Download NUTRITION LECTURE MIDTERMS and more Lecture notes Nursing in PDF only on Docsity!
GLOBAL PROBLEMS OF NUTRITION
MALNUTRITION
refers to deficiencies, excesses, or imbalances in a person’s intake of energy and/or nutrients. Malnutrition , in all its forms, includes undernutrition (wasting, stunting, underweight), inadequate vitamins or minerals, overweight, obesity, and resulting diet-related noncommunicable diseases. VARIOUS FORMS OF MALNUTRITION I. FORMS OF MALNUTRITION IN DEFICIENCY OR UNDERNUTRITION UNDERNUTRITION There are 4 broad sub-forms of undernutrition: wasting, stunting, underweight, and deficiencies in vitamins and minerals. Undernutrition makes children in particular much more vulnerable to disease and death. Low weight-for-height is known as wasting Low height-for-age is known as stunting Children with low weight-for-age are known as underweight. PEM (Protein- Energy Malnutrition)
- Undernourished children can suffer from PEM when there is: rapid growth, infection or disease w/c increases the need for protein and essential nutrients. **TWO DIFFERENT FORMS OF PEM
- MARASMUS** – named also as the “drying away”
- this is a chronic PEM wherein it reflects a severe deprivation of food over a long time
- There is severe wasting or the patient is emaciated
- it occurs in children from 6-18 mons of age in all over-populated urban slums.
- marasmic children looks like a little old people – just skin and bones.
- Skin is dry and wrinkled
- Hair is thin and dry, easily pulled
- Spoon-shaped brittle nails 2. KWASHIORKOR
- reflects a sudden and recent deprivation of food
- this is classified as Acute PEM
- it sets in between 18 mons to 2 years
- distinctive feature “moon face”
- this is commonly precipitated by an illness such as measles or dysentery (infxn of the digestive tract result to diarrhea
- The child has bulging belly w/ a fatty liver
- With edema on face and limbs **CLASSIFICATION OF NUTRIENT DEFICIENCY/UNDERNUTRITION
- PRIMARY –** caused by inadequate dietary intake E.g. poverty Poor food habit Limited food supply due to over population 2.SECONDARY – caused by a disease condition that may cause mal- absorption(steatorrhea), accelerated excretion or destruction of nutrients **II. FORM OF MALNUTRITION IN EXCESS/OVERNUTRITION
- OBESITY** – generally, it is defined as an excessive amount of fat stored ( as adipose tissue) in the body
- the actual body weight is 20% above the DBW. -will result to many health problems suc as Htn, DM, CAD, CVD, atherosclerosis and even CA CAUSES:
- Genetics – accdg to research that a considerable proportion of human obesity (50-79 %) has a genetic component.
- Sedentary lifestyles – low expenditures
- Abnormal absorption of nutrients
- Over-eating / binge eating disorder. **TYPES OF OBESITY
- UPPER BODY OBESITY** – referred to as central, abdominal/male obesity
- apple-shaped people/Android obesity 2. LOWER BODY OBESITY – known as peripheral, gluteal, femoral/ female obesity Pear-shaped people/ Gynoid obesity
THERAPEUTIC DIETS
PHENYLKETUNURIA Diet(PKU)
- Purpose is to control intake of phenylalanine, an amino acid that cannot be metabolized
- Diet will be prescribed until age 6 or longer to prevent brain damage and mental retardation
- Avoid: breads, meats, fish, poultry, cheeses, legumes, nuts and eggs
- Give lofenalac formula as ordered
- Teach client the family to use low-protein flour for baking
- Sugar substitutes such as Nutrasweet (contain phenylalanine), must not be used. Use the brand sweet ‘n’ low, w/ saccharin ● Clients w/ Peptic Ulcers, Diverticulitis, IBD, Gastritis BLAND DIET – low fiber, roughage - promotes healing of the gastric mucosa
- Chemically and mechanically non stimulating
- For patients w/ gastritis, peptic ulcer
- Given in small, frequent feedings to assist in diluting or neutralizing stomach acid protein foods are good at neutralizing acid) Foods not Allowed:- Spices such as pepper and chili are eliminated.
- A soft diet w/o spices
- Fried, commercially prepared, strong tea, alcohol LOW-RESIDUE DIET – consists of food items that minimize elimination patters by reducing fecal volume
- 5- 10mg of dietary fiber is intended to reduce the normal work of the intestines
- Residue is the indigestible material left in digestive tract after food has been digested.
- it is not the same as fiber
- high fiber foods are high in residue
- other foods such as milk and milk products also leave a residue-increases stool volume and prunes acts as laxative Indication: a. following a colon, rectal or pereneal surgery to reduce pressure on the operative site b. Prior to examination of the lower bowel to enhance visualization(proctosigmoidoscopy)
c. Internal radiation for cancer of the cervix d. Crohn’s disease e. Diarrhea to rest the bowel f. Diverticulitis g. Ulcerative colitis- Foods not Allowed : High fiber foods: fruits and veg Milk and milk products whole grain breads and cereals Foods Allowed: a. Clear liquids a. Sugar, salt b. Meats, eggs c. Limited amounts of milk d. Refined cereals e. White breads f. Peeled white potatoes HIGH-RESIDUE DIET- for patients w/ constipation, hemorrhoids Foods allowed - fresh fruits and veg
- Whole grain products GLUTEN-FREE DIET– purpose is to eliminate gluten ( a protein ) from the diet Indicated in malabsorption syndromes such as sprue or celiac disease Eliminate all products that contain identified grain sources- barley, rye, oats wheat, and malt Avoid: cream sauces, breaded foods. Cakes, breads and muffins
- Allow: corn, rice and soy flour
- Teach client to read the labels of prepared foods.
● Clients w/ Diabetes, Overweight, Obese, w/ HTN,
Atherosclerosis and other Cardiac Problems
- Low Calorie Diets
- A low calorie diet is an allowance of food and drink with an energy value below that required for maintenance in order to bring about weight reduction.
- With moderate calorie restriction, a wise choice of foods can make the diet adequate in minerals and vitamins. However, very low calorie diets, 1200 kcal or less, require vitamin and mineral supplementation.
Note: When other medical conditions such as renal complications are present, further modifications of the diet are required. Distribution of Calories – protein – 12-20% Carbohydrates – 55-60% Fats – 20-30%;fats shld be unsaturated b. Glycemic Index- it refers to how fast and how much the food raises the blood sugar level
- Persons w/ diabetes should eat foods w/ moderate to low glycemic index foods - Client w/ cirrhosis, Pancreatitis, Hepatitis, Pancreatitis, Cholelithiasis
- Low Fat Diets
- A fat restricted diet is an allowance of food and drink in which fat provides no more than 15% of total calories.
- Since the absorption of fat-soluble vitamins is impaired when fat intake is low, supplementation of the diet with these vitamins, especially Vitamin A, is desirable. Indication for Use
- Cholecystitis, cholelithiasis
- Atherosclerosis
- Portal cirrhosis, hepatitis
- Pancreatitis, sprue -Celiac disease, or celiac sprue, is a chronic disorder of the small intestine caused by sensitivity to gluten, a protein found in wheat and rye and, to a lesser extent, in oats and barley.It causes poor absorption by the intestine of fat, protein, carbohydrates, iron, water, and vitamins A, D, E, and K.
- Fat malabsoprtion
- Weight reduction
- Low Carbohydrate Diets
- A carbohydrate restricted diet is an allowance of food and drink in which carbohydrates provide no more than 50% of total calories. Complex carbohydrates are preferred.
- Restricted carbohydrate diets are higher in fat and protein than the normal or regular diet.
- Non-fat milk and low fat meat exchanges are used in order to limit cholesterol to about 300 mg. Cholesterol levels may be further reduced by using fish and chicken without skin and fish more often than meats, and limiting eggs to three to four week.
- A polyunsaturated to saturated fat ratio (P/S) of approximately 1:1 can be obtained by using an appropriate mixture of corn oil and coconut oil
- If higher calorie levels are desired, monounsaturated fats like olive, peanut and sesame oil may be used to provide extra calories.
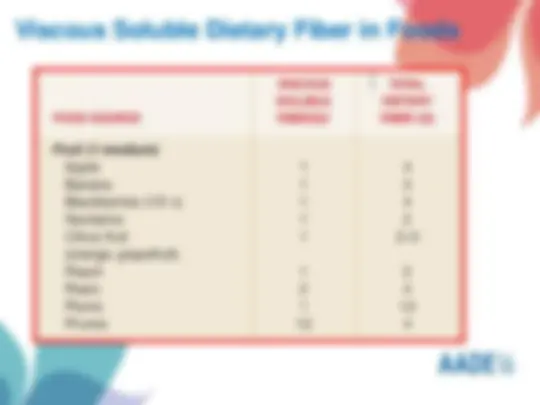
- High Fiber Diet /High Roughage diet- to increase bulk in the stool Indication: - 30gms of dietary fiber would help prevent constipation, diverticulitis, hemorrhoids and colon cancer
● CLIENTS W/ RENAL PROBLEMS
1. Sodium Restricted Diets - To lower body water and promote excretion - These diets have varying levels of sodium that are lower than the usual sodium content of the regular diet which is approximately 2800 to 6000 mg or the equivalent of 7 to 15 grams of sodium chloride. The sodium in the regular diet comes mainly from table salt, although appreciable amount may come from the natural sodium content of foods. Thus sodium restricted diets limit the use, not only of table salt, but also of foods naturally high in sodium. - The diet follows the daily food plan of the regular diet, but the foods allowed are those low in sodium. No salt is used in the preparation and service of meals. - Restriction range from mild(3,000-4,000mg/day) to severe(500mg/day) Indication For Use Condition of sodium or saline excess as in: Congestive heart failure with edema or hypertension Liver disease with ascites Glomerulonephritis Nephrotic syndrome Acute and chronic renal failure PIH and HTN 2. Low Potassium Diet - This is a diet in which the potassium content is reduced to about 1.0 to 1. grams (25-46 mEq) per day. The usual diet contains about 2 to 6 grams (51. to 153.6 mEq) daily, coming mainly from vegetables, cereals, fruits, meat, fish and poultry. The low potassium diet therefore, contains prescribed amounts of selected foods from of supplements. - The diet should be used for limited periods as a supplement to medical therapy. 3. Low Protein Diet - This diet provides about 30 grams of protein per day. Sufficient calories are provided for the maximum utilization of the limited dietary protein and to prevent or minimize tissue breakdown. This is achieved with liberal use of carbohydrates and fat. - Cereals, beans and nuts are used in limited amounts as these contain significant levels of low biologic value proteins. The diet is low in B-vitamins and iron. Indication for Use Acute glomerulonephritis with impaired function
9. Chronic Renal Failure - The diet here is called Renal diet - The diet for chronic renal failure (CRF) is designed to meet nutritional requirements, minimize uremic complications, maintain acceptable blood chemistries, blood pressure and fluid status in patients with impaired renal function, and at the same time, to promote well-being. - Generally, the diet has controlled amounts of protein, potassium, sodium, phosphorus, and fluids. Additional modifications of fat, cholesterol, triglycerides, and fiber may be necessary depending on individual requirements. - The diet is used for patients with CRF requiring hemodialysis or peritoneal dialysis treatments. 10. Acute Renal Failure - The diet for acute renal failure (ARF) aims to reduce the accumulation of the uremic toxins, control electrolyte abnormalities, and correct fluid retention while maintaining nutritional status. Dietary factors need to be controlled include protein, sodium, potassium, phosphorus , and fluid with adequate calories depending on individual needs and the frequency of dialysis treatment. 11. Nephrotic Syndrome - The protein-and sodium-controlled diet for nephrotic syndrome (NS) is designed to minimize edema and proteinuria, control hypertension of renal disease, prevent muscle catabolism and protein malnutrition, and supply adequate energy. - The diet is for persons with NS who are not being dialyzed. 12. Urolithiasis (Kidney Stones) - The dietary modifications for urolithiasis are designed to minimize the supersaturation of components in the urine associated with the formation of renal calculi. Generally, dietary intervention includes combining the restriction of a specific dietary constituent associated with the formation of the stone with a generous fluid intake. Most calculi contain variable amounts of calcium, cystine or uric acid surrounded by calcium oxalate. Indication for Use
- Diet modifications may be used with medical treatment to decrease the predominant components in urine that cause stone formation. Dietary Treatment for Clients w/ diff Renal Stones a. Calcium Oxalate Stones – about 80% of the renal stones formed contain calcium oxalate. -formation of this kind of renal stone is caused primarily by a diet high in oxalate, like, beets, wheat bran, chocolate, tea, rhubarb, strawberries and spinach,and beer(high in oxalate but may have limited bioavailability and thus may be less problematic Deficiency in pyridoxine, thiamine and magnesium contribute to the formation of oxalate stones.
b. Uric Acid Stones – Purine-rich foods are restricted in here Purines are the end products of nucleoprotein metabolism and are found in all meats, fish, poultry. Organ meats, anchovies, sardines, meat extracts and broths. -Uric acid stones are usually associated w/ Gout, GI disease that cause diarrhea and malignant diseases. c. Cystine Stones – Cystine is an amino acid. Formation of this stone is due to high concentration of cysteine in the urine secondary to some hereditary metabolic disorder
- Recommendation is to increase fluid intake and an alkaline-ash diet(to retard the growth of renal calculi) d. Struvite Stones – this is composed of magnesium ammonium sulphate
- This is being called as infection stones bec they develop following a UTI
- A low phosphorus diet is often prescribed. Indications for Use Conditions characterized by elevated blood glucose levels such as diabetes mellitus (insulin dependent and non-insulin dependent), impaired glucose tolerance and gestational diabetes. Note: When other medical conditions such as renal complications are present, further modifications of the diet are required.
● Client w/ Infection, Fever, Underweight/PEM,
Hyperthyroidism, BURNS
- High Calorie Diets
- A high calorie diet is an allowance of food and drink with an energy value of 50 to 100 percent above that required for maintenance.
- Its aim is to produce a gain in body weight, to meet increased energy needs, or to prevent or minimize the catabolism of tissues. Indication for Use
- Underweight
- Hypercatabolic conditions: hyperthyroidism, injury, burns, fever and infections when a full diet can be tolerated.
- High Protein Diets
- To re-establish anabolism and raise albumin levels in burns, infections, hyperthyroidism
- A high protein diet is allowance of food and drink which provides 1.5 grams of protein or more per kilogram of body weight per day or where the protein is increased by 50 to 100 percent above the normal allowance.
- Its aim is to meet increased protein needs or replace proteins lost from the body (see Indication for Use).
▪ -Impairment in upper GI tract leading to digestion, transport and absorption problems ● Alteration in intake pattern due to client’s inability to eat, refusal to eat, or inability to ingest sufficient intake to meet nutritional goals ▪ -functional GI tract ▪ -for stroke/CVA patients, severe malnutrion or extensive burns, IBDs, Pancreatitis(mild), Parkinson’s disease, Dementia, Cancer, Anorexia Nervosa, Severe depression Formulas to be use: Polymeric Formulas(1-2 cal/ml)-containing intact CHON, CHO and fats that require digestion
- Elemental/Hydrolyzed Formulas – (1.0cal/ml)-contain the products of digestion of CHON, CHO and fats and are lactose-free
- Modular Formulas(3. 8-4.0cal/ml)- for client having an extensive wound-healing needs Parenteral Nutrition – nutrition provided via a vein/intravenously
- it is used if the GI tract is not functional or if normal feeding is not adequate for the client’s needs TPN /hyperalimentation is used to provide total nutrition.Catheter is inserted into the subclavian vein/super vena cava.(this is used bec the high blood flow facilitates quick dilution of the highly concentrated TPN, thus reducing phlebitis and thrombosis Weaning -TPN-tube feeding-oral feeding.
- They can be administered via a central vein or for a period of 2wks/less is at peripheral vein. Monitor client for infection on the site and enters bloodstream causing sepsis(infxn of the blood) Formula: a dextrose- amino acid-fat solution Indication: Clinical disease states such as malabsorption, surgical interventions, trauma/stress and or related pathology of GI tract/oncologic condition.
- Malnourished clients who require long-term nutritional support and high nutrient requirements based on clinical deficiencies and for Non- functional GI tract.
- Massive small bowel resection/GI surgery, Intestinal Obstruction, Trauma to the abdomen, head/neck, Chemotherapy, radiation therapy and bone marrow transplantation, IBD(exacerbation),Severe diarrhea, Moderate-severe pancreatitis FOODS THAT CAUSE GAS
- Cabbage, cauliflower, turnips, broccoli
- Dried peas, lentils,turnips,melons,cucumbers
- Peppers, asparagus, pickles,carbonated beverages
- Beer, chewing gum, alcohol and some fried foods FOODS THAT MAY CONTRIBUTE TO DIARRHEA
- Prune juice, apple juice, coffee, coconut
- Highly seasoned /fried foods, high sugar foods, alcohol,
- broccoli, cabbage, cauliflower and popcorn FOODS THAT PRODUCE ODOR
- Dried peas, beans, lentils, fish, garlic, onions
- Asparagus, turnips, eggs and some spices, strong cheeses,
- Medication and vitamin preparation FOODS THAT CONTROL ODOR
- Fresh parsley, yogurt and buttermilk FOODS THAT MAY HELP CONTROL DIARRHEA
- Banana, smooth peanut butter, soda crackers, potatoes
- Oatmeal, oat bran, cheese, yogurt and boiled rice/barley/pasta
Parenteral and Enteral Nutrition
PARENTERAL NUTRITION
Feeding intravenously, bypassing the usual process of eating and digestion.
Feeding through the central vein
Feeding through peripheral veins.
ENTERAL NUTRITION
Liquid supplemental nutrition is either taken by mouth or is given via a feeding tube.
Nasal or oral feeding tube terminates at, either:
Stomach (Nasogastric)
Duodenum (Nasoduodenal)
Jejunum (Nasojejunal)
Feeding tube that leads though an artificial external opening into the stomach (Gastrostomy)
Feeding tube that leads though an artificial external intestine (Jejunostomy) opening into the
small
INDICATIONS:
▶ A person on enteral feeds usually has a condition or injury that prevents eating a regular
diet by mouth, but their GI tract is still able to function or problems with eating or digestion, to
provide nutrition with artificial food, which is specially formulated to provide the right balance
of fats, proteins, sugars, vitamins and minerals.
Three Methods of Nutrient Delivery
1. ENTERAL NUTRITION BY MOUTH
►This form of nutrition support is used for patients who are unable to eat enough food
▸ Nutritional products can be eaten or drunk in addition to any food or drink that the patients
may be able to manage.
2. ENTERAL NUTRITION THROUGH A TUBE
> Enteral nutrition delivered into the gut by a tube is used where nutrition cannot be taken
normally by mouth, but the gut is otherwise working.
TYPES OF ENTERAL NUTRITION
► There are several methods for supplying enteral nutrition to the GI tract. These methods
include:
► 1. Nasogastric (NG) tube: a tube inserted down into the nose until it reaches the stomach.
►2. Nasoduodenal (ND) tube: a tube inserted down into the nose until it reaches the
duodenum (first part of the small intestine).
3. Nasojejunal (NJ) tube: a tube inserted down into the nose until it reaches the jejunum (the
second part of the small intestine).
►4. Percutaneous endoscopic gastrostomy (PEG) tube: a tube surgically inserted through the
abdominal wall and into the stomach,
Mary Ann Hodorowicz RDN, MBA, CDE, CEC (Certified Endocrinology Coder)
Mary Ann Hodorowicz, RN, MBA, CDE, CEC, is a licensed
registered dietitian and certified diabetes educator and earned
her MBA with a focus on marketing. She is also a certified
endocrinology coder and owns a private practice specializing in
corporate clients in Palos Heights, IL. She is a consultant,
professional speaker, trainer, and author for the health, food,
and pharmaceutical industries in nutrition, wellness, diabetes,
and Medicare and private insurance reimbursement. Her clients
include healthcare entities, professional membership
associations, pharmacies, medical CEU education/training firms,
government agencies, food and pharmaceutical companies,
academia, and employer groups. She serves on the Board of
Directors of the American Association of Diabetes Educators.
Mary Ann Hodorowicz Consulting, LLC
www.maryannhodorowicz.com Twitter: @mahodorowicz
Disclosure to Participants
- Notice of Requirements For Successful Completion
- Please refer to learning goals and objectives
- Learners must attend the full activity and complete the evaluation
in order to claim continuing education credit/hours
- Conflicts of Interest and Financial Relationships Disclosures:
- Mary Ann Hodorowicz has no conflicts of interest or financial
disclosures to disclose.
- Sponsorship / Commercial Support:
- Non-Endorsement of Products:
- Accredited status does not imply endorsement by AADE, ANCC,
ACPE or CDR of any commercial products displayed in
conjunction with this educational activity.
- Off-Label Use:
- Mary Ann Hodorowicz will not discuss any off-label use of OTC or
prescription drugs.