarrhea Diabetes Insipidus Cushing syndrome Hyperglycemia due to uncontrolled DM Primary hyperaldosteronism Hypernatremia >145 mEq/L Signs/Symptoms Restlessness Agitation Intense thirst Flushed skin Management If water deficit, replace fluid orally or IV (isotonic 0.9% NaCl slowly) Restrict sodium intake Diuretics if water excess Seizure precautions if altered mental state Monitor serum Na+ levels Dry swollen tongue Increased reflexes Seizures, coma ↑BP Causes ↓ ECF volume Diarrhea/vomiting NG suction Diuretics Adrenal insufficiency Burns, wound drainage Fasting/NPO ↑ ECF volume Excessive hypotonic IV fluids Primary polydipsia SIADH Heart failure Primary hypoaldosteronism Sodium (Na+) Major cation in ECF (Extracellular Fluid) Roles: Generation and transmission of nerve impulses Muscle contractility Regulation of acid-base balance Blood pressure maintenance Helps regulate amount of water in and out of cell - Wherever sodium goes, so does water Inverse to Potassium Hyponatremia < 135 mEq/L Normal: 135 - 145 mEq/L Signs/Symptoms If due to↓ ECF volume Irritability Apprehension/confusion Dizziness Tremors/seizures/coma Dry mucous membranes Thready pulse Cold, clammy skin If due to ↑ ECF volume Headache Apathy Confusion Muscle spasms Seizures/coma N/V/Diarrhea Ab cramps Management If due to↓ ECF volume Replace fluid using isotonic sodium- containing solutions Encourage oral Na+ intake Withhold all diuretics If due to ↑ ECF volume Fluid restriction Loop diuretics and demeclocycline IV 3% NaCl (low rate) ADH antagonists for heart failure or SIADH Soups, canned foods Ham, bacon, sausage Most processed foods Cheese, dressings Pizza, hot dogs Cold cuts High Sodium Foods Electrolyte Imbalances