Download OPHTHALMOLOGY and more Exercises Ophthalmology in PDF only on Docsity!
THE BRITISH JOURNAL
OF
OPHTHALMOLOGY
JULY, 1918
COMMUNICATIONS
DISTURBANCES OF VISION BY CEREBRAL
LESIONS*
BY
GORDON HOLMES, C.M.G., M.D., Lieut.-Col. R.A.M.C.
ABOUT 18 months ago I was able to present to this Section with
my colleague, Colonel Lister, certain clinical observations on the
disturbances of vision produced by gunshot injuries of the visual
cortex and of the optic radiations. From these we drew certain
conclusions on the cortical representation of the retina, and
particularly on the segmental (^) correspondence of different areas of
the retina with separate zones of the visual cortex. Our chief
conclusions were:
1. The upper half of each retina is represented in the dorsal, and
the lower in the ventral part of each visual area.
2. The centre for macular or central vision lies in the posterior
extremities of the visual areas, probably in the margins and the
lateral surfaces of the occipital (^) poles. The macular (^) region has not
a bilateral representation.
3. The centre for vision subserved by the periphery of the retinae
is probably situated in^ the anterior ends^ of^ the^ visual^ areas, and the
serial concentric zones of the retina from^ the^ macula to^ the periphery
'Read in the Section of Ophthalmology of the Royal Society of Medicine, December
354 THE BRITISH JOURNAL OF OPHTHALMOLOGY
are probably represented in this order from behind forwards in the
visual cortex.
These conclusions agree with those that were^ previously^ arrived
at by Inouye from his observations on gunshot injuries^ of the
occipital lobes inflicted in the Russo-Japanese War,^ and^ they
conform with Marie and Chatelin's valuable investigations^ on men
with wounds similar^ to those of our^ patients.^ They^ have later
received support from various observers,^ and^ especially^ from Captain
Riddoch.
Since our last communication I have had the^ opportunity^ of
examining a large number of cases in which various defects or
disturbances of vision were produced by local cerebral injuries.
Every further individual^ observation^ has been in^ harmony^ with
these conclusions, and I have not^ met^ with^ a^ single^ clinical fact
that is in any way at variance with them.^ It^ is^ not my^ intention
to place all my later observations before you,^ though^ they^ afford
valuable confirmatory evidence of our contentions, but to^ select
a certain number which will fill up some gaps in our previous
communication.
Local Defects in^ the^ Fields^ of^ Vision
The most interesting and important of^ these are^ the^ central^ and
paracentral scotomata. These are extremely common in^ all super-
ficial and moderate injuries of the occipital lobes. When the^ poles
of both hemispheres are injured central vision may be completely
lost, while^ a^ unilateral^ wound^ produces^ homonymous^ scotomata^ in
the opposite halves of the fields.^ In^ our^ previous^ communication
we recorded several cases with central scotomata; since then^ I^ have
seen very few of these and they have added nothing^ further^ to the
facts we then presented to you. Paracentral scotomata due to
unilateral occipital lesions^ are much^ more^ common,^ and^ especially
those situated in^ the^ lower^ quadrants; so^ many^ of these^ latter
have been already recorded by ourselves,^ by^ Marie^ and^ Chatelin
and by others, that further examples are not^ necessary. One of^ the common types is a pure lateral paracentral scotoma, and^ as^ but^ few
cases with this condition have been described^ I^ may put the
following example forthwith:
CASE 1.-Private R-, 15104, was wounded on September 26, 1916, by a^ shrapnel ball which penetrated his steel helmet. He was unconscious for an hour or^ so, and stated that he was completely blind till the next day. He never noticed any subjective visual phenomena. He was admitted to a Base Hospital on the day following the infliction of the wound. Wound.-There was^ a^ small^ penetrating wound from which softened^ brain^ extruded,
immediately to^ the^ right of^ the^ middle^ line^ of^ the^ skull^ and^1 inch^ (2-5^ cm.)^ above the
inion. A radiograph revealed^ much^ depressed bone,^ but^ no^ foreign body.^ An^ operation
was performed next^ day, and several^ fragments^ of^ bone^ as^ well^ as^ clots^ and^ pulped^ brain
tissue were removed from^ the^ occipital^ pole.^ The^ recovery^ was^ rapid^ and^ uneventful. His visual fields were taken by a^ perimeter and^ a screen^ scotometer^ six^ days^ after^ the
356 THE BRITISH JOURNAL OF OPHTHALMOLOGY
close relation to the depth of the wound. Certain cases of bilateral
inferior scotomata which I have seen deserve, however, mention, as
they afford valuable evidence on the question of cortical localisation.
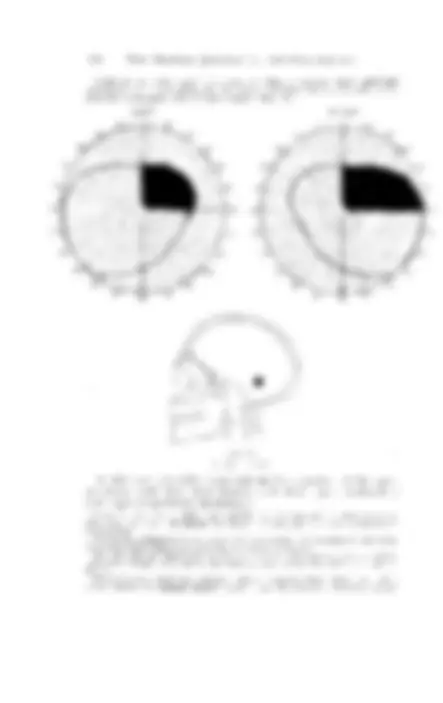
CASE 2.-Private B.-, 1822, was wounded by a rifle bullet which passed through his steel belmet on July 15, 1916. He did not become unconscious, but noticed almost at once " expanding red iings, like the rings you may see when you throw a stone into a pool," in front of his eyes. These remained only a few minutes. Since then he (^) was aware of a considerable disturbance of vision in the (^) right eye; his left eye had (^) been amblyopic and almost useless since^ childhood. He complained of, and showed no other symptoms. The wound was a shallow gutter 2 inches long, which crossed the middle
RI OltT
FIG. 2.
White 5 mm.2 Red and Green 10 mm.i
line and was bisected by it, 1I inches (37 cm.) above the tip of the inion. A radio-
graph revealed a fracture and (^) a slight depression of the skull. When he was examined two (^) weeks after he received the wound his visual disturbances were the only abnormal symptoms he presented. On perimetric examination the peripheries of the fields for white (5mm.2) and colours (10mm.2) were found unrestricted, but by the scotometer a small absolute scotoma for white and colours was (^) detected below the fixation point. It extended into both the right and the left halves of the visual fields to about 2°, and downwards to about 30; it (^) reached exactly to the fixation point (Fig. 2). The borders of this scotoma were remarkably sharp; when a test object was moved from the scotomatous area into the seeing part of (^) the field the patient described it as if " (^) the object suddenly (^) passed from behind a curtain. " (^) The areas blind to white and to colours
were practically identical.
DISTURBANCES OF VISION BY CEREBRAL LESIONS 357
In this case the lesion obviously involved the margins of both
occipital lobes slightly above the level of the calcarine fissures and
produced a^ bilateral inferior scotoma.
CASE 3.-Private L- was wounded on May12, 1917, by a fragment of shell. He was wearing a steel helmet at the time and the missile passed through it. He was
dazed but not^ unconscious.^ He states^ that^ he^ was blind^ for^ five minutes or^ so; since
then was not aware of any disturbance of vision, but he suffered^ much from^ headache
and was in a dull irritable state. The wound was a deep gash 3 inches^ (7 5 cm.)^ long across the middle line, slightly higher on the right side than on the left, which crossed
the middle line Ij inches (3 5 cm.) above the point.of the inion. Stereoscopic X-ray
piates showed a depressed fracture under the wound. He was operated upon on the
LIFT RIOHT
FIG. 3.
White 6 mm. 2
third day; the scalp wound^ was^ excised, a^ flap was^ turned^ down,^ a^ trephine^ opening
made, and a considerable area of^ depressed inner^ table^ was^ removed.^ The dura mater
was lacerated most-extensively on^ the^ right side.
He was at first so dull that his vision could not be properlv examined, but before the
operation he had certainly a large bilateral inferior paracentral scotoma which gradually
diminished in size from below upwards. Sixteen days after the^ infliction of the wound, when he was again bright and intelligent and the^ operation wound^ was^ healed,^ a
perimetric examination revealed only a bilateral inferior^ paracentral scotoma^ which
reached the fixation point and extended 150 to^ 170Q^ in^ every direction.^ His central
vision and the peripheral limits of his visual fields were^ normal^ (Fig. 3).^ He
presented no other signs of cerebral disturbance.
DISTURBANCES OF VISION BY CEREBRAL LESIONS 359
occipital lobes were injured at, or immediately above, the posterior
ends of the calcarine fissures.
These three cases support strongly the conclusions we have
already arrived at, that the upper halves of the retina are represented
in the dorsal parts of the visual areas, and that the macula and the
zones of the retina immediately surrounding it are projected on the
most posterior part of the area striata. It is impossible to estimate
exactly, even when an operation has been performed, the extent or
depth of the injury to the brain in any case of gunshot wound of
the skull; but in many of my patients, as in Case 2, it was probably
small and superficial, and probably did not afiect the mesial
surfaces of the hemispheres. It is, consequently, likely that the
zones of the retina immediately around the macula are represented
in that portion of the area striata which extends on to the lateral
and posterior surfaces of the^ hemispheres.
Superior paracentral scotomata
Isolated superior paracentral scotomata are much less common.
Listerland I^ were^ able^ to^ describe^ only two^ cases^18 months^ ago;
LE FT RS OHT
FIG. 5.
360 THE BRITISH JOURNAL OF OPHTHALMOLOGY
Marie and Chatelin have also described two, and Riddoch one other
case. In all these patients the lesion, as far as could be determined,
involved the lower part of the area striata, and they therefore indicate that the retina immediately below the macula is represented in the lower portion of the calcarine area. The three cases I can
now add to these go to confirm this assumption.
CASE 5.-Private W-, 3262, was wounded by a fragment of shell-casing on October 20, 1916. He did not become unconscious, and was able to walk to the dressing station with a little help. There he found he could not see properly; he was unable to recognize the food placed in front of him, but he did not notice any mist in front of his eyes, or other subjective visual phenomena. The disturbance in vision diminished rapidly during the first few days. He had much headache at first, but this soon disappeared. The wound was a small puncture over the left lateral sinus, one inch (2 5 cmi.) to the left of the middle line. A stereoscopic X-ray examination revealed a defect in the skull over the left lateral sinus, a piece of bone depressed beneath it, and a small fragment of metal under the left parieto-occipital suture, some distance from the middle line. He had also a penetrating septic wound of lhis left knee-joint which nec ssitated amputation through the thigh. There were no local cerebral symptoms apart from hiis visual disturbance. When he was first examined ten days after the infliction of the wound, he was not aware of anv visual defect, and his central vision was 6/6 in each eye. A perimetric examination also showed that the peripheral limits for white and colour vision were normal. A complete scotoma for white, red and green (objects 75 mm2) was, howeever, found in the right upper quadrants; the^ blindness extended to the fixation point and peripheralwards for
about 150. The visual fields were again investigated by a scotometer three weeks after
he received the wound, and then the only difference detected was a slight restriction in the periphery of the scotoma; it still extended up to the fixation point (Fig. 5).
The headache had now disappeared, and he presented no symptoms of an active
cerebral lesion.
The course of the missile in^ this case was such that it^ must^ have
injured the posterior lower and inner portion of the occipital pole,
and consequently it probably involved the lower and posterior part
of the area striata.
CASE 6.-Captain T- was wounded by a fragment of shell-casing on July 1,
- He was not unconscious. After the first few days he complained of no symptoms, and was unaware of^ any visual^ disturbance, but^ about^ three^ weeks^ later began to suffer with increasing headache, and then^ a slight degree of^ optic neuritis developed.
The wound was an oblique gutter, 1J inches (3'8 cm.) long, which extended from
the upper margin of the inion to the right and slightly upwards. A radiograph showed a depressed fracture. This was later operated upon by Captain Burrows, who found an extensive extradural clot. The dura was bruised but not lacerated; it was not incised. He made an uneventful recovery. When his eyes were examined four weeks after the infliction of the wound, he was not (^) conscious of (^) any visual (^) disturbance, but a small absolute paracentral scotoma, which extended from the fixation point to about 40, was found in^ both left upper quadrants. This absolute scotoma reached slightly below the horizontal line, and was here continuous with an area in which vision for small white objects (7 mm2) was very imperfect, and colour vision was lost. The peripheral limits of both white and colour vision were normal in both eyes (Fig. 6).
Here the (^) posterior tip of the right occipital lobe was (^) certainly
contused and compressed by the depressed fracture and extradural
clot, aind from the position of the wound it (^) may be assumed that
362 THE BRITISH JOURNAL OF^ OPHTHALMOLOGY
LEFT. RI GHT.
(^30 30) so~~~~~~~~~~~~~~~~~
I.
V.~~^ ~^ ~~~FG^9 7.
In 0
FIG. 7.
L. and R. 6/6. White 7 mm.2 Red and Green 10 mm.
casualty clearing station soon after the, infliction of the injury, but the note which accompanied him merely stated "decompression over the occipital region; wound closed with a small drainage tube in its centre." He came under observation four weeks later. The wound was represented by a healed horizontal scar, 2 inches^ (5 cm.) in^ length, which was slightly higher on the right than on the^ left^ side, and crossed the^ middle
DISTURBANCES OF VISION BY CEREBRAL LESIONS 363
line J inch (1 cm.) above the inion. A defect in the skull could be felt beneath it on
each side of the middle line. His vision was now 6/6 in each eye, but he had still considerable difficulty in reading. His visual fields were examined by a screen scotometer as well as by a perimeter. The peripheral limits for white, red, and green (test objects 7mm2) were normal, but (^) there was an absolute paracentral scotoma of equal extent for white and colours above the fixation point. This extended to (^) 6° or 7° to the right and left of the fixation point, to 50 above (^) it, and reached exactly to it (Fig. 7). An area of partial blindness to white, and complete to colours, extended from this absolute scotoma below the horizontal line in (^) the right halves of the visual fields.
It was impossible to ascertain the exact degree of the injury in
this case, but the position of the wound and the defect in the skull
indicate that the brain was damaged superficially on both sides of
the middle line, immediately below the posterior ends of the
calcarine fissures.
These cases of superior paracentral scotomata were all associated
with, as far as can be judged from the position of the wound and
from radiographic examination, lesions of the inferior portion of the
occipital pole; in each case the local injury was probably small and
aftected chiefly the cortex, or the cortex and subcortical white
matter, below the level of the calcarine fissure. They are con-
sequently evidence that the inferior halves of the retinae are repre-
sented in^ this area.
It is a striking fact that in the majority of paracentral scotomata
the blindness extends directly up to or to within (^10) or so of the
fixation point, but this is not always so. I have seen cases, and
Marie and Chatelin have recorded others, in which the scotoma was
separated from it by an appreciable zone of vision. The question,
however, arises why the area of central vision is so commonly
affected by these traumatic injuries. Two explanations might be
involved; because the macula is projected on to a (^) part of the visual
cortex which is likely to be damaged by all injuries of the occipital
region; or because macular (^) vision, being very7 (^) highly specialized, has
a (^) relatively much more extensive cortical distribution than has
peripheral, just as the cortical motor areas for the finger and thumb
movements are both absolutely, and relatively to the bulk of the
muscles they innervate, very much larger than that of other (^) parts of the body. Both (^) explanations are (^) probably correct. The evidence
at (^) present available (^) goes to show that (^) the macula is represented at
the occipital poles of the hemispheres, and probably on their posterior
and lateral surfaces, and this is the region which must be involved
by lesions which produce such scotomata as are described here.
Additional evidence that the upper halves of the retina are
represented in the dorsal parts of the visual areas is furnished (^) by a
case of inferior horizontal hemianopia in whom an autopsy was
obtained 7 weeks after the infliction of the wound.
CASE 8.-Sergeant K-, 679270, was wounded by a fragment of shell-casing on July
23, 1917. He was unconscious for some hours and later found his vision much
affected, but he could recognize and distinguish persons.
DISTURBANCES OF VISION BY CEREBRAL LESIONS 365
less distinctly in the remaining (^) portions of this quadrant than to the left of the vertical line. The colour fields were, however, normal in both upper quadrants. He died from other causes seven weeks after his injury. On examination of his brain the entrance wound was found in the middle of the lateral surface of the right occipital lobe some distance behind the (^) level of the parieto-occipital notch. From here the missile (^) passed through the dorsal parts of the optic radiations and emerged on the mesial surface of the hemisphere in the angle between the calcarine and the parieto-occipital fissures. The track of the missile was small and it had produced relatively little softening around it. The missile then entered the mesial surface of the left hemi- sphere in the parieto-occipital fissure, the destruction it produced reaching to 0 5 cm. of the calcarine fissure, passed through the dorsal portion of the optic radiations, and made its exit through the anterior portion of the gyrus angularis. On this side there was a considerable area of destruction, especially under the operation wound.
In this case the blindness in the inferior quadrants was probably
due to destruction of the dorsal portions of the optic radiations, and
the defect in the upper right quadrants to additional damage of the
left optic radiations by the softening under the gyrus angularis; but
the fact that there was no restriction or amblyopia of the left upper
quadrants, despite the presence of a lesion in the dorsal and anterior
part of the right visual area, permits the assumption that no part of
this quadrant *is (^) represented in the (^) dorsal portion of the calcarine
cortex.
Sector scotomata
We have now, I believe, sufficient evidence to conclude that the
upper halves^ of^ the retina are projected on to the dorsal parts of the
visual areas, and the lower halves on to their ventral portions, while
macular and perimacular vision are represented in the most
posterior (^) parts of these areas.
Other problems must be, however, considered, and they can be
most easily studied in cases with paracentral scotomata. It is not
uncommon, for instance, to find sector scotomata, that is isolated
homonymous areas of blindness which are more or less accurately
limited (^) by two radii of the visual fields. Can we then say which
portion of the visual area is injured? Here, again, in the absence
of (^) pathological confirmation, the localization of the lesions can
be only approximate, and until a certain number of suitable
anatomical examinations are available, our conclusions can merelv
have the value of hypotheses, but by the accumulation of clinical
cases these (^) hypotheses can be made more and more (^) probable. As a
rule, these sector scotomata lie between the vertical line through
the fixation point, and one of the oblique radii, or, as in^ Case 1, only
this area may escape. Patches of blindness bounded by the
horizontal line through the fixation point and an adjacent radius are
more uncommon. The following cases can, I believe, throw some
light on this subject:-
CASE 9.-Private G-, 201700, was wounded by a^ shrapnel ball^ on^ August 12, 1917.
He was in^ a drowsy and unconscious state^ for^ two^ days, and^ became^ aware^ that his
sight was affected 'when he reached a Base Hospital on the third day. He then found
366 THE BRITISH JOURNAL OF OPHTHALMOLOGY
that he could not see sufficiently well to (^) read or write, though he was able to recognize large objects in the ward. He had never any subjective visual phenomena. Wound.-There was a circular contused wound just to the right of the middle (^) line with its centre 3 cm. above the point of the inion. Radiographic plates showed a whole spherical shrapnel ball within the (^) brain; it (^) had passed to the left, and slightlv upwards and forwards. and (^) lay about (^) 1-5 cm. to the (^) left of the middle line, about 2 cm. in front of the occipital bone, (^) with its lower border 5 cm. above the inion. Soon after his (^) admission to the (^) Base Hospital an operation was undertaken; some fragments of depressed bone were removed from the mesial surface of the right hemisphere, but on drawing out one which had penetrated the torcula, severe haemorrhage occurred which made plugging necessary, and prevented further operative interference. Uninterrupted recovery took place. His visual fields were first carefully examined five (^) weeks after the infliction of the wound. This^ was^ then^ healed completely; he had no headache or cerebral symptoms, apart from the disturbance of vision of which he himself was scarcely aware. His central vision was 6/9 itn each eye, but perimetric observation revealed in each eye (^) a complete right-sided inferior quadrantic hemianopia extending to 1l' from (^) the fixation point, and a (^) sector-shaped inferior left (^) paracentral scotoma which lay between the
inferior vertical line and the radius at 45Q to it; it came to within 40 of the fixation point.
The colour fields were normal except in the blind areas (Fig. 9).
LE FTY (^) RI OHT.
(^30) ~~~~~~~
(^45 )
75
00~~~~~~~~~~~~~~~~~~~~~
20~~~~~~~~~~~~~~~~~~~~
(^135) -136~~~~~~~~~~~~~~~~~~~
FIG. 9.
White, Red, and Green 7 mm.
In this case the (^) right lower quadrantic hemianopia was obviously
due to the extensive lesion produced by the shrapnel ball in. the
mesial part of the left occipital pole above the level of the calcarine
fissure. As the bullet entered near the middle line and passed obliquely upwards and to the (^) left, the (^) injury to the mesial surface of the (^) right hemisphere was in (^) all probability superficial, and must have affected^ chiefly the^ upper and posterior portion of7the^ visual
area on this side. The visual cortex buried in the calcarine fissure
probably escaped direct injury.
This case consequently suggests that those portions of the retinae
which lie (^) along the (^) superior vertical radii send their afferent
368 THE BRITISH JOURNAL OF OPHTHALMOLOGY
In this case the left-sided paracentral scotoma was evidently due
to the injury to the right occipital pole, while the inferior right
scotoma can be most easily explained by the injury which the
mesial surface of the left occipital lobe must have received from the
fragments of bone which were driven through the falx cerebri.
Their position, which could be accurately localized on the radiograph
plates, corresponded to the upper margin of the trephine opening,
and consequently they probably affected only the most dorsal part
of the visual area.
In this case, as in the preceding one, we also find an irregular
sector scotoma lying between the inferior vertical radius and a
neighbouring one, which was probably produced by a lesion of the
most dorsal zone of the visual area.
CASE 11.-Private H-, (^) 31902, received, on June 14, 1917, a gutter wound from a rifle bullet, which (^) passed beneath his helmet. He was unconscious for a time, and later found that he was quite blind; he never noticed flashes of light or other subjective visual phenomena. He became able to see moving objects on the third day, and his vision improved (^) progressively from this day, especially after the operation. Wound.--There^ was^ an^ apparently superficial gutter wound about 1 inch (2.5 cm.) above his inion, but an X-ray photograph revealed a large depression of the skull on to his occipital poles. An operation was performed, and it was found that (^) the internal occipital protuberance, together with the internal occipital (^) crest and a considerable portion of surrounding (^) bone, was driven into his left occipital lobe, and through the longitudinal sinus and (^) falx cerebri. He made an uninterrupted recovery, but was kept under observation for three months after the infliction of the wound. His vision was first (^) examined six weeks after he received the wound. Then he had an almost complete right-sided hemianopia, in fact he was (^) able to (^) recognize only moving objects indistinctly in the upper margins of these fields. (^) The hemianopia
came exactly to the fixation point. His central vision was only 6/36 in each eye, and
there were large paracentral (^) scotomata extending to about 250 outwards from the fixation point in both the upper (^) and lower quadrants, which did not, however, involve vision (^) along the horizontal radii. His visual fields were repeatedlv taken both with the perimeter (^) and the screen scotometer up to three months after the (^) infliction of the wound. At the latter date there was a considerable return of (^) vision in the periphery of the right halves of the fields; but here he (^) was generally conscious only of the movement of the white test (^) object, and saw it only " (^) as through a mist," and as a "dirty grey colour." Central vision was now 6/18 to 6/24, and there were still (^) paracentral scotomata in the left (^) upper and lower quadrants. In the greater part of the lower the blindness was complete, but between the horizontal radius and that 300 below it he could recognize small white, red, and (^) green test objects, but they did not appear distinct to him. The upper scotoma (^) lay between the upper vertical radius and that at 45° to it; here he had no colour vision, and the appreciation of a white test object 8mm2. was vague and uncertain (Fig. 11). There was no definite loss of (^) peripheral vision to either white or colours in the left visual fields.
In this case there were, in addition to a large right-sided hemianopic
scotoma, areas of complete and partial blindness to the left of the
middle (^) line, which, within 18° to 200 from the fixation point, spared
only the macula and a triangular strip between the horizontal radius
and that which runs upwards at approximately 450 to it.
The right-sided blindness was obviously due to the massive
injury to the pole of the left occipital lobe, while the left-sided
scotomata were (^) probably produced by the contusion and destruction
DISTUIRB3ANCES OF VISION B1Y CEREBRAL LESIONS 369
of the right vistual area by the fragments of bone which penetrated
the falx. Macular visionl (^) escaiped, as^ the most^ posterior^ part of^ the
visual area w-as probably not severely injured.
If we asstume from the two (^) preceding cases that the (^) upper and lower margins of the cortical visual areas receive light (^) impressions fromn those
portions of^ the^ retina^ which^ lie^ along the^ vertical^ radii,^ the^ p)ersistelce of (^) vision in the neighboturhood( of the (^) 1horizontld ra,dii might be ex-
pilained by^ the^ escape of^ that p)rtion of^ the^ VisUal^ cortex^ which^ is
cont(ained in the walls of the c;tlcarine fissuire, since the damage of the
tuesial sulrface of the right (^) occilpital lobe was (^) p)robablv stiperficiall.
LE FT. R^ I^ GHT.
45~~~~~~15~
V--~~~~~~~~5.
ISo 05~~~~~~~~~~~~~~~~
s8\0,-,1-A w-@E~~~~~~~~~~~~~~
'd] d ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~1,
FIG. 1-1. \'hite 8 mm.' iRed 7 mm.' (reen^ /^ mm.' L. 6/18-6/24 andl R. 6/24.
CASE, 12.-LPrivate \V.-, 52786, was wounded on^ September 20, 1917, by a fragment of shell, and is still uinder observation. He^ was^ uniconscious for^ a^ short time, andi on^ regaininig^ consciousness^ found^ he^ xvas^ completelv^ blind.^ He^ soon^ began to see again, but "out of^ my^ left^ eye only"^ he^ noticed^ no^ lights,^ or^ colours,^ or othe- subjective plhenomena, but^ everything he^ cotsld^ see^ seemed^ to^ move.^ He^ ha(d severe headache during the first few days, but^ this^ theis^ subsided^ comiipletely. WVo1und.-There was a small circtilar scalp wound^ juist to^ the right^ of the middle line, and I inch (2.5 cm.) above the inion. Radiographss revealed^ a^ circular^ diefect in the mididle line of the skuill, 1 incs (2 5 ctim.) above the inion, and(l a^ definite^ track .eading from^ this^ forwards,^ slightly^ uipwards^ andi^ to^ the^ left,^ for^ a^ (listanice^ of^ 2?^ inclies (7 cm.) along whsich^ several^ fragnsents of^ depresse(l bsoise^ anici^ metal^ lay^ (Fig,.^ '). His woundl healed rapidly, and all his sysmptoms, e\cept the affectioll of visioll, disappeared quickly. His visual fields were repeatedly examined up to^ elexen wN-eeks after^ the^ ilnfliction of
the woun(d; no appreciable change occuirred dturing tlse^ last^ few^ weeks.^ His^ central
\vision was 6/24. There was a complete and absolute^ right-sided hlemianopia which
came directly tip to the fixation poinit. In^ the^ left^ halves^ of^ his^ fields^ an^ inferior^ sector
scotoma existed between the vertical and the radius^ at^ 15Q^ to^ it, wlhich^ came^ to^ within 1`1 of the fixationi point and the liorizontal radliuis, ai(s a^ smnall^ isolated^ superior para-
central scotoma which reached almost to^ the^ fixation^ point. The^ fields^ for red^ ain(d
DISTURBANCES OF VISION BY CEREBRAL LESIONS 371
When a tracing of a lateral X-ray view of his skull was super-
imposed on a mesial sagittal section of a normal average head, it
was found^ that the missile must have^ passed^ along and^ parallel^ to
the posterior limb of the calcarine fissure, and must have destroyed
both its cortex and its sub-cortical fibres. Owing to the position and
the track of the wound, the injury to the right occipital lobe was
certainly superficial; in all probability it did not involve the cortex
in the walls of the calcarine fissure, and, as it produced an inferior
sector scotoma, vision in^ this part of the field may be probably^ brought
into relation with that portion of the visual area that occupies the
tipper free surface of the calcarine cortex. Further, the (^) only useful vision which the patient had to the
left and^ within^ 10°^ of the fixation^ point,^ was^ on^ either side -of
the horizontal radii; it^ seems^ probable that this was dependent on
the integrity of the more laterally situated cortex which is bulried in
the calcarine fissure.
Though these cases cannot, in the absence of anatomical
examinations, be regarded as conclusive evidence, they tend^ to show
that those portions of the retinae which lie along the vertical radii
are represented on the exposed mesial surfaces of the occipital
lobes, and by exclusion one might assume that the retinae on either
side of the^ horizontal^ radii^ are^ projected on^ to^ the visual^ cortex
which occupies the walls of the^ calcarine fissures.^ I cannot^ pretend
to suggest how much of the retinal representation actually lies on
the exposed mesial surface of the hemisphere; it is probable that
anteriorly at^ least^ the^ proportion^ is^ small.
I have not yet met with a case' of sector scotoma along the
horizontal radius, excepting a^ few^ small paracentral scotomata
which occupied this position; but if^ the hypothesis put forward
here is correct, this is what might be expected, as any missile
which had^ such^ a^ course^ that^ it^ would^ destroy the walls^ and^ floor^ of
the calcarine fissure^ only, must^ injure also the^ afferent fibres^ to^ these
portions of the visual area^ on^ the free^ surface of^ the^ hemisphere, and
consequently produce a hemianopia or large irregular scotoma.
The cortical representation of peripheral vision
In my previous communication with Colonel Lister, we could
only by a process of^ exclusion^ suggest^ that vision in the^ periphery of the fields was represented in^ the^ anterior portions of^ the^ cortical
visual areas. We cannot expect to find many appropriate cases^ to
decide this question definitely, as penetrating or perforating wounds
which could injure the anterior portion of the area striata would
be very liable to involve the optic radiations too, and cause extensive
or irregular areas of blindness.
Riddoch has since then published, a case which is^ of considerable value as (^) positive evidence of the localization of per;ipheral vision.
372 THE BRITISH JOURNAL^ OF^ OPHTHALMOLOGY
In this man, in whom there^ was considerable^ peripheral^ con- traction of^ both^ visual^ fields,^ a rifle^ bullet and, later, fragments^ of
bone, were^ removed^ from^ the^ great^ longitudinal fissure between^ the
two hemispheres,^ at^ such^ a^ level^ and^ depth^ that they^ probably
injured the^ anterior^ portions^ of^ the^ calcarine areas.^ I have^
also
recently seen a^ case^ which bears^ directly^ on^ this^ question.
LEFT. (^) R I (^) GHT.
FIG. 13.
CASE 13.-Private M.-, 3841,^ was^ wounded^ by^ a^ small^ piece^ of^ shell-casing.^ fle
was unconscious for^ a^ time^ and later^ had^ considerable^ headache,^ but^ he^ noticed^
no affection of his sight.
Wound.-There was^ a^ small^ clean^ entrance^ wound^ just behind^ the^ base^ of^ his^
left
mastoid. Radiographs^ showed^ a^ small^ fragment^ of^ shell-casing^ in^ the^ occipital^ region
which had^ just^ crossed^ to^ the^ right^ of^ the^ middle^ line;^ it^ was^ probably^
arrested
immediately it^ had^ passed^ through^ the^ falx.^ When^ a^ lateral^ X-ray photograph^
was
superimposed on^ a^ mesial^ sagittal^ section^ of^ an^ average^ normal^ head,^ the missile^
was located in^ the^ calcarine^ fissure^ immediately^ in^ front of^ the^ parieto-occipital^ fissure
(Fig. 13).
!His visual^ fields^ were^ carefully^ examined^ on^ three^ separate^ occasions up^ to^
three
weeks after the^ date^ he^ received^ the^ wound,^ and^ on^ each occasion^ exactly^ the^
same condition was^ found.^ This^ was^ a^ contraction^ of the^ temporal^ periphery^ of the^ left