Download patho mod 5 outline. and more Exams Pathophysiology in PDF only on Docsity!
Pulmonary
Outline
Review Types of Pulmonary Diseases video
Learning Objectives:
Compare and contrast the concepts of ventilation and oxygenation (ch. 20)
Describe pulmonary function evaluation and treatment for condition in the upper and lower airways (ch. 20,
Describe the various types of pneumonia, the risk factors, prevention and treatment options (ch. 20)
Differentiate the various diagnostic and imaging studies used to detect pulmonary disease (ch. 20,21)
Discuss common thoracic surgical options and care implications (there are a couple)
Identify risk factors and priorities for types of pneumothoraces (ch. 21)
Chapter 20:
Review A&P for refresher
Gas Exchange
What is oxygenation?
Gas exchange of oxygen and carbon dioxide occurs within the respiratory bronchioles, alveolar ducts, and alveoli.
Alveoli are thin-walled, balloon-like structures surrounded by pulmonary capillaries (see Fig. 20-2). This unique
structure enables transfer of both oxygen and carbon dioxide. Air enters the alveolus, and oxygen moves across the
alveolar membrane to the blood. At the same time, carbon dioxide moves from the blood into the alveolus to be
excreted by exhalation.
Oxygen combines loosely with the heme portion of hemoglobin to form oxyhemoglobin. The most important
function of hemoglobin is to combine with oxygen in the lungs and then release oxygen to the peripheral tissues. It
then collects carbon dioxide from the tissues and carries it back to the lungs to be excreted. Each hemoglobin
molecule can carry four oxygen molecules.
The volume of oxygen dissolved in the plasma varies directly with the partial pressure of oxygen in the arteries. The
relationship between the arterial pressure of oxygen and the percentage of saturation of oxygen in the blood (SaO 2 )
is shown in the oxyhemoglobin dissociation curve (see Fig. 20-3).
If the pressure of oxygen in the arterial blood (PaO 2 ) stays within the 90 to 100 mm Hg range, hemoglobin remains
maximally saturated with oxygen and tissues remain oxygenated. When PaO 2 falls below 60 mm Hg, hemoglobin
begins to drop oxygen molecules. The desaturation of hemoglobin leads to tissue hypoxia. To ensure optimal tissue
oxygenation, it is important to keep hemoglobin fully saturated with oxygen above PaO 2 of 90 mm Hg.
Erythropoietin, which is responsible for the stimulation of red blood cell (RBC) production, is secreted by the
kidneys in response to low oxygen levels in the bloodstream. Any condition that causes hypoxia, such as cardiac
disease, lung disease, or changes in atmospheric pressure, will stimulate secretion of erythropoietin. Erythropoietin
then stimulates the bone marrow to produce more RBCs that can carry more oxygen to the tissues.
What role do RBCs, HGB, and kidneys play in gas exchange?
Various receptors control the process, rate, and depth of respirations during inspiration and expiration. Central
chemoreceptors, located in the medulla, sense changes in carbon dioxide and blood pH and cause alterations in the
rate and depth of respirations. An increase in CO 2 (hypercapnia) or a decrease in pH (acidosis) stimulates the
central chemoreceptors, resulting in an increased rate of respirations. The end result is the return of the pH to
normal.
Chemoreceptors in the medulla also sense the hydrogen (H
) concentration of the cerebrospinal fluid (CSF). An
increase or decrease of pH in the arterial blood is reflected in a chemical change in the CSF. When CO 2 is retained,
carbonic acid (H 2 CO 3 ) levels in the blood increase. This increases the PaCO 2 level and lowers blood pH. In response
to these changes, the respiratory center at the medulla stimulates respirations.
Peripheral chemoreceptors, found in the aortic arch and bifurcation of the carotid artery (called carotid bodies),
respond primarily to a decrease in arterial oxygen. A decreased level of oxygen in the blood is sensed by the
peripheral chemoreceptors, which stimulate respirations; this is referred to as a hypoxic drive. A hypoxic drive takes
Pulmonary
Outline
over when CO 2 accumulation is not stimulating the medulla to control respiration, as in diseases such as chronic
obstructive pulmonary disease (COPD).
The normal stimulus to breathe is hypercapnia, an increase of carbon dioxide in the blood. The high CO 2 levels
stimulate the central respiratory center in the medulla. However, when central chemoreceptors are exposed to high
levels of CO 2 for extended periods, they become less responsive. The blunted response to CO 2 allows the peripheral
chemoreceptors of low O 2 to take over as the stimulus of respirations. The hypoxic drive becomes the main trigger
for breathing. This response correlates with a PaO 2 level of about 60 mm Hg, the point at which oxygen fully
dissociates from hemoglobin.
Baroreceptors, sensors of blood pressure, are also located in the aortic arch and carotid artery. Baroreceptors send
signals to the sympathetic nervous system, depending on blood pressure levels. When systolic blood pressure drops
to 80 mm Hg or lower, the baroreceptors stimulate the sympathetic nervous system to increase heart and respiratory
rate.
Proprioceptors, located in the muscles of movable joints, respond to body movement. When stimulated by exercise,
respiratory rate and depth increase. The purpose of these receptors is to maintain adequate oxygen levels during
periods of exertion.
The Hering–Breuer reflexes are stretch reflexes located in the bronchi and bronchioles. When the lungs inflate,
neuronal impulses are sent up the vagus nerve to the medulla. The result is an inhibition of rate, rhythm, and
duration of inspiration, which prevents the overdistention of the lungs.
See last clinical concept, pg. 473.
At high altitude, the decreased air pressure causes decreased levels of PO 2 , which stimulates erythropoietin. This, in
turn, increases production of RBCs, which is why individuals who live in mountainous areas have higher-than-
normal levels of hemoglobin and hematocrit.
inspiration and expiration are important for respiration counting. Define the two.
See alert pg. 474
The diaphragm is a muscle that separates the abdomen from the thoracic cavity. It is composed of both skeletal and
smooth muscle and is controlled both voluntarily and involuntarily. During inhalation, the diaphragm moves
downward or contracts at the same time the rib cage is being pulled up, resulting in lung expansion. The incoming
air movement as the lungs expand is inspiration. When the diaphragm ascends, the rib cage moves down and the
diaphragm compresses the lungs, promoting exhalation. The accompanying air movement with lung deflation is
referred to as expiration.
What is ventilation?
Ventilation is the process of inspiration and expiration of air through the pulmonary airways. Physical factors affect
the flow of air and oxygen content of the atmospheric air. At high altitudes there is low atmospheric pressure and
diminished oxygen content. The decreased O 2 levels trigger an increase in the rate and depth of respiration.
Perfusion is the movement of blood through the pulmonary circulation, eventually providing oxygen to every
part of the body. Circulation to the lungs begins with the pulmonary artery, which arises from the right ventricle. The
pulmonary artery divides into two trunks, which deliver blood to each lung. Oxygen and carbon dioxide are
dissolved in the blood and transported throughout the body at the same time.
The ventilation-perfusion ratio (V-Q ratio) is defined as the ratio of the amount of air reaching the alveoli to
the amount of blood reaching the alveoli; it is measured with a ventilation-perfusion (V-Q) scan. The ideal V-Q ratio
occurs when ventilation and perfusion are equal or when ventilation and perfusion match. When ventilation and
perfusion are unequal, there is ventilation-perfusion imbalance. An area with no ventilation is termed a shunt. An
area with no perfusion is termed dead space. The lungs have a built-in compensatory mechanism that attempts to
match blood flow and ventilation: where there is little ventilation, pulmonary arterial vessels constrict. Pulmonary
artery vasoconstriction leads to redistribution of blood flow to better-ventilated areas of the lung.
You should already know perfusion.
o See clinical concept pg. 474
Hypoxia stimulates pulmonary arterial vasoconstriction. Patients with chronic hypoxia can develop chronic
pulmonary vasoconstriction, which can result in pulmonary hypertension.
It is important that all functioning alveoli have adequate perfusion. Ventilation-perfusion imbalance occurs
when air cannot flow into an alveolus or blood flow around an alveolus is altered. One of the most common
etiologies for this is a blood clot in the lung, also called a pulmonary embolus (PE). The clot prevents blood
flow to the alveolus, and gaseous exchange cannot take place.
Pulmonary
Outline
Hypoxia
Hypoxia occurs when oxygen levels in the blood are insufficient to meet the needs of tissue. It can be caused by any
number of conditions that alter gas exchange across the alveolar membrane. Pulmonary edema, for example, creates
a fluid barrier to oxygen transfer across the alveolar–capillary interface. The term hypoxemia indicates a lack of
sufficient oxygen in the arterial blood, whereas the term anoxia indicates a zero amount of oxygen in the blood.
Chemical poisoning, such as that seen in carbon monoxide poisoning, can cause hypoxia. In this case, carbon
monoxide binds to hemoglobin as carboxyhemoglobin, which has a much higher affinity for hemoglobin than
oxygen and prevents oxygen from binding to the hemoglobin molecule. High levels of carbon monoxide in the
bloodstream can be fatal.
Impending Respiratory Failure
Respiratory failure occurs when the pulmonary system fails to oxygenate the blood or fails to sufficiently eliminate
carbon dioxide. It is classified as either hypoxemic or hypercapnic respiratory failure.
Hypoxemic respiratory failure occurs when the pressure of oxygen in arterial blood (PaO 2 ) is lower than 60 mm
Hg with normal arterial carbon dioxide (PaCO 2 ). Many acute diseases of the lung can cause respiratory failure,
including pulmonary edema, PE, pneumonia, or pneumothorax.
Hypercapnic respiratory failure occurs when carbon dioxide in arterial blood (PaCO 2 ) is greater than 50 mm Hg.
Common causes of hypercapnia include COPD and asthma. Hypoxemia commonly accompanies hypercapnic
respiratory failure in persons who are breathing room air.
It is challenging to predict when a patient will cease independent breathing and incur respiratory failure. Serial
arterial blood gases (ABGs) should be evaluated in all patients with respiratory problems. Usually, there is a gradual
increase in arterial carbon dioxide and a decrease in arterial oxygen when a patient is developing respiratory failure
(see Table 20-1). The patient typically appears distressed, may be using accessory respiratory muscles, and has
difficulty maintaining a normal respiratory rate despite oxygen administration. Patients at risk of respiratory failure
need intubation equipment ready at the bedside. The patient’s whole clinical picture should be considered when
deciding to intubate. After the patient’s ventilatory status is corrected, the underlying pathophysiological process that
led to respiratory failure needs investigation.
Physical Assessment:
Bradypnea vs Tachypnea vs hyperventilation
What does cyanosis look like?
Assess the rate, rhythm, and depth of respirations by observing the rise and fall of the chest during breathing. The
presence of retractions, visible indentation of the intercostal and supraclavicular spaces, is a sign of increased work
of breathing and respiratory distress; it indicates that accessory muscles are necessary for inspiration. Nasal flaring is
also a sign of respiratory distress. Normal respiratory rate is 12 to 20 breaths per minute. Bradypnea, or
hypoventilation, is a respiratory rate less than 12 breaths per minute, whereas tachypnea, or hyperventilation, is a
respiratory rate greater than 20 breaths per minute.
Diagnostic Testing: What are the 7 tests listed and when would we use them?
Arterial Blood Gases. ABGs are serum blood values obtained through an arterial puncture. They enable
identification of alterations in acid–base balance caused by respiratory diseases. ABG results include blood pH,
partial pressure of O 2 , CO 2 , bicarbonate ion, and the saturation of hemoglobin (Hgb) (see Table 20-2). A pH of more
than 7.45 indicates alkalosis, and a pH of lower than 7.35 indicates acidosis (see Chapter 8 ).
The level of arterial oxygen (PaO 2 ) indicates the degree of oxygenation of the blood. The saturation of Hgb with
oxygen (SaO 2 ) in the arterial blood also indicates the arterial oxygenation. The arterial carbon dioxide level (PaCO 2 )
is an indicator of alveolar ventilation. The PaO 2 and PaCO 2 values are useful in determining the ability of the lungs
to provide oxygen and remove carbon dioxide. The pH of the blood is balanced by the lungs and the kidneys. The
lungs regulate CO 2 , and the kidneys regulate conservation and excretion of acid (H
) and HCO 3
(bicarbonate ion).
The following equation demonstrates the chemical reaction occurring in the bloodstream in terms of CO 2 , H
(acid)
and HCO 3
(base) (as discussed in Chapter 8 ): CO 2 + H 2 O ↔ H 2 CO 3 ↔ H
+ HCO 3
Pulmonary
Outline
Culture and Sensitivity Testing. Culture and sensitivity testing of sputum samples can assist in the diagnosis of
respiratory infection. Sputum that has been obtained by expectoration may be contaminated with normal flora from
the mouth. Microscopic examination for the presence of epithelial cells from the oral mucosa can help determine if it
is contaminated. Sputum cultures obtained by suctioning the respiratory tract or through bronchoscopy are less
likely to be contaminated by normal flora. Acid-fast smears and cultures of the sputum are used for TB. Nucleic acid
amplification tests (NAAT) on sputum, also used to identify the presence of TB, can provide more rapid results than
acid-fast smear and culture. NAAT can be used to diagnose other types of pathogens that cause respiratory infection
or malignancy.
Pulse Oximetry. Pulse oximetry can continuously monitor the oxygen saturation of hemoglobin (SaO 2 ). A small
probe is attached to an extremity, usually the fingertip, although the forehead, earlobe, or toe may also be used.
Infrared light passes over the extremity, reflects the blood pulsing through the tissue, and senses changes in oxygen
saturation. Normal SaO 2 is 95% to 100%. A saturation level lower than 95% indicates that tissues are not receiving
enough oxygen.
Imaging Studies. Imaging studies used to diagnose lung disease include chest x-rays, CT, and MRI. Chest x-ray can
demonstrate numerous abnormalities, including inadequate lung expansion, areas of consolidation, changes
associated with COPD, tumor, pneumothorax, or the presence of fluid in or around the lungs. It is also often used to
evaluate the response to treatment. A CT scan shows a more specific cross-sectional view of the respiratory system
and can identify many different pathological conditions, such as lung abscesses, tumors, TB, and pleural effusion. A
chest MRI can be used to provide more detail than a CT scan. Inhaled hyperpolarized gas MRI can use inhaled gases
to evaluate ventilation and gas exchange in the lungs.
Bronchoscopy. Bronchoscopy allows for direct visualization of the larynx, trachea, and bronchi, which can then
allow for biopsy and removal of foreign objects. Secretions may also be removed using suctioning during the test.
Endobronchial ultrasound can be used with bronchoscopy to assist in the diagnosis of inflammatory, infectious, or
cancerous respiratory conditions.
Thoracocentesis. Thoracocentesis is the removal of pleural fluid using a large-bore needle inserted through the chest
wall into the pleural space. The procedure can be used to obtain specimens for culture and sensitivity or biopsy.
Medication may also be inserted during the procedure.
Pulmonary Function Tests. Pulmonary function tests (also called spirometry) can be used in the diagnosis of
inflammatory respiratory diseases. These tests evaluate lung volumes, such as inspiratory and expiratory flow and
residual lung volume, and can differentiate between obstructive and restrictive diseases.
Treatment: Know the broad overview of pharm and non-pharmacologic support.
Alert pg. 480 (Keep in mind when thinking about treating a cough)
Treatment of inflammatory and infectious pulmonary disease includes a variety of drugs and procedures. The
following includes general treatment measures. Bronchodilators reduce bronchospasm, and antibiotics treat bacterial
respiratory infections. PE can be treated with thrombolytic and anticoagulant medications. Decongestant
medications cause vasoconstriction that helps to reduce the inflammation and edema in the nasal passage and relieve
nasal congestion. Antihistamine medications block the inflammatory effects of histamine in the airways. Antitussive
medications can be used to control coughs. A warm saltwater gargle and mild analgesics can be used to treat
pharyngitis (sore throat). Antiviral drugs, such as amantadine, are available to lessen the effects of viral infection in
the respiratory tract.
Pulmonary hygiene measures are used to clear the respiratory tract of mucus and purulent drainage. Methods used
for pulmonary hygiene include suctioning of the airways, chest physiotherapy, incentive spirometry, and
nasotracheal suction. Percussion over the chest loosens secretions and allows the cilia of the airways to remove
material. Positioning is another method for promoting drainage of secretions. Intermittent positive pressure
breathing physiotherapy is often used in nonintubated patients. Nebulizers can deliver humidified air with
medication. Supplemental oxygen and mechanical ventilation are used when hypoxia or respiratory failure occur.
ALERT! Coughing is important for ridding the airways of secretions, so clinicians do not want to inhibit
coughing or oversedate the patient to a point that weakens the cough.
Pulmonary
Outline
Epiglottitis
Epiglottitis is the infection and inflammation of the epiglottis—the flap of tissue that sits atop the trachea to keep
food from going into the trachea during swallowing. When inflamed, the epiglottis can obstruct the trachea. It may
be caused by a respiratory infection, exposure to chemical substances in the environment, trauma, and various
organisms, including bacteria, viruses, and fungi. Common organisms that cause epiglottitis include Streptococcus
pneumoniae, Haemophilus influenza , parainfluenza, varicella-zoster virus, herpes simplex virus type 1,
and Staphylococcus aureus.
The disorder begins as inflammation and swelling between the base of the tongue and the epiglottis. The swelling
pushes the epiglottis backward; as the process continues, complete blockage of the airway occurs, leading to
suffocation and death.
X-rays and a laryngoscopic examination will show that the pharynx is inflamed, red, and stiff and that the
epiglottis is swollen. Blood tests will show signs of infection or inflammation, ABGs will confirm lack of gas
exchange, and cultures may grow bacteria and indicate the causative organism. Neck x-ray shows a characteristic
swelling of the pharyngeal tissues called “steeple” sign.
Immediate hospitalization is usually necessary, as there is a danger of sudden and unpredictable closing of the
airway. Initial treatment includes making the person as comfortable as possible, humidified oxygen, and IV fluids.
Antibiotics are given to control inflammation and stop the infection after the causative organism has been identified.
Laryngitis and Tracheitis
Laryngitis is inflammation of the larynx, whereas tracheitis is inflammation of the trachea. The infection that causes
both is usually viral in nature, although bacteria such as Haemophilus influenza can also cause the infection. Signs
of acute laryngitis are hoarseness or complete loss of the voice. If the infection involves the larynx, trachea, and
bronchi, then laryngotracheobronchitis, commonly called croup, occurs. Croup is mainly a children’s disease.
In laryngitis, an irritating, high-pitched cough may be present. Tracheal involvement can produce a raspy cough
or stridor, a high-pitched inhalation sound. Pleuritic chest pain may indicate pleural or other musculoskeletal
involvement. The underlying cause of the cough is the irritation of the mucous membranes. Eventually, sputum will
be produced in response to the chronic irritation. Sputum is usually thin and may be yellow or green when bacteria
are causing the infection. Thin mucoid sputum may indicate a viral or bacterial infection. Foul-smelling sputum may
indicate a lung abscess. As airways narrow, the patient begins to wheeze mainly upon expiration.
There is no specific medical intervention for viral laryngitis other than resting the voice and managing the
symptoms. If the infection has spread and proves to be bacterial, antibiotics may be administered. Bronchodilator
medications are useful if the airway has narrowed, and wheezing is present. Tracheitis can involve the epiglottis; if
so, it can become a medical emergency.
Compare/Contrast acute bronchitis (ch. 20) to chronic bronchitis (Ch. 21) (A Venn diagram can help)
Acute Bronchitis
Acute bronchitis is an inflammation of the bronchi and bronchioles caused by either bacterial or viral infection.
Bronchitis can also be triggered by inhalation of toxic gases or chemicals.
Epidemiology
It is estimated that 44 out of 1,000 adults suffer from acute bronchitis in the United States annually. This is likely a
low estimate because not all individuals with acute bronchitis seek health care. Most episodes occur in fall or winter.
Etiology
Respiratory viruses are the most common causes of acute bronchitis. The most common viruses include influenza A
and B, parainfluenza, respiratory syncytial virus, and coronavirus. Bacteria that cause acute bronchitis
include Mycoplasma species, Chlamydia pneumoniae, Streptococcus pneumoniae, Moraxella catarrhalis ,
and Haemophilus influenzae. Bordetella pertussis , which causes whooping cough, is another microorganism that can
cause bronchitis. B. pertussis has had a recent resurgence in incidence in the United States after many years of
successful eradication because of pertussis vaccine.
ALERT! Epiglottitis is a medical emergency. A laryngoscope and tracheostomy equipment should be available at
the patient’s bedside at all times, because intubation may be needed.
Pulmonary
Outline
Cigarette smoking and exposure to pollutants or chemical irritants increase susceptibility to bronchitis. URIs such
as the common cold, sinusitis, and pharyngitis also increase susceptibility to acute bronchitis. Influenza is
commonly complicated by acute bronchitis.
Pathophysiology
In acute bronchitis, the bronchial tree undergoes an inflammatory response to a pathogen or irritant. The cells of the
bronchial tissue are irritated, and the mucous membrane becomes edematous, diminishing the bronchial mucociliary
function. The air passages become obstructed by excessive mucus. Dysfunctional mucociliary movement and excess
mucous secretion cause patients to frequently cough to clear the airway of secretions. Pleuritic chest pain with
inhalation and exhalation, fever, and general malaise are also common.
Clinical Presentation
In the history, the patient may report that the illness began as a common cold. It is important to ask the patient when
the symptoms began to exclude chronic bronchitis as the diagnosis. The clinician should ask about recent exposure
of the patient to others who are ill, recent exposure to pollutants or occupational chemicals, and past medical history.
It is important to know if the patient has a history of asthma because acute bronchitis sometimes presents with
wheezing. The patient usually complains of sore throat, nasal discharge, muscle aches, and persistent cough. The
initial days of infection can appear as the common cold and fever, and headache may occur. Cough becomes
prominent as the disease progresses and can last from 10 to 20 days during the course of acute bronchitis. Sputum
production is reported in most patients. Sputum may be clear, yellow, green, or even blood tinged. Purulent sputum
is reported in 50% of persons with acute bronchitis. Sputum color is not indicative of bacterial versus viral infection.
On physical examination, the patient may exhibit pharyngeal erythema, localized lymphadenopathy, and
rhinorrhea. Rhonchi and wheezes can be heard across all lung fields. In severe cases, diffuse wheezes, high-pitched
continuous sounds, and the use of accessory muscles can be observed. Coughing can clear some of the rhonchi and
wheezes. Inspiratory stridor indicates that there may be mucous obstruction within the trachea.
Diagnosis
Diagnosis is mainly based on symptomatology, although a culture of respiratory secretions may be done. A CBC
may be useful to distinguish bacterial infections from nonbacterial infections. A chest x-ray is usually done to rule
out pneumonia.
Treatment
Broad-spectrum antibiotics are used to treat bacterial infections. Expectorant medications will assist the individual to
cough up the exudate and mucus. Mucolytic agents can dissolve mucus. At times a bronchodilator is necessary if
bronchospasm is present with cough. Cough suppressants may be needed at night to allow the individual to sleep.
Chronic Obstructive Pulmonary Disease
Chronic obstructive pulmonary disease (COPD) is a combination of chronic bronchitis, emphysema, and
hyperreactive airway disease. It is characterized by the features of these three disorders.
Epidemiology
COPD is the third leading cause of death in the United States and a leading cause of disability. It is estimated that
there are 16 million persons with COPD; most are over age 45. However, the prevalence is believed to be up to
twice that number because of underreporting of individuals who do not seek health care. In the past, COPD had a
higher prevalence in men, but from 1980 to 2000, the mortality rate from COPD increased dramatically in women;
today, more women than men die of COPD. In the United States, the economic burden of this disease, estimated at
$24 billion annually, is caused by the cost of medical care and days lost from work.
Etiology
Smoking is the major cause of COPD, as 90% of patients with this condition are smokers, but occupational and
environmental exposures to chemicals, dusts, and secondhand smoke are also causes. COPD is caused by a
combination of genetic susceptibility and environmental factors. One such genetic predisposition to COPD is caused
by alpha 1 anti-trypsin (AAT) deficiency. This rare genetic variant accounts for less than 1% of all COPD cases.
Chronic bronchitis is diagnosed when a patient reports a history of bronchitis for 3 months out of the year for at
least 2 years.
Pulmonary
Outline
- What is the frequency and quality of the cough? Is it productive of sputum? Is hemoptysis present? If so, how
much?
- Has there been any wheezing?
- Is there a history of smoking? If so, what is the pack-year history?
- Is secondhand smoke a problem at work or home?
- Has there been any weight loss? What is the patient’s pattern of exercise?
- Is there a history of alcohol use? Illicit drugs?
- Is there a family history of respiratory illness?
Along with these questions, ask about the patient’s past and present occupations, particularly focusing on possible
exposure to toxins such as asbestos, silica, hydrogen sulfide, lead, mercury, coal, cotton dust, and diisocyanates.
Also obtain the patient’s complete list of current medications, including herbal and over-the-counter medications, as
well as information about allergies.
Signs and Symptoms. Signs and symptoms of COPD include those of chronic bronchitis, emphysema, and asthma.
Dyspnea is usually the first symptom, initially occurring with heavy exertion. As the disease progresses, dyspnea
becomes increasingly worse with less and less vigorous exertion. Cough or wheezing may be a chief complaint. The
cough may be productive, and sputum should be expectorated for culture. Productive cough, hypoxia, and cyanosis
are classic signs of chronic bronchitis. The hypoxia of chronic bronchitis stimulates pulmonary arterial
vasoconstriction. Over time, because of the high resistance against the right ventricle, right ventricular failure
occurs. The signs and symptoms of right-sided heart failure, such as jugular venous distension, ascites,
hepatosplenomegaly, and ankle edema, develop after long-term chronic bronchitis.
Observe the patient for signs of respiratory distress, use of intercostal muscles or accessory muscles with
breathing, and clubbing of the fingers (see Fig. 21-2).
Examine the thoracic cage structure. A barrel-shaped chest is commonly present in emphysema; this is a shape
that has an equal diameter of the width and depth of the chest. In healthy persons the width of the chest should be
double the depth of the chest. In emphysema, there is an accumulation of air in the alveoli, which over time
increases the width and depth of the thoracic cage.
Observe the patient’s complexion. Cyanosis, commonly visible around the lips, indicates hypoxia. In those with a
lengthy smoking history, the teeth or fingertips may be tobacco stained. Examine the jugular veins, abdomen, and
ankles. Distended jugular veins, ascites, and ankle edema indicate cor pulmonale (right ventricular failure).
With regard to vital signs, focus particularly on respiratory rate, rhythm, and depth. Patients with COPD often
have prolonged exhalation and purse the lips when exhaling. The examiner can palpate the posterior lung fields
bilaterally for tactile fremitus. Vibrations over lung fields should be equal as the patient vocalizes “ninety-nine.” The
posterior lung fields can also be percussed bilaterally for resonance. In severe emphysema, hyperresonance may be
percussed because of the extra air retained in the lungs. Auscultate the heart and note any abnormal sounds.
Commonly wheezing is heard over the lung fields in COPD. Diminished breath sounds may suggest severe disease.
Identify the location of any adventitious sounds.
Diagnosis
The COPD Assessment Test (CAT) is a patient questionnaire that asks specific questions about the patient’s
breathing ability and activity limitations due to their pulmonary symptoms. There are eight questions that ask about
breathlessness, cough, chest tightness, sputum, and activity level. Each item is scored on a scale of 0 to 5, with a
higher total score indicating more severe disease.
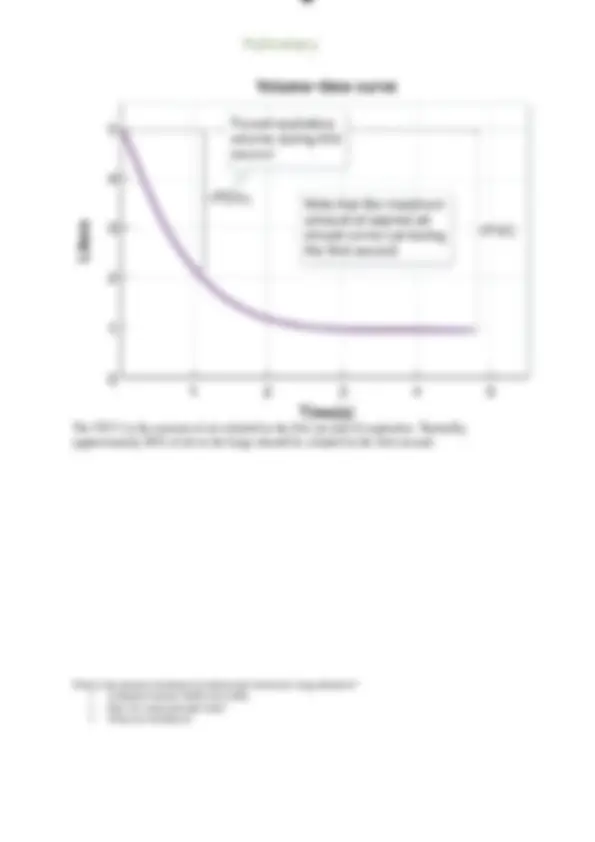
PFTs (also called spirometry) are a key part of the diagnosis of COPD (see Box 21-1). Common parameters
measured in PFT s include FVC and FEV1. FVC is the total volume of air that can be exhaled with maximum effort.
FEV1 is the volume of air expelled during the first second of exhalation of air from the lungs. Airflow limitation of
COPD is identified by a FEV1/FVC ratio of less than 70%. FEV1 significantly diminishes in COPD because the
patient’s exhalation phase is slow and prolonged (see Fig. 21-7).
A complete blood count (CBC), blood chemistry panel, chest x-ray, electrocardiogram (ECG), and ABGs should
be analyzed. In individuals with mild to moderate disease, all laboratory data should be normal except for the PFTs.
In severe COPD, the chest x-ray may show characteristics consistent with emphysema: flattened, low diaphragm
borders and hyperinflation of both lung fields caused by retained air. The ECG commonly demonstrates a right axis
deviation caused by right ventricular hypertrophy. Also in severe COPD, an enlarged heart may be visible because of
right ventricular failure. The pulmonary vasculature may be constricted if pulmonary hypertension exists because of
Pulmonary
Outline
chronic bronchitis. In those with severe hypoxia, the CBC will indicate erythrocytosis (high number of erythrocytes)
caused by the constant secretion of erythropoietin from the kidney. Eosinophilia will be present if allergy exists.
Treatment
Treatment of COPD involves a stepwise approach that begins with short-acting bronchodilator agents for patients
with mild disease and incorporates long-acting agents into the treatment plan as the disease progresses in severity.
Beta-2-adrenergic agonist inhalers stimulate bronchiole smooth muscle, leading to dilation, whereas anticholinergic
inhaler agents counteract bronchoconstriction. Inhaled bronchodilators, which include SABAs and LABAs, and
long-acting anticholinergic agents (also called long-acting antimuscarinic agents, or LAMAs) are the cornerstone
of therapy. Inhaled bronchodilators are the treatment of choice in patients with COPD who have respiratory
symptoms and an FEV1 that is less than 60% of normal. Similar to asthma, a combination inhaler that contains a
LABA and IC is commonly prescribed for daily maintenance treatment. The patient is also prescribed a SABA to
use for acute episodes of bronchospasm.
Phosphodiesterase inhibitors, such as theophylline, can be added to the regimen when the patient does not
respond adequately to bronchodilators. Oral corticosteroids are used when the patient has an acute exacerbation and
does not respond adequately to bronchodilators. The patient needs to use oral corticosteroids in low doses for a short
time and be weaned off them slowly.
Leukotriene antagonists are another type of maintenance agent used in asthma and COPD to counteract
bronchoconstriction and inflammation in the bronchioles. These drugs block the lipoxygenase pathway of
inflammation that yields leukotrienes and should be used daily.
Nonpharmacological interventions include smoking cessation, pneumococcal and influenza vaccines, pulmonary
rehabilitation, and oxygen therapy. Pulmonary rehabilitation involves a slowly progressive program of aerobic
exercise and endurance training with supervision. Ventilatory muscle training is used with patients who have
decreased respiratory muscle strength and debilitating breathlessness. Pulmonary rehabilitation should be used for
symptomatic patients who demonstrate an FEV1 less than 50% of normal on PFTs.
Continuous oxygen therapy is indicated when arterial PO 2 is lower than or equal to 55 mm Hg or the saturation of
oxygen in the blood is less than or equal to 88%. Oxygen is also indicated if there is evidence of pulmonary
hypertension, cor pulmonale, cognitive impairment caused by hypoxia, or polycythemia and a PO 2 of 56 to 59 mm
Hg. Oxygen should be used in the lowest doses that can enhance the patient’s oxygenation. Oxygen therapy requires
slow upward titration to the level that assists the patient’s oxygenation while still maintaining the patient’s
independent respiratory drive.
Mechanical ventilator support via an endotracheal tube is indicated for patients with severe respiratory distress
unrelieved by other therapies, life-threatening hypoxemia, severe hypercapnia, respiratory acidosis, or respiratory
arrest. There is a 17% to 30% mortality rate for patients requiring mechanical ventilatory support. For patients older
than 65 years who require critical care for COPD, the mortality rate doubles to 60%, regardless of the need for
mechanical ventilation.
LVRS is indicated in severe emphysema when nonsurgical therapies have proven to be limited in effectiveness.
The goals of LVRS are to remove the most severely diseased areas of emphysematous lung and to decrease the
degree of lung hyperinflation. The procedure removes the severely damaged alveoli that act as dead spaces that do
not allow diffusion of oxygen into the circulation.
Pneumonia:
See video "What is pneumonia."
You learned a little about S. Pneumoniae, now you will learn more.
Hospital-Associated (HAP) vs. Community-Acquired (CAP)
What are the 4 main risk factors for pneumonia?
What is the patho? Clinical Manifestations? Diagnostic tests? Treatment? (flashcard)
ALERT! When oxygen is administered to a patient with severe COPD, the lowest dose of oxygen that relieves the
patient is recommended. It is important to recognize that the patients stimulus to breathe is hypoxia, and high
oxygen levels can decrease the patient’s independent drive to breathe. Oxygen administration higher than 2 liters
per minute will decrease or interrupt the stimulus for breathing and can result in respiratory arrest.
ALERT! Tranquilizers, sedatives, and opiates can depress respiratory drive and cause respiratory failure in
patients with severe COPD.
CLINICAL CONCEPT
Cough, crackles, and fever are the characteristic signs of pneumonia. In older adult patients, hypothermia may
present instead of fever.
Pulmonary
Outline
pneumonias. Environmental sources of pathogens can cause clusters of infection in the population, such
as Legionella pneumophila (referred to as Legionnaire’s disease). Bioterror pathogens can cause pneumonia,
particularly Bacillus anthracis —the cause of anthrax.
Pathophysiology
Pneumonia is most commonly caused by inhalation of droplets containing bacteria or other pathogens. The droplets
enter the upper airways and then enter the lung tissue. Pathogens adhere to respiratory epithelium and stimulate an
inflammatory reaction. The acute inflammation spreads to the lower respiratory tract and alveoli. At the sites of
inflammation, vasodilation occurs, and neutrophils travel out of capillaries into the air spaces. The neutrophils
phagocytize microbes and kill them using reactive oxygen species, antimicrobial proteins, and degradative enzymes.
There is an excessive stimulation of respiratory goblet cells that secrete mucus. Mucous and exudative edema
accumulate between the alveoli and capillaries. The alveoli attempt to open and close against the purulent exudate;
however, some cannot open. The sounds heard with the stethoscope over the alveoli opening against the exudative
fluid are crackles. A layer of edema and infectious exudate at the capillary-alveoli interface hinders optimal gas
exchange. The patient can become hypoxic and hypercapnic, with obstructed exchange of 2 aOnd CO 2 at
the (^) pulmonary capillaries.
Clinical Presentation
The clinical presentation of bacterial pneumonia usually starts with a sudden onset of symptoms. Cough, which may
or may not be productive of sputum; fever; and chills are usually initial manifestations. Pleuritic chest pain, which is
pain with deep breaths; dyspnea; hemoptysis; and decreased exercise tolerance develop as the disorder continues.
Other nonspecific symptoms that may be seen with pneumonia include myalgias, headache, abdominal pain, nausea,
and vomiting. Headache and earache, with less cough and fever, are the symptoms that occur
with Mycoplasma pneumonia.
On physical examination, the patient is likely to demonstrate fever, tachypnea, use of accessory muscles with
breathing, tachycardia, and possibly cyanosis. Crackles are pathognomonic of pneumonia, and the clinician can
elicit egophony, bronchophony, and whispered pectoriloquy. There may be dullness to percussion and increased
fremitus over the site of pneumonia. The patient may have periodontal disease, which can increase susceptibility to
aspiration pneumonia with anaerobic infection. Poor cough and gag reflex increases the risk of aspiration
pneumonia. Otitis media (middle ear infection) and myringitis (inflammation of the tympanic membrane) typically
occur in Mycoplasma pneumoniae infection.
When interviewing the patient, it is important to assess exposure to any other persons who are ill and evaluate if
the patient has any aspiration risks or immunosuppression factors. The clinician should ask the patient about current
medications, allergies, and past medical history. Conditions such as influenza, asthma, or COPD increase
susceptibility to pneumonia. Social habits, such as smoking and use of alcohol or illicit drugs, are also factors that
increase risk for pneumonia.
Diagnosis
A chest x-ray is the most important diagnostic study in the diagnosis of pneumonia (see Fig. 20-6). CBC with
differential will suggest either a bacterial or viral infection. Pulse oximetry can demonstrate oxygenation. Sputum
culture and sensitivity can exhibit the organism and antibiotic susceptibility. Ultrasound and thoracocentesis are
useful if pleural effusion is suspected. Sputum, serum, and urinary antigen tests are available for S.
pneumoniae and Legionella.
Treatment
Antibiotic therapy and oxygenation of the patient are key priorities in the treatment of pneumonia. Fowler’s position
and oxygen via nasal cannula or mask are recommended. The patient may require IV fluids if dehydrated. Analgesia,
antipyretics, and bronchodilators may be needed. To prevent pneumonia in older adults, infants, and children with
risk factors, the pneumococcal vaccine is recommended.
Pulmonary
Outline
TB:
Know the usual and the diagnostic tests
See video on TB Pathogenesis. The others are optional.
What link is there between autoimmune disorders and TB?
What do patients receiving treatment need to remember as they begin to feel better.
Pay close attention to which test is for exposure vs. active.
Tuberculosis
TB is an infection caused by the Mycobacterium tuberculosis bacterial organism. Although most commonly
occurring in the lungs, TB can infect other parts of the body, such as the adrenal gland, vertebrae, meninges, and
lymph nodes. It can also spread within the bloodstream and cause multisystem disease. There are two forms of TB:
TB disease and latent TB infection (LTBI) (see Fig. 20-8). In TB disease the infected individual has symptoms and
clinical evidence of active disease. They are usually severely ill, infectious to others, and can die if not treated. In
LTBI the individual has been infected with the M. tuberculosis organism but the disease is dormant. The individual
has no clinical symptoms and is noninfectious. Both forms require treatment, as LTBI can convert to active TB
disease at any point during the individual’s lifetime if not treated.
Epidemiology
TB is one of the top 10 causes of death in the world. HIV infection and TB are among the most lethal infectious
diseases. According to the most recent data from 2014, it is estimated that globally, one-fourth of the world’s
population is infected with M. tuberculosis. The majority, 1.7 billion persons, have latent TB infection.
Approximately 10% of these persons are speculated to progress to active TB disease in their lifetime.
The prevalence of TB is particularly high in Africa, India, and Asia. In 2018 the incidence of TB in the United
States was 2.8 per 100,000 persons, a 1.8% decrease from 2016. This is the lowest incidence on record. African
Americans, Hispanics, and immigrants have the highest incidence of TB in the United States. Persons with
immunosuppression, particularly persons with HIV, those receiving cancer chemotherapy, or those receiving
biologic agents for autoimmune disease, have the highest susceptibility to TB.
According to the World Health Organization (WHO), due to an effective international treatment campaign to
eradicate TB, the incidence has been declining globally by approximately 1.5% per year. Currently, there are two
sets of goals put forth by the WHO for the elimination of TB: a 90% reduction in incidence by 2035 and less than
one case per million population, per year by 2050. According to experts, this is a formidable challenge.
Pulmonary
Outline
Persons can present with TB of the bones, lymph nodes, meninges, or adrenal gland. Patients with tuberculous
meningitis complain of headache that is either intermittent or persistent for 2 to 3 weeks. Fever may be low-grade or
absent. Skeletal TB involves the vertebrae and is also called Pott’s disease. Symptoms include back pain or stiffness,
and lower-extremity paralysis occurs in up to half of the patients. TB can also involve the joints, causing swelling
and stiffness. Scrofula is TB of the lymph nodes, which usually occurs in the neck. TB of the adrenal gland can
cause decreased cortisol levels exhibited by severe hypotension and weakness.
On physical examination, pulmonary TB will be exhibited by crackles or bronchial sounds in the lungs over the
area of involvement. Lymph nodes may be enlarged in the cervical, supraclavicular, or axillary areas. However,
many persons exhibit no significant physical findings, so absence of physical signs does not exclude active TB. In
patients who are immunosuppressed, classic symptoms are often absent. In fact, up to 20% of patients with active
TB may not have any symptoms. Therefore, sputum testing is essential when chest x-ray is consistent with TB.
Diagnosis
The Mantoux tuberculin skin test is a screening test for TB. The test can indicate only if an individual has had
prior exposure and sensitization to the organism M. tuberculosis. It does not differentiate LTBI from active TB
disease. In the Mantoux tuberculin test, a small amount of purified protein derivative (PPD), which is an extract of
the tubercle bacteria, is injected intradermally into the forearm. For this reason, the Mantoux test is sometimes
referred to as a PPD test. After 48 hours, the injection site should be checked for a reaction of induration, which
appears as elevated and hardened. If there is no induration at the site, the test is negative and the individual is
considered uninfected. An induration of 5 to 15 mm may be positive, depending on the person’s risk factors and
susceptibility to TB. A reaction greater than 15 mm of induration is interpreted as positive in all persons.
In some countries of Europe, the Middle East, Africa, and Asia, individuals commonly receive the Bacillus
Calmette–Guérin (BCG) TB vaccine. This vaccine protects the individual from contracting TB. These individuals
will test positive on the Mantoux test, an indication of previous sensitization with PPD. The positive reaction does
not necessarily mean that the individual is infected with TB. However, most individuals who test positive are
required to get a chest x-ray to check for active disease.
The interferon gamma release assay (IGRA) is a blood test also used to screen for TB. This test demonstrates
whether the immune system has been exposed to TB bacteria. A positive IGRA test requires further testing of the
individual to decipher if there is latent TB infection or active TB disease. A chest x-ray or CT scan can rule out
active TB. The IGRA result is not affected by a previous BCG vaccine.
The WHO recommends the rapid test called Xpert MTB/
R
ItFo expedite the diagnosis of TB. The
test diagnoses TB and detects resistance to rifampicin, a first-line TB medication. Diagnosis can be made within 2
hours, and the test is recommended as the initial diagnostic test for all persons with signs and symptoms of TB. If
positive,
it is followed by additional testing. A sputum smear for acid-fast culture and sensitivity of M. tuberculosis is the
most reliable test for diagnosis of TB. This test also can determine which antibiotic will be most effective against the
bacteria. NAAT also can be used to detect M. tuberculosis in sputum and infected tissue. Although it is used to
support the diagnosis of TB, acid-fast culture is the primary laboratory test. Chest x-ray, as well as HIV testing, is
important. If chest x-ray findings suggest TB and the sputum smear is positive for acid-fast bacteria, treatment is
initiated.
The classic chest x-ray exhibits a round granuloma, called a “tubercle,” usually toward the apex of the lung.
(see Fig. 20-9). CT scan or MRI can also demonstrate the granulomatous mass in TB.
Treatment
Antimicrobial medications, including isoniazid, rifampicin, pyrazinamide, ethambutol, and streptomycin, are used in
combination therapy to treat patients with active TB and as prophylactic therapy for those who have had exposure to
and are at risk for developing active TB. Isoniazid and rifampicin are the first-line drugs within the regimen.
TB bacteria mutate rapidly and easily acquire resistance to any one drug; therefore, usually a combination of four
different drugs is used. Multidrug therapy is required for a long time, usually 6 to 12 months, and may need to
continue longer in patients with an HIV infection or those with drug-resistant strains of TB. Treatment protocols are
based on the health of the patient and the type of TB strain.
Because the bacteria travel through the air, patients are placed in respiratory isolation until they are no longer
considered contagious. Adequate hydration and nutrition are necessary to aid in recovery from the disease. TB is
considered chronic in nature, as there is a potential for reactivation of active disease if a patient becomes
immunosuppressed. Patient teaching is needed about the possibility of recurrence and spread of the disease. Because
Pulmonary
Outline
drug therapy extends over a prolonged period, the proper use of prescribed medications needs to be reinforced.
Many patients fail to maintain the full regimen, which can lead to the development of resistant TB bacteria.
Multidrug resistant (MDR) TB is an increasing problem. This most often occurs when patients fail to take the
complete medication regimen. TB organisms mutate and possess genetic mechanisms that can endow them with
resistance when exposed to medication. Currently, resistance to isoniazid and rifampicin, the two most powerful
first-line drugs, is increasing in the population, which is becoming a public health crisis.
Chapter Summary
- URIs are among the most common reasons for patients to seek health care.
- Rhinitis can be caused by infection or allergy; infection is mainly caused by rhinovirus or adenovirus.
- GABHS is a common cause of pharyngitis; it can lead to rheumatic fever, rheumatic heart disease,
glomerulonephritis, and other disorders.
- Epiglottitis, a condition that can occur as a complication of laryngitis and tracheitis, is a medical emergency that
can cause asphyxiation.
- The right bronchus is vertical and wider than the left bronchus, making aspiration pneumonia more common in the
right lung.
- Aspiration pneumonia can occur in debilitated persons, those with decreased level of consciousness, and persons
with a weak gag or cough reflex.
- Acute bronchitis is a common complication of URI and influenza infection.
- Chronic bronchitis is diagnosed if the patient suffers bronchitis for 3 months out of the year for 2 years.
- Atelectasis commonly occurs in the postoperative period and predisposes individuals to pneumonia.
- Patients with atelectasis should be encouraged to cough and deep-breath and use an incentive spirometer.
- Impending respiratory failure occurs when the patient’s PO 2 decreases toward 60 mm Hg and PCO 2 increases
toward 50 mm Hg.
- The most common cause of CAP is S. pneumoniae. - HIV-related pneumonia is caused by Pneumocystis jirovecii.
- Cough, fever, and crackles are classic signs of pneumonia.
- Septic emboli, which commonly develop from right-sided endocarditis, can form lung abscesses in IV drug
abusers.
- Bronchial tumor obstruction of mucus and secretions can cause a lung abscess.
- There are two forms of TB: TB disease and LTBI.
- TB disease consists of actively growing M. tuberculosis bacteria, symptoms, and infectious potential.
- LTBI consists of inactive M. tuberculosis bacteria, no symptoms, and no infectious potential. However, LTBI can
progress to TB disease at any point during a person’s lifetime.
- Persistent cough, weight loss, night sweats, and hemoptysis are classic signs of TB.
- Immunosuppression caused by infection with HIV increases susceptibility to TB.
- TB is an opportunistic infection that can occur in HIV infection.
ALERT! At a PO2 of approximately 60 mm Hg, oxygen saturation of Hgb dramatically falls. The patient will devel
Pulmonary
Outline
stimulus to breathe, hypoxia becomes the impetus for the patient to take another breath. This is a significant change
in physiological response, which commonly occurs in severe COPD.
In persons who develop long-term chronic hypercapnia, the respiratory center becomes insensitive to accumulation
of CO 2 as a stimulus for breathing. The body changes its breathing stimulus to low oxygen levels (hypoxia), instead
of high CO 2 levels. This often occurs in persons with long-term COPD.
Chronic Hypoxia
The pressure of O 2 gas in the bloodstream is measurable and termed the partial pressure of O 2 (PO 2 ). The ideal PO 2 ranges from 90 mm Hg to 100
mm Hg. Chronic hypoxia is a chronic lack of oxygen that occurs in respiratory dysfunction. The term is often used interchangeably with
hypoxemia, which refers to diminished O 2 levels in the blood. Body tissues vary in their vulnerability to hypoxia; some, such as bone, can
withstand episodes of hypoxia for much longer periods than others, such as the heart, kidney, and brain. For example, the brain can tolerate
hypoxia for only 5 to 6 minutes before brain cells die. The kidney can sustain hypoxia for 20 minutes before nephrons die.
If the PO 2 of tissues falls below a critical level (60 mm Hg), cellular aerobic metabolism ceases and anaerobic metabolism takes over with
formation of lactic acid. Mild hypoxemia causes few symptoms because hemoglobin (Hgb) saturation remains high, at approximately 90%, with
PO 2 levels as low as 70 mm Hg. However, there is a dramatic drop in Hgb saturation of oxygen at a PO 2 of 60 mm Hg. At a PO 2 of 60 mm Hg,
Hgb starts to release all its oxygen molecules, placing the patient in a state of severe hypoxemia. Severe hypoxemia causes behavioral changes,
restlessness, uncoordinated movements, impaired judgment, delirium, and eventually stupor and coma.
The body compensates for hypoxia by increasing ventilation, stimulating pulmonary arteriole vasoconstriction, and having the kidney release
erythropoietin (see Fig. 21-1). Erythropoietin stimulates the bone marrow to synthesize red blood cells (RBCs). Chronic hypoxia causes constant
synthesis of RBCs, a condition called erythropoiesis. Chronic hypoxia also causes pulmonary arterial vasoconstriction; this leads to pulmonary
hypertension, a condition of high blood pressure within the pulmonary arterial system. Pulmonary hypertension develops because in lung
regions where there is lack of oxygen, the arterioles vasoconstrict to limit blood flow to those deoxygenated areas. If there are a large number of
lung areas with chronic hypoxia, then the large areas of vasoconstriction of pulmonary arterioles cause the pulmonary artery to increase in pressure;
this is termed pulmonary hypertension. High pulmonary artery pressure places high resistance against the right ventricle of the heart, which can lead
to right ventricular hypertrophy and eventually excessive strain that leads to right ventricular failure.
Pulmonary
Outline
What is an obstructive disorder? Restrictive disorder?
Obstructive disease is characterized by an increase in resistance to airflow from the trachea and larger
bronchi to the terminal and respiratory bronchioles. The major obstructive lung diseases are asthma, COPD,
and bronchiectasis.
Restrictive pulmonary diseases are those that prevent complete ventilation, diminish total lung capacity,
and impede the opening of all the alveoli. Pneumothorax and pleural effusion are the most common causes
of restrictive respiratory diseases. Lung diseases that damage the lung tissue directly, such as pulmonary
fibrosis and environmental lung disorders, can also cause restrictive disease, as can musculoskeletal
disorders that cause structural alterations of the thoracic cage. Vertebral abnormalities such as kyphosis and
scoliosis can restrict pulmonary function. Immunological-mediated disorders, such as sarcoidosis, cause
restrictive lung disease. Neurological disorders such as muscular dystrophy, myasthenia gravis, and
Guillain–Barré syndrome, all of which can impair full thoracic cage expansion, can also cause a restrictive
pulmonary disorder.
What are the general risk factors for pulmonary disorders/diseases?
Risk Factors
A history of current and past smoking habits should be sought from all patients. If the patient has smoked, the
clinician should ask the patient the number of years he or she has smoked and multiply that number by the number
of packs of cigarettes smoked per day; this yields a smoking history in pack-years. For example, a 76-year-old
patient who has smoked two packs per day since age 16 years has a 120 pack-year smoking history (2 packs per day
× 60 years). If the patient has no smoking history, the clinician should ask about exposure to secondhand smoke.
Occupational exposure to toxic agents should be investigated. Common occupational exposures linked to lung
disease include mineral dust, coal, silica, farming and landscaping materials, and reactive chemicals such as toluene.
Asbestos exposure is a particularly significant risk factor for pulmonary disease. Asbestos was used as a building
material prior to 1980; therefore, construction workers, firefighters, shipyard and power plant workers, mechanics
and others may have been exposed. Ask the patient about exposure to animals, pet dander, molds, pollen, ragweed,
household dust, and cockroaches. Illicit drug use, particularly marijuana, cocaine, and IV drugs, needs to be
discussed. Ask the patient about possible contact with individuals with respiratory infections and exposure to
infectious agents such as tuberculosis (TB).
A history of any respiratory or nonrespiratory disorder should be sought, particularly cardiac disease, HIV
infection, immunosuppressive conditions, cancer, and autoimmune disease such as systemic lupus erythematosus,
scleroderma, or sarcoidosis. A complete list of the patient’s current medications and treatments is needed,
particularly radiation therapy, immunosuppressive agents, steroids, chemotherapeutic agents, beta blockers, and
angiotensin-converting enzyme (ACE) inhibitors. A family history of pulmonary and nonpulmonary disease should
be investigated, particularly TB, asthma, cystic fibrosis, alpha-1 antitrypsin (AAT) deficiency, and heart disease.
Signs/Symptoms/Physical Assessment
What is orthopnea? Clubbing?
o When would you see these
o Both clinical concept pg. 506
Signs and Symptoms
The clinician should use the physical examination techniques of inspection, palpation, percussion, and auscultation
when assessing the patient’s pulmonary system. On inspection, note the patient’s rate, rhythm, and depth of
breathing. Observe the use of intercostals and accessory muscles, symmetrical or asymmetrical expansion of the
chest, and structural abnormalities of the thoracic cage and spine. Observe the patient for dyspnea, which is
CLINICAL CONCEPT
Patients with chronic hypoxia develop pulmonary vasoconstriction, called pulmonary hypertension,
which causes an increased workload for the right ventricle and can lead to right ventricular failure, a
condition known as cor pulmonale.