



Pathology Notes














































































Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
An overview of pathology notes, including the definitions of commonly used suffixes, cellular injury, cellular responses to injury, and inflammation. It also covers the causes and major components of acute inflammation, as well as the consequences of chronic inflammation. useful for students studying pathology or related fields.
Typology: Study notes
1 / 86

This page cannot be seen from the preview
Don't miss anything!
Lesion: structural (or functional) abnormality in an organ, tissue, cell responsible for ill health.
Pathognomonic: a lesion or sign that is specifically distinctive or characteristic of a disease or pathological condition.
Autopsy: postmortem examination of body to determine pathological processes that contributed to death/disease.
Biopsy: the removal and examination of tissue from the living body to establish a precise diagnosis.
Diagnosis: a concise statement or conclusion concerning the nature, cause, or name of a disease.
Differential Diagnosis (“rule-outs”): A list of diagnoses that could account for the history, clinical signs or lesions in a case.
Clinical Diagnosis: Diagnosis based on data obtained from the case history, clinical signs, and physical examination.
Morphologic Diagnosis (lesion diagnosis): A diagnosis based on the predominant lesion(s) in the tissue. it may be macroscopic (gross) or microscopic (histologic) & describes the severity, duration, distribution, location and nature (eg degenerative, inflammatory, neoplastic) of the lesion.
Etiologic Diagnosis: a definitive diagnosis that names the specific cause of the disease.
Disease (Definitive) Diagnosis: a specific diagnosis that states the “name of the disease”.
Eponymous names: An eponymous disease or lesion is named after a person or place associated with it. Syndromes often have eponymous titles.
Anatomic Terminology: ORGAN + OPATHY (disease of an organ; the etiology / pathogenesis is not entirely clear). Hepatopathy - any disease of the liver.
ORGAN + OSIS (noninflammatory disease of an organ, often used if degeneration / necrosis)
ORGAN + ITIS (an inflammatory disease of the organ). Hepatitis - inflammation of the liver.
CELLULAR INJURY: Numerous causes: physical and chemical agents including products of microorganisms. Various mechanisms: disruption, membrane failure, metabolic interference (respiration, protein synthesis, DNA), free radicals. May be reversible, or end in cell death.
Cellular Responses to Injury (important)
Hyperplasia: Hyperplasia is an increase in the number of cells in an organ or tissue, usually resulting in increased mass of the organ or tissue. Hyperplasia takes place if the cell population is capable of dividing. (Neurons lack centromere so it can’t divide)
Physiologic Hyperplasia: hormonal hyperplasia, which increases the functional capacity of a tissue when needed (female breast at puberty and during pregnancy)
Compensatory hyperplasia, which increases tissue mass after damage or partial resection (In individuals who donate one lobe of the liver for transplantation, the remaining cells proliferate so that the organ soon grows back to its original size)
Pathologic Hyperplasia: caused by excesses of hormones or growth factors acting on target cells. Pathologic hyperplasia constitutes a fertile soil in which cancerous proliferation may eventually arise. It’s characteristic response to certain viral infections like papillomaviruses.
Atrophy: reduced size of an organ or tissue resulting from a decrease in cell size and number
Physiologic atrophy is common during normal development, Uterus decreases in size shortly after parturition.
Pathologic atrophy: Decreased workload (atrophy of disuse), Loss of innervation (denervation atrophy like in tongue after hypoglossal nerve injury), Diminished blood supply, Inadequate nutrition, Loss of endocrine stimulation, Pressure.
Metaplasia: is a reversible change in which one differentiated cell type (epithelial or mesenchymal) is replaced by another cell type. It may represent an adaptive substitution of cells that are sensitive to stress by cell types better able to withstand the adverse environment.
The most common epithelial metaplasia is columnar to squamous. As occurs in the respiratory tract in response to chronic irritation. In the habitual cigarette smoker Metaplasia from squamous to columnar type may also occur, as in Barrett esophagus.
The hallmarks of reversible injury are reduced oxidative phosphorylation with resultant depletion of energy stores in the form of adenosine triphosphate (ATP), and cellular swelling caused by changes in ion concentrations and water influx.
Causes of Cell Injury
NECROSIS: is death of tissues following bioenergetic failure and loss of plasma membrane integrity. It Induces inflammation and repair. Causes include ischaemia, metabolic, and trauma.
Types of necrosis: IMPORTANT
Coagulative necrosis in most tissues; firm pale area, with ghost outlines on microscopy
Colliquative (Liquefactive) necrosis is seen in the brain; the dead area is liquefied.
Caseous necrosis is seen in tuberculosis; there is pale yellow semi-solid material.
Gangrene necrosis with putrefaction (decay). It follows vascular occlusion or certain infections and is black.
Fibrinoid necrosis is a microscopic feature in arterioles in malignant hypertension.
Fat necrosis may follow trauma and cause a mass or may follow pancreatitis visible as multiple white spots.
Coagulative necrosis: the commonest form of necrosis and can occur in most organs
Following devitalization (deprive of normal blood supply and nutrients), the cells retain their outline as their proteins coagulate. Ischemia caused by obstruction in a vessel may lead to coagulative necrosis of the supplied tissue in all organs except the brain. The affected tissues exhibit a firm texture A localized area of coagulative necrosis is called an infarct.
Coagulative necrosis. A wedge-shaped kidney infarct (yellow). Microscopic view of the edge of the infarct, with normal kidney (N) and necrotic cells in the infarct (I) showing preserved cellular outlines with loss of nuclei & an inflammatory infiltrate.
Fat necrosis: Fat necrosis may be due to:
Direct trauma to adipose tissue and extracellular liberation of fat Enzymatic lysis of fat due to release of lipases.
Fat necrosis. The areas of white chalky deposits represent foci of fat necrosis with calcium soap formation (saponification) at sites of lipid breakdown in the mesentery.
Gangrene: Gangrene is necrosis with putrefaction (decay) of the tissues. Sometimes because of the action of certain bacteria, notably clostridia
The affected tissues appear black because of the deposition of iron sulphide from degraded haemoglobin
Ischaemic necrosis of the distal part of a limb may proceed to gangrene if complicated by an appropriate infection.
Dry Gangrene: Is usually seen in the toes. As a result of gradual arterial or small vessel obstruction in atherosclerosis or diabetes mellitus
A line of demarcation develops between the gangrenous and adjacent viable tissues.
The dead area drops off. This is a sterile process, and is the common fate of gangrenous toes as a complication of diabetes.
Wet Gangrene: As clostridia are very common in the bowel. Intestinal necrosis is particularly liable to proceed to gangrene.
It can occur as a complication of appendicitis , or incarceration of a hernia if the blood supply is impeded.
Gas gangrene Is the result of infection by Clostridium perfringens
Overview of Inflammation:
Why is inflammation essential to humans (organisms)?
It’s an indicator of disease and to get rid of damaged or necrotic tissues and foreign invaders such as microbes
How inflammation is fundamental to humans (organisms)?
This is fundamentally a protective response, designed to rid the organism of both the initial cause of cell injury (e.g., microbes, toxins) and the consequences of such injury (e.g., necrotic cells and tissues).
Without inflammation, what can happen to humans (organisms)?
Infections would go unchecked, Wounds would never heal, Injured tissues might remain permanent festering sores.
Important
Inflammation is a complex reaction in living tissues that consists mainly of responses of blood vessels and leukocytes. The inflammatory response coordinates the reactions of vessels, leukocytes, and plasma proteins to achieve this goal.
Vasodilation in which the wall of vessels become leaking Endothelial contraction led to leakage of fluid and substances necessary to fight the cause.
Do Inflammation contribute to a variety of diseases?
YES, Inflammation may contribute to a variety of diseases that are not thought to be primarily due to abnormal host responses. For instance, chronic inflammation may play a role in:-
Atherosclerosis, type 2 diabetes, rheumatoid arthritis, lung fibrosis, degenerative disorders like Alzheimer disease, and cancer.
In recognition of the wide-ranging harmful consequences of inflammation, the lay press has rather melodramatically referred to it as “ the silent killer.”
Causes of acute inflammation (important)
Microbial infections e.g. (bacterial, viral, fungal, parasitic) and microbial toxins
Tissue necrosis , e.g., ischemic infarction.
Physical agents, e.g., trauma, ionizing radiation, heat, cold (freeze bites)
Chemicals , e.g., corrosives, acids, alkalis, reducing agents.
Immune reactions (also called hypersensitivity reactions), e.g., parasites, tubercle bacilli
The most important leukocytes in typical inflammatory reactions are the ones capable of phagocytosis, namely neutrophils and macrophages.
These leukocytes ingest and kill bacteria and other microbes and eliminate necrotic tissue and foreign substances. Leukocytes also produce growth factors that aid in repair.
In most forms of acute inflammation neutrophils predominate in the inflammatory infiltrate during the first 6 to 24 hours. Neutrophils are multilobed nucleus, purple fine lysosomes granules, bluish cytoplasm and highly active & mobile.
In certain bacterial infections the cellular infiltrate is dominated by continuously recruited neutrophils for several days
In viral infections, lymphocytes may be the first cells to arrive
In some hypersensitivity reactions and parasite , eosinophils may be the main cell type.
Important
The cardinal signs of acute inflammation (important)
Redness (rubor): An acutely inflamed tissue appears red, for example skin affected by sunburn , cellulitis due to bacterial infection or acute conjunctivitis. This is due to dilatation of small blood vessels within the damaged area.
Heat (calor): Increase in temperature is seen only in peripheral parts of the body, such as the skin. It is due to increased blood flow (hyperaemia) through the region, resulting in vascular dilatation and the delivery of warm blood to the area.
Swelling (tumour): Swelling results from oedema. The accumulation of fluid in the extravascular space as part of the fluid exudate
Pain (dolor): For the patient, pain is one of the best-known features of acute inflammation. It results partly from the stretching and distortio n of tissues due to inflammatory oedema and from pus under pressure in an abscess cavity.
Some of the chemical mediators of acute inflammation, including bradykinin , the prostaglandins and serotonin , are known to induce pain.
Loss of function (functio laesa): Loss of function, a well-known consequence of inflammation. Movement of an inflamed area is consciously and reflexly inhibited by pain , while severe swelling may physically immobilise the tissues.
Outcomes of Acute Inflammation (important)
Complete resolution
Healing by connective tissue replacement (fibrosis) leaving a scar.
Progression of the response to chronic inflammation
Suppurative or purulent inflammation; abscess:
Is characterized by the production of large amounts of pus or purulent exudate consisting of :-
Certain bacteria (e.g., staphylococci) produce this localized suppuration and are therefore referred to as pyogenic (pus-producing) bacteria.
Abscesses : are localized collections of purulent inflammatory tissue caused by suppuration buried in a tissue, an organ, or a confined space.
They are produced by deep seeding of pyogenic bacteria into a tissue. Once pus begins to accumulate in a tissue, it becomes surrounded by a ‘ pyogenic membrane’ consisting of sprouting (new buds) capillaries, neutrophils and occasional fibroblasts. Such a collection of pus is called an abscess. Bacteria within the abscess cavity are relatively inaccessible to antibodies and to antibiotic drugs.
Antibioma is a chronic abscess formed because of incomplete treatment of an infection by using antibiotics without incision and drainage. (Incomplete draining)
Ulcers: Is a local defect, or excavation, of the surface of an organ or tissue that is produced by the sloughing (shedding) of inflamed necrotic tissue
Ulceration can occur only when tissue necrosis and resultant (a force) inflammation exist. It is most commonly encountered in:
Inflammation, even if localized, is associated with cytokine induced systemic reactions. That are collectively called the acute-phase response.
The cytokines TNF, IL-1, and IL-6 are important mediators of the acute-phase reaction ; other cytokines, notably interferons, also contribute.
Fever: Characterized by an elevation of body temperature, usually by 1°C to 4°C. (above 37.5, if above 42 then death)
Substances that induce fever are called pyrogens and include bacterial products (exogenous pyrogens, e.g., LPS). Cytokines principally IL-1 and TNF (called endogenous pyrogens). Exogenous pyrogens act by stimulating immune cells to release IL-1 and TNF. Which upregulate cyclooxygenases, the enzymes that synthesize prostaglandins
Cells that respond to IL-1 and TNF are Vascular cells and perivascular cells of the hypothalamus.
Prostaglandins released by these cells, especially PGE2, stimulate the production of neurotransmitters by the hypothalamus. That reset the body’s steady-state temperature to a higher level by reducing heat loss (via vasoconstriction).
NSAIDs, including aspirin, reduce fever by inhibiting prostaglandin synthesis.
Acute-phase Proteins
Elevated levels of acute-phase proteins, which are plasma proteins, mostly synthesized in the liver , whose plasma concentrations may increase several hundred–fold as part of the response to inflammatory stimuli.
Three of the best known of these proteins are (important)
C-reactive protein (CRP) Fibrinogen Serum amyloid A (SAA) protein
Synthesis of these molecules in hepatocytes is stimulated by cytokines:
Especially IL-6 (for CRP and fibrinogen), IL-1 or TNF (for SAA)
Action of acute phase proteins:
They bind to microbial cell walls. They may act as opsonin and fix complement. They also bind chromatin , possibly aiding in clearing necrotic cell nuclei.
Fibrinogen binds to red cells and causes them to form stacks (rouleaux) that sediment more rapidly at unit gravity than do individual red cells.
This is the basis for measuring the erythrocyte sedimentation rate (ESR ) as a simple test for the systemic inflammatory response, caused by any stimulus. The normal range is 0-22 mm/hr for men and 0-29 mm/hr for women.
Chronic Inflammation
Chronic inflammation is inflammation of prolonged duration (weeks or months) in which inflammation, tissue injury, and attempts at repair coexist
Rheumatoid arthritis, atherosclerosis, tuberculosis, and pulmonary fibrosis and purely degenerative, such as Alzheimer disease. It has been implicated in the progression of cancer.
Causes of Chronic Inflammation
Persistent infections by microorganisms that are difficult to eradicate , such as mycobacteria, and certain viruses, fungi, and parasites
Immune-mediated inflammatory examples of such diseases are rheumatoid arthritis and multiple sclerosis
Prolonged exposure to potentially toxic agents , either exogenous or endogenous. Atherosclerosis by endogenous toxic plasma lipid components.
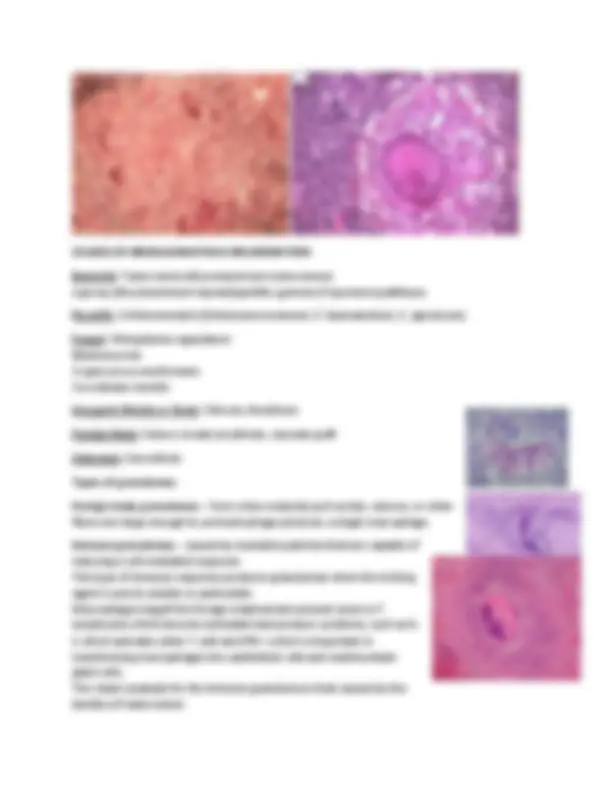
Granulomatous Inflammation: a distinctive pattern of chronic inflammation. It is a protective response to chronic infection or foreign material, preventing dissemination and restricting inflammation.
Granuloma is a microscopic aggregation of macrophages that are transformed into epithelium-like (epithelioid) appearance cells surrounded by a collar of mononuclear leukocytes, principally lymphocytes and occasionally plasma cells.
Fibrous connective tissue often surrounds granulomas (remodeling of tissue) Areas within the granuloma can undergo necrosis (prototype: caseous necrosis, cheese-like in tuberculosis ). Necrosis can lead to calcification or liquefaction and formation of a cavern if drained.
Tuberculosis is the prototype of the granulomatous diseases. But also Leprosy, Leishmaniasis, Schistosomiasis, Sarcoidosis, Actinomycosis. Some Autoimmune diseases such as rheumatoid arthritis and Crohns disease are also associated with granulomas.
The prototype of the immune granuloma is that caused by infection with Mycobacterium tuberculosis. In this disease the granuloma is referred to as a tubercle
It is often characterized by the presence of central caseous necrosis
Epithelioid cells fuse to form giant cells containing 20 or more nuclei. The nuclei arranged either peripherally ( Langhans-type giant cell ) or haphazardly ( foreign body-type giant cell). These giant cells can be found either at the periphery or the center of the granuloma.
Bacterial : Tuberculosis (Mycobacterium tuberculosis) Leprosy (Mycobacterium leprae)Syphilitic gumma (Treponema pallidum)
Parasitic : Schistosomiasis (Schistosoma mansoni, S. haematobium, S. japonicum)
Fungal : Histoplasma capsulatum Blastomycosis Cryptococcus neoformans Coccidiodes immitis
Inorganic Metals or Dusts : Silicosis, Berylliosis
Foreign Body : Suture, breast prosthesis, vascular graft
Unknown : Sarcoidosis
Types of granulomas :
Foreign body granulomas – form when material such as talc, sutures, or other fibers are large enough to preclude phagocytosis by a single macrophage.
Immune granulomas - caused by insoluble particles that are capable of inducing a cell-mediated response. This type of immune response produces granulomas when the inciting agent is poorly soluble or particulate. Macrophages engulf the foreign material and present some to T lymphcytes which become activaded and produce cytokines, such as IL- 2 which activates other T cells and IFN-γ which is important in transforming macrophages into epithelioid cells and multinucleate giant cells. The classic example for the immune granuloma is that caused by the bacillus of tuberculosis