Download Pathophysiology Concept Maps and more Study notes Pathophysiology in PDF only on Docsity!
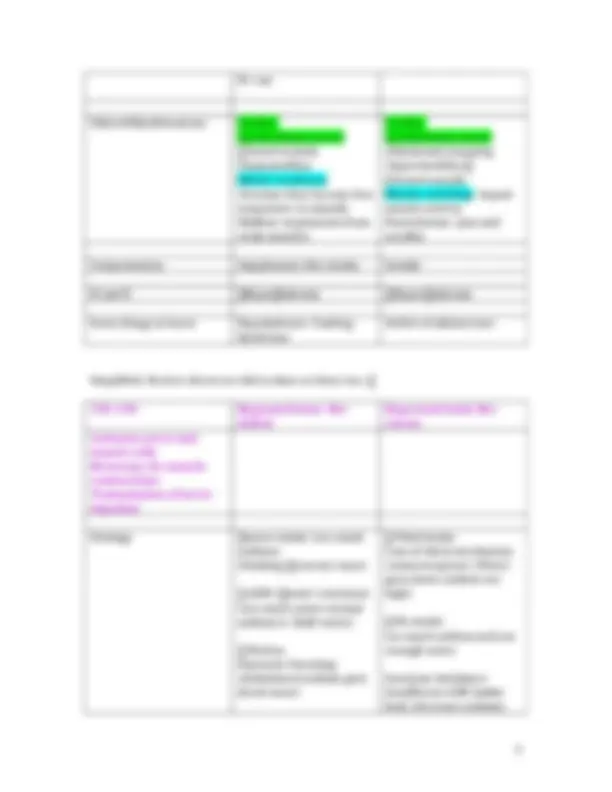
Addison's disease and Cushing's Disease Cortisol level
Addison’s (need to "add" hormone)
Cushing’s (have extra "cushion" of hormones)
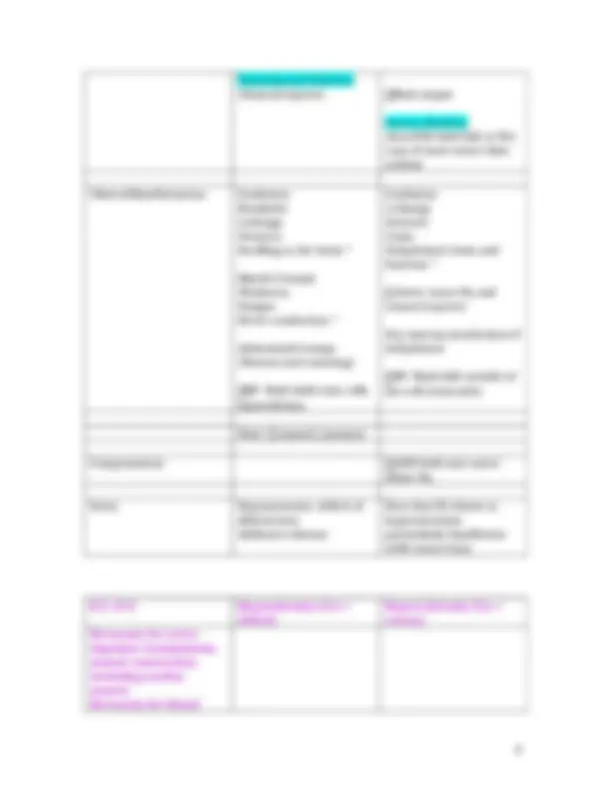
Corticoids ^ Risk of infection High risk of infection High risk of infection Stress response Poor stress response Poor Stress response Weight Weight loss fatigue Moon face, buffalo hump, obese Problems eating/bruising of skin
Anorexia, Nausea, Diarrhea
Striae, bruising of skin (Ecchymoses) Tension, syncope, glucose Hypotension syncope Hypertension, Glucose formation Color of the skin, mental status and delayed healing
Hyperpigmentation Fatigue, weakness delayed healing Hypercalcemia Hypocalcemia Hypoglycemia Hyperglycemia Hyperkalemia Hypokalemia Hyponatriemia Hypernatriemia Hypovolemia Hypervolemia
Type 1 Diabetes Type 2 Diabetes Age of Onset Children and Young Adults Older adults usually Onset Acute Insidious Etiology Autoimmune destruction Family History
Familial
Body Weight Thin Obesity/ Obese Plasma Insulin Very Low Decreased or Normal Ketoacids Frequent Less common/ none
Hypothyroidism- Hashimoto’s Tyoriditis- Decrease in cell metabolism
Hyperthyroidism- Graves Disease (Whys due to the increase in cell metabolism) Levels of T3 and T4 Low High Metabolic Rate Low High Goiters Endemic Goiter Graves disease Goiter Skin Pale cool edema Flushed warm skin Temp Balance Cold intolerance= think ice, cold day, snow
Heat intolerance= think sun or hot day Eyes No changes Exophthalmos- bulging of eyes
Cardiovascular HR enlarged heart HR BP Nervous System Lethargic, slow Restlessness, nervous and tremors. Body Weight weight appetite thin appetite
vol (dehydration) Fluid deficit
Vol (edema) Fluid excess BP Heart rate Temp and Lungs Normal but (Pulmonary congestion, cough and rales) Skin Poor skin turgor Cap refill Dry mucous membranes
Edema (Pale gray red skin) because of Fluid cap and skin Weight Mental Status Tired, fatigue, Irritable, weakness, dizziness, stupor
Confused Tired/lethargy (hypovolemia Seizures Pulses Weak, rapid, thready Bounding and slow H&H ^ Electrolytes Urine specific gravity ^
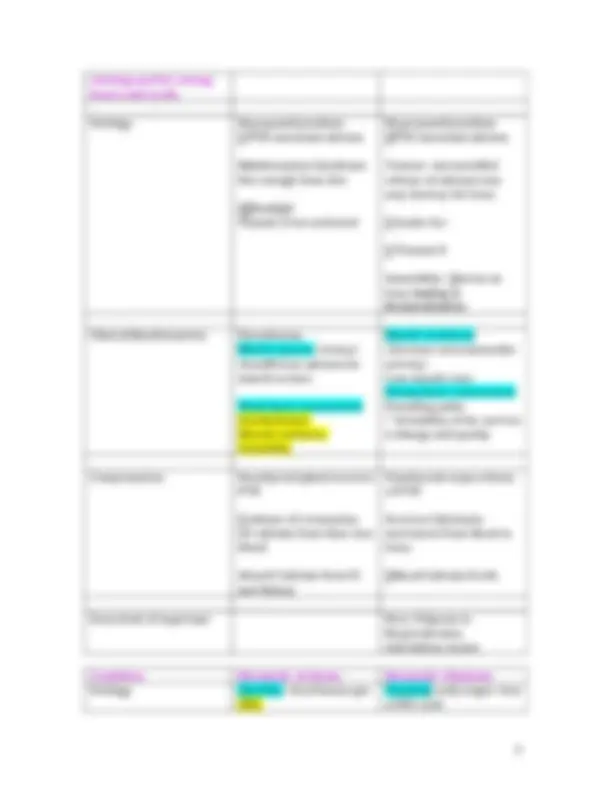
3.5- 5.0 Hypokalemia K+ deficit Hyperkalemia K+ excess Necessary for transmission of electric impulses, particarly in nerve, heart, skeletal, intestinal and lung tissue.
Etiology intake of K+ (how much you take in
output of K+ Vomiting and Diarrhea (lose water lose potassium)
Alkalosis
K+ in
output of K+ Renal Failure- Not getting rid of Potassium. (kidney failure)
Acidosis K+ out H+ in
Cell lysis or hemolysis ICF to ECF
Vomiting and Diarrhea (Osmoreceptors) fluid output
watery diarrhea (loss H20 hold Salt or Na) Loss of more water than sodium
Clinical Manifestations Confusion Headache Lethargy Seizures Swelling to the brain ^
Muscle Cramps Weakness Fatigue Nerve conduction ^
Abdominal Cramps (Nausea and vomiting)
BP- fluid shifts into cells hypovolemia.
Confusion Lethargy Seizures Coma Dehydrated, brain and function ^
thirst (more Na and osmoreceptors)
Dry mucous membranes if dehydrated
BP- fluid shift outside of the cell (extra info)
Note: osmotic pressure
Compensation ADH hold onto water dilute Na.
Extra Hyponatremia- deficit of aldosterone Addison’s disease
Note that DI relates to hypernatremia particularly Insufficient ADH (water loss)
8.5-10.5 Hypocalcemia (Ca++ deficit)
Hypercalcemia (Ca++ excess) Necessary for nerve impulses transmission, muscle contraction, including cardiac muscle Necessary for blood
clotting and for strong bones and teeth.
Etiology Hypoparathyroidism PTH intestinal calcium
Malabsorption Syndrome Not enough from diet
Sunlight Vitamin D not activated
Hyperparathyroidism PTH intestinal calcium
Tumors- uncontrolled release of calcium ions may destroy the bone
intake Ca+
Vitamin D
Immobility- stress on bone leading to demineralization
Clinical Manifestations Paresthesias Muscle spasms (tetany) (Insufficient calcium for muscle action)
Weak heart contractions Dysrhythmias Mental confusion Irritability
Muscle weakness- (decrease neuromuscular activity) Loss muscle tone Strong heart contractions Bounding pulse ^ Irritability of the nerves) Lethargy and apathy
Compensation Parathyroid gland secretes PTH
release of (resorption of) calcium from bone into blood
Absorb Calcium from GI and Kidney
Parathyroid stops release of PTH
Secretes Calcitonin- movement from blood to bone.
blood Calcium levels
Extra kind of important Note: Polyuria in Hypercalcemia. And kidney stones
Condition Metabolic Acidosis Metabolic Alkalosis Etiology Diarrhea- bicarbonate gut DKA
Vomiting early stages- loss of HCL acid
Depress respirations
Neuromuscular Dx Control area
Chest trauma Cortisol diaphragm
(Won’t be breathing as deeply hold onto CO2) Airway obstruction
Pain- causes problems
Fever- metabolic rate respiratory
Initial State of pulmonary embolus
Pathophysiology Excess of carbonic acid; CO2 retention from alveolar hypoventilation
Deficit of carbonic acid; increased CO2 loss due to alveolar hyperventilation
Clinical Manifestation Same as Metabolic acidosis
Same as Metabolic alkalosis
ABG findings= ROME RO = opposite
pH PaCO
pH PaCO
How is the Body Trying to Help or Compensate
Increase renal excretion of H+ and HCO reabsorption Excrete more H+ reabsorp HCO H+ for K+ Too much K
Kidneys decrease H+ excretion
Slow HCO3 reabsorption Reabsorp less bicarbonate H+ for K+ Decreased Serum K+
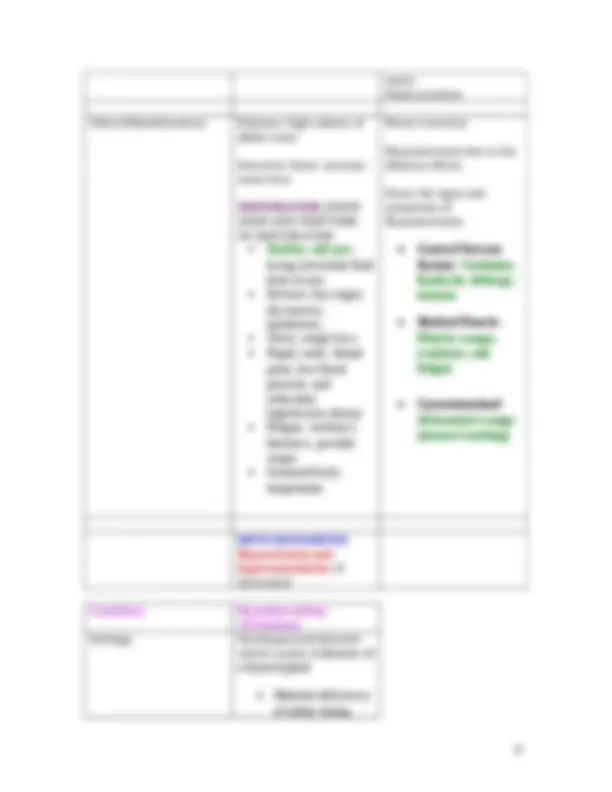
DI SIADH
Def. Decreased production of ADH
Excess production of ADH
Etiology Adenoma Head injury or surgery Sometimes ADH secretion is okay but kidney tubules do not respond to ADH = genetic problem or drug reaction
Maybe triggered by stress
Paraneoplastic (ectopic tumor)
Pathogenesis Kidney tubules are unable to reabsorb water
Excess production of ADH Kidney tubules reabsorb excessive amounts of
water Fluid retention
Clinical Manifestations Polyuria- high volume of dilute urine
Excessive thirst- increase water loss
DEHYDRATION : KNOW SIGNS AND SYMPTOMS OF DEHYDRATION Sunken, soft eyes - losing interstitial fluid from tissues Decease skin turgor, dry mucous membranes Thirst, weight loss- Rapid, weak, thread pulse, low blood pressure, and orthostatic hypotension (dizzy) Fatigue, weakness, dizziness, possible stupor Increased body temperature
Water retention
Hyponatriemia due to the dilution effects.
Know the signs and symptoms of Hyponatriemia
Central Nervous System: Confusion, headache, lethargy, seizures
Skeletal Muscle: Muscle cramps, weakness, and fatigue
Gastrointestinal: Abdominal cramps (nausea/vomiting)
NOTE ON DIABETES:
Hypovolemia and hyperosmolarity (if untreated)
Condition Hypothyroidism (Cretinism) Etiology Developmental disorder which consist of absence of a thyroid gland
o Maternal deficiency of iodine during
Increased capillary hydrostatic pressure- Increased blood volume, Vasoconstriction, & Increased blood pressure
Decreased plasma proteins (albumin)- Poor diet, Released through urine (proteinuria), & liver disease/dysfunction
Lymphatic Obstruction- Tumor, Infection in lymph node, & surgical removal of nodes
Increased capillary permeability- Chemical mediators, Inflammatory response, & Infection
Increased hydrostatic pressure on the venous end- Blockage or narrowing on the venous end
Go over questions we went through in class powerpoint
Osmosis and Diffusion
Osmolarity 3 types Hypo-osmolar Hyper-osmolar Iso-osmolar
Know electrolytes (Sodium, Potassium and Calcium)
Know Acid Base Balance and the Acid Base Imbalances
For Endocrine Know Hypo and Hyperthyroidism and the diseases in those Know Hypoparathyroid and Hypoparathyroid
Know the Growth Hormones alterations: Dwarfism, Gigantaism, Acromegaly
Know Cushing and Addison’s Disease.
Alterations related to Antidiuretic Hormone
Know important diagnostic tests
Know Hypo and Hyper Aldosteronism
Know Pheochromocytoma
Know Diabetes Type 1 and Type 2 The 3P’s
Diagnostic Findings
Know the Acute Complications for Type 1 and Type 2
Know the complications of Chronic Hyperglycemia
Know Gluconeogenesis, Glycogenolysis and Glycolysis
Know Stress ANS SNS And the diagram picture.
Know Stress Response