



Osteomyelitis
Ilya Maisara
Tan Zhen yang
Supervisor:
Dr Faiq, Mr Ganesha

























Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
A detailed overview of osteomyelitis, covering its anatomy, pathogenesis, types, clinical features, investigation methods, and treatment options. It discusses the anatomy of long bones, focusing on the epiphysis, metaphysis, and diaphysis, and explains the blood supply and common infection sites. The document also outlines different types of osteomyelitis, including acute hematogenous, contiguous-focus, chronic, vertebral, and implant-associated forms. Clinical features, such as symptoms and signs, are described, along with laboratory and imaging investigations like x-rays, ct scans, and mri. Treatment strategies, including conservative and surgical management, are also discussed, along with potential complications. A case study of chronic osteomyelitis of the tibia is presented to illustrate the clinical aspects of the disease. Valuable for medical students and healthcare professionals seeking a comprehensive understanding of osteomyelitis. (498 characters)
Typology: Slides
1 / 35

This page cannot be seen from the preview
Don't miss anything!
Tan Zhen yang^ Ilya Maisara Dr Faiq, Mr GaneshaSupervisor:
● Periosteum ○ Fibrous layer: fibroblasts ○ Cellular layer: osteoprogenitor cells → osteoblasts, osteoclasts ○ Contains blood vessels, nerves, and lymphatic vessels that nourish compact bone
● Endosteum ○ Inner membranous lining of compact bone that lines the medullary cavity
Nutrient / medullary artery system: (High pressure system)
● Enter the cortex then medullary canal through nutrient foramen (mid-shaft) ● Branches into: ascending & descending → goes laterally to end of the bone → anastomosis with metaphyseal and epiphyseal vessels
Age group Most common organisms Newborns (<4 months)
S. aureus , Enterobacter species, and group A and B Streptococcus species Children (4 months - 4 years)
S. aureus , group A Streptococcus species, Kingella kingae , and Enterobacter species Children, adolescents (4 years - adult)
S. aureus (80%), group A Streptococcus species, H. influenzae , and Enterobacter species
Adult
S. aureus , occasionally Enterobacter or Streptococcus species
Organisms reach the bone through the bloodstream.
● Adult (5%) ○ Most common affected site = Vertebrae ○ infection reaches the vertebral column through spinal venous plexus ● ● Infant and children (95%) ○ Most common affected site = Long bone metaphysis
● Direct inoculation of bacteria ○ Trauma, open fracture, surgical reduction and internal fixation of fractures, prosthetic devices ○ ● Septic arthritis ○ Infection extend into the underlying bone → Erosions and osteomyelitis ○ ● Vascular compromise ○ Diabetes mellitus are predisposed to osteomyelitis due to inadequate local tissue response ○ Minor trauma to the feet → Multi-organism infection → Foot ulcers allow bacteria to reach the bone ○ Patients may not experience any resulting pain, because of peripheral neuropathy → Delayed treatment
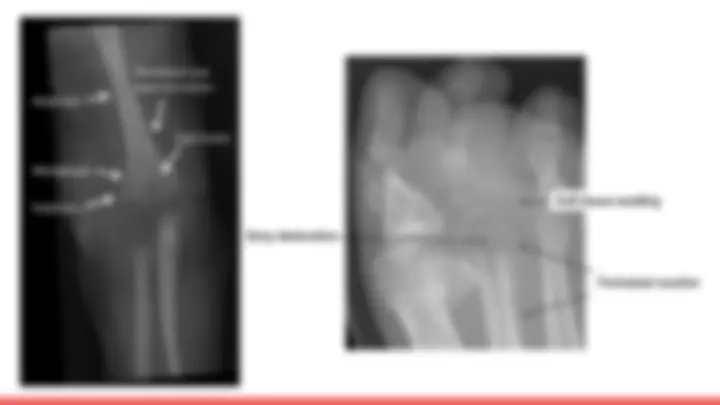
● Organisms reach the bone through the bloodstream from a septic focus elsewhere in the body ● ● Infection begins in the metaphysis of a long bone (productive medium for bacterial growth) ● ● It may spread to involve a large part of the bone. ● ● The organisms induce an acute inflammatory reaction but rigid structure of the bone not allow swelling. ● ● Pus is formed and soon finds its way to the surface of the bone where it forms a subperiosteal abscess
● Abscess may burst into the soft tissues and form a sinus
● Usually the blood supply to a part of the bone will be cut off by septic thrombosis ● ● The ischaemic bone dies and eventually separates from the surrounding living bone as a sequestrum ● ● New bone laid down beneath the stripped-up periosteum, forming an investing layer known as the involucrum
● Neurologic deficits present in 10-20% ○ direct infectious involvement of neural elements ○ compression from instability of the spine ○ compression from an epidural abscess ■ collection of pus or inflammatory granulation tissue between dura mater and surrounding adipose tissue
● Early onset (within 30 days of implant insertion) ○ Staphylococcus aureus, Beta-hemolytic streptococci, Gram-negative bacilli ○ Common cause: intraoperative contamination ● ● Late onset (>30 days of implant insertion) ○ Staphylococcus aureus, Corynebacterium spp., P. acnes ○ Frequently due to haematogenous infection
Symptoms ● Dull pain at the involved site with or without movement ● Refuse to bear weight (pediatrics) ● Fever
Signs ● Fever, tachycardia, hypotension ⇒ sepsis ● Erythematous, edematous limb ● Tenderness over the affected bone ● Increased local temperature ● Restricted ROM ● Draining sinus tract