Download Neurological and Endocrine Disorders: A Comprehensive Overview and more Study Guides, Projects, Research Nursing in PDF only on Docsity!
PATHOPHYSIOLOGY – FINAL EXAM STUDY GUIDE
NEURO – TERMS TO KNOW
CONSCIOUSNESS
- The state of being aware, or perceiving physical facts or mental concepts; a state of general wakefulness and responsiveness to environment; a functioning sensorium. [L. conscio, to know, to be aware of]
- totally aware of surrounding activities and incoming stimuli
- oriented to time, place, and people
- person can respond quickly and appropriately to questions, commands, or events.
- Various levels of reduced consciousness may present as o Lethargy o Confusion o Disorientation o memory loss o unresponsiveness to verbal stimuli o difficulty in arousal
- Glasgow Coma Scale o Used for assessing LOC
- Coma o Most serious level of loss of consciousness o Affected person does not respond to stimuli (pain, or verbal) o Some reflexes may still be present
- Deep coma o Loss of all reflexes o Fixed and dilated pupils o Slow and irregular pulse and respirations AROUSAL
- Reticular Activating System
- determines the degree of arousal or awareness of the cerebral cortex
- The pons and medulla influence the brain's awareness of the incoming pain stimuli o PONS – composed of bundles of both afferent (incoming) and efferent (outgoing) fibers o MEDULLA ▪ contains vital control centers that regulate respiratory and cardiovascular function ▪ contains the coordinating centers that govern coughing, swallowing, vomiting VEGETATIVE STATE - Loss of awareness and mental capabilities - Results from diffuse brain damage AMNESIA
- Loss of memory CONVULSION
- sudden, involuntary movement with loss of awareness, caused by uncontrolled neuronal discharge in the brain. TONIC - In a state of continuous unremitting action ; denoting especially a muscular contraction. 2. Invigorating; increasing physical or mental tone or strength. CLONIC/CLONIC STATE/CLONIC SPASM
- Relating to or characterized by clonus
- Movement marked by repetitive muscle contractions and relaxations in rapid succession.
- Alternate involuntary contraction and relaxation of a muscle DYSPHASIA
- Difficulty comprehending language or speaking; partial impairment of communicating ability - Less severe form of aphasia - Caused by damage to the brain APHASIA - Inability to comprehend or express language; total loss of communicating ability
- Receptive—damage to Wernicke’s area
- Expressive—damage to Broca’s area
- Mixed, global—damage to both areas or to the fibers and tracts between them PARESIS
- Muscle weakness
- Mild paralysis OTORRHEA
- Leaking of CSF from the ear
- Occurs with fractures
- Tearing of meninges o Allows CSF to pass out of the subarachnoid space SEIZURES Seizures (look up types of seizures) ● Generalized o Absence seizures (petit mal) ▪ Lapses of awareness lasting only a few seconds ▪ Appear without warning/end abruptly ▪ More common in children ▪ Are frequently so brief, they go undetected o Tonic-clonic (grand mal) ▪ Most common ▪ Begin with stiffening of limbs (tonic phase) ▪ Followed by jerking of the limbs/face (clonic phase) o Myoclonic ▪ Rapid, brief contractions of bodily muscles ▪ Occur at the same time on both sides of body ▪ Usually involve one arm or a foot ▪ “sudden jerk” movements or “clumsiness”
ALZHEIMER’S DISEASE (AD) (tends to be more psychosocial)(can be considered primary) ● Progressive cortical atrophy o Neurofibrillary tangles and plagues o ACh deficit caused by loss of neurons ● No definite diagnostic tests available o Exclusion of other disorders o Careful medical and psychological history ● Specific cause unknown o Repetitive DNA sequences on different chromosomes have been associated with AD. ● Five stages o Pre-clinical stage o Early stage o Mild stage o Moderate stage o Severe stage ● The five “A”s o Anomia – inability to remember names of things o Apraxia – misuse of objects due to failure to identify them o Agnosia – inability to recognize familiar objects, tastes, sounds, and other sensations o Amnesia – memory loss o Aphasia – inability to express language ALZHEIMER’S DISEASE (AD) - Signs and symptoms ● Extend over 10 to 20 years ● Behavioral changes o Irritability, hostility, mood swings ● Gradual loss of memory and lack of concentration ● Impaired learning, poor judgment ● Decline of cognitive function, memory, language ● Change in food intake ● Inability to recognize family, lack of environmental awareness, incontinence, inability to function INCREASED INTRACRANIAL PRESSURE ● Brain is encased in rigid, nonexpendable skull. ● Fluids, blood, and CSF are not compressible. ● Increase in fluid or additional mass causes increase in pressure in the brain o Ischemia and eventual infarction of brain tissue ● Increased ICP is common in many neurological problems. o Brain hemorrhage, trauma, cerebral edema, infection, tumors, abnormal circulation of CSF ● LOC change o may be alert, but not oriented o changes in pulse ▪ could be rapid or slow o changes in BP ▪ wide pulse pressure
o Cushing’s Triad ▪ Hypertension (with widening pulse pressure) ▪ Bradycardia ▪ Respiratory depression
- Early signs—if cause is not removed o Decreasing level of consciousness or decreased responsiveness (lethargy) o Decreased pupillary responses ▪ Pupils – fixed and dilated o Severe headache ▪ From stretching of dura and walls of large blood vessels o Vomiting ▪ Often projectile, not associated with food intake ▪ Result of pressure stimulating the emetic center in the medulla o Papilledema ▪ Caused by increased ICP and swelling of the optic disc HUNTINGTON’S DISEASE
- Inherited disease o Autosomal dominant gene ▪ Carried on chromosome 4
- Does not usually manifest until individual is older than 40 years
- Progressive atrophy of brain
o Dysarthria o Chewing and swallowing become difficult. ▪ Prolonging eating time ▪ Recurrent drooling o Face might resemble a mask ▪ Blinking of eyelids reduced ▪ Blank, staring face ▪ Impairs communication o Autonomic dysfunction ▪ Urinary retention ▪ Constipation o Orthostatic hypotension ▪ Threat of falls increases o Urinary tract and respiratory tract infections are common complications. o Dementia develops late in course of disease
- Treatment o Removal of cause, if known o Dopamine replacement therapy ▪ Levodopa—dopamine precursor o Anticholinergic drugs o Speech and language pathologist o Physical therapy o Occupational therapy o Improves balance, coordination o Monitoring and treatment of respiratory and urinary tract infections Transient Ischemic Attacks (TIAs) = “small strokes” - precursor to CVA ● May occur singly or in a series ● Result from temporary localized reduction of blood flow in the brain o Partial occlusion of an artery o Atherosclerosis o Small embolus ▪ clump that broke off from another part of the body ▪ can be blood, fat, protein o Vascular spasm o Local loss of autoregulation ● Signs and symptoms o Difficult to diagnose after the attack o Directly related to location of ischemia o Intermittent short episodes of impaired function ▪ e.g., muscle weakness in arm or leg o Visual disturbances o Numbness and paresthesia in face o Transient aphasia or confusion may develop. ▪ Repeated attacks may be a warning sign for obstruction related to atherosclerosis. CEREBROVASCULAR ACCIDENT (CVA)
- A CVA (stroke) is an infarction of brain tissue that results from lack of blood. o Occlusion of a cerebral blood vessel o Rupture of cerebral vessel
- 5 minutes of ischemia causes irreversible nerve cell damage. o Central area of necrosis develops o All function lost o Surrounded by an area of inflammation. this zone will regain function following healing. LEFT HEMISPHERE CVA
- Right sided weakness/hemiplegia
- Aphasia
- Slow performance
- Visual field deficits RIGHT HEMISPHERE
- Left sided weakness/hemiplegia
- Spatial-perceptual deficits o Increased vulnerability to accidents
- Tends to minimize problems
- Short attention span
- Impaired judgement
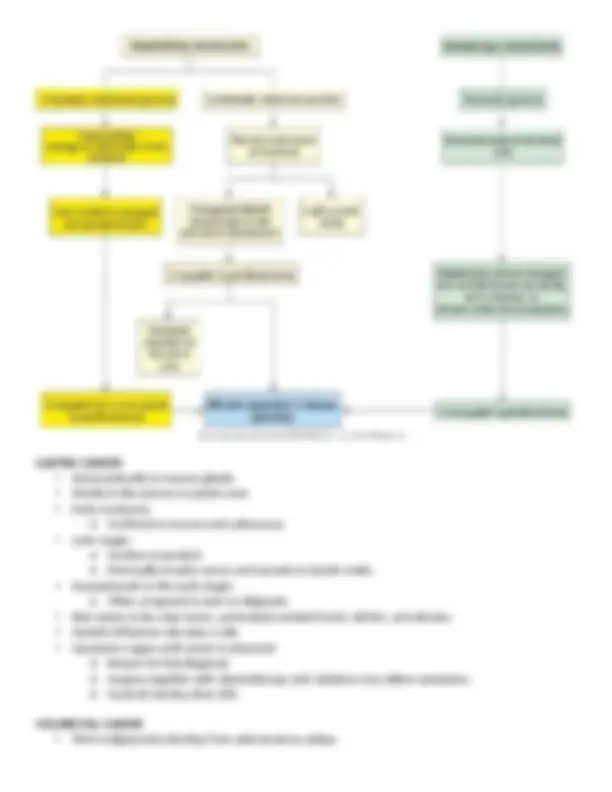
- Impaired time concept TYPES OF CVAs
- Occlusion of an artery by an atheroma o Atheroma = fatty deposits and scarring that leads to tissue breakdown of the artery walls o Often develop in large arteries o Can trigger the formation of thrombosis ( THROMBUS )(blood clot) o Onset is gradual o May be preceded by transient ischemic attacks (TIAs)
- Sudden obstruction caused by an embolus ( EMBOLUS ) o Lodging in a cerebral artery o Localized unless multiple emboli are present
- Intracerebral hemorrhage ( HEMORRHAGE ) o Caused by rupture of a cerebral artery in patient with severe hypertension ▪ Effects are evident in both hemispheres. ▪ Complicated by secondary effects of bleeding Types of CVAs
Infections – BACTERIAL MENINGITIS ● Different age groups are susceptible to infection by different causative organisms. o May be secondary to other infections ● Children and young adults o Neisseria meningitis or meningococci o Classic meningitis pathogen o Frequently carried in the nasopharynx of asymptomatic carriers o Spread by respiratory droplets o Occurs more frequently in late winter and early spring ● Signs and symptoms o Sudden onset is common. o Severe headache o Back pain o Photophobia o Nuchal rigidity (neck stiffness) o Kernig sign ▪ Severe stiffness of the hamstrings causes an inability to straighten the leg when the hip is flexed to 90 degrees. o Brudzinski sign ▪ Severe neck stiffness causes a patient's hips and knees to flex when the neck is flexed. o Vomiting, irritability, lethargy, fever, chills with leukocytosis o Progression to stupor or seizures ● AUTOMATIC PRECAUTIONS o only way to confirm Dx is through CSF analysis Patient with meningitis will still be able to communicate through discomfort Encephalitis (on the brain tissue)(can be seen on a CAT scan) ● Infection of the parenchymal or connective tissue in the brain and spinal cord o Necrosis and inflammation develop in brain tissue.
▪ Result in some permanent damage ● Infection may include meninges. ● Usually of viral origin o May be caused by other organisms ● Early signs o Severe headache, stiff neck, lethargy, vomiting, seizures, fever ● Patient will be completely shut down ● Western equine encephalitis o Arboviral infection spread by mosquitoes o More frequent in summer months o Common in young children ● St. Louis encephalitis o Affects older persons more seriously than younger individuals ● West Nile fever o Caused by a flavivirus o Spread by mosquitoes ● Neuroborreliosis (Lyme disease) o Caused by Borrelia burgdorferi o Transmitted by ticks o Typical bull’s-eye lesion—sore throat, dry cough, fever, headache, cardiac arrhythmias, neurological abnormalities o Antimicrobial therapy ● Herpes simplex encephalitis o Occurs occasionally o Spread from herpes simplex I o Extensive necrosis and hemorrhage in the brain Multiple Sclerosis (MS) ● Progressive demyelination of neurons in the brain, spinal cord, and cranial nerves ● Disease progresses in stages (4-5 stages) ● Progressive, intermittent lost of motor function ● Different types of MS o Variation in effects, severity, and progression ● Loss of myelin interferes with conduction of impulses in affected fibers o May affect motor, sensory, and autonomic fibers o Occurs in diffuse patches in the nervous system o Early symptoms include: ▪ Numbness ▪ Weakness in legs ▪ Visual problems Amyotrophic Lateral Sclerosis (ALS) ● Also referred to as Lou Gehrig’s disease ● No identified cause o Genes on various chromosomes have been linked to the disease. ● Progressive degenerative disease affecting upper motor neurons in the cerebral cortex and lower motor neurons in brainstem and spinal cord ● No indication of inflammation around the nerves
● Laceration or compression of brain tissue ● Rupture or compression of cerebral blood vessels ● Damage because of rough or irregular inner surface of the skull ● Movement of lobes against each other Secondary injuries ● Result from additional effects of cerebral edema, hemorrhage, hematoma, cerebral vasospasm, infection, ischemia related to systemic factors COUP/CONTRACOUP
- Coup – direct impact site - Contracoup – secondary injury on the opposite side away from primary injury BRAIN TUMORS (CANCER)
- Space-occupying lesions that cause increased ICP
- Benign and malignant tumors can be life-threatening. o Unless accessible and removable
- Gliomas form the largest category of primary malignant tumors. o Classified according to cell derivation and location of the tumor
- Tumors in the meninges or pituitary gland cause similar neurological effects.
- Primary malignant tumors rarely metastasize outside the CNS.
- Secondary brain tumors o Metastasize from breast or lung tumors o Cause effects similar to those of primary brain tumors
- Pathophysiology o Primary malignant brain tumors ▪ Usually no well-defined margins ▪ Invasive and have irregular projections into adjacent tissue ▪ Difficult to remove completely o Usually inflammation around the tumor
- Occurrence o Brainstem and cerebellar tumors common in young children o Adults—occur more frequently in the cerebral hemispheres
- Signs and symptoms
o Site of tumor determines focal signs o Seizures often first sign ▪ Surrounding inflammation stimulates neurons to discharge spontaneously o Headaches (increased ICP), vomiting, lethargy, irritability, personality and behavioral changes, possible unilateral facial paralysis or visual problems o Do not cause systemic signs of malignancy ▪ Will cause death before they cause general effects
- Treatment—may cause damage to normal CNS tissue o Surgery if tumor is accessible o Chemotherapy and radiation (many are radioresistant) Rabies
- Viral—transmitted by: o Bite of rabid animal o Transplantation of contaminated tissues
- Virus travels along peripheral nerves to CNS
- Headache and fever, nervous hyperirritability, sensitivity to touch, seizures
- Virus also travels to salivary glands o Difficulty swallowing o Fear of fluids
- Respiratory failure, death Herpes zoster (shingles)
- Caused by varicella-zoster virus in adults o Can occur years after primary infection of varicella (chickenpox)
- Usually affects cranial nerve or one dermatome
- Pain, paresthesia, vesicular rash o If antiviral drugs started within 48 hours of onset, pain is significantly reduced
- Lesions and pain persist for several weeks. o Postherpetic pain may persist for months to years in some cases.
- Vaccine available for those 60 years or older GASTROINTESTINAL SYSTEM DISORDERS MELENA - Passage of tarry stools, due to the presence of blood altered by the intestinal juices.
- results from significant bleeding that has occurred higher in the digestive tract; the hemoglobin has been acted on by intestinal bacteria, causing the dark color. HEMATEMESIS
- Vomiting blood that resembles “coffee grounds”
- a brown, granular material resulting from the partial digestion in the stomach of protein in the blood
- bright red blood = coming from upper GI
- yellow/green vomit = bile (enzymes and hormones) HEMATOCHEZIA
- Passage of bloody stools (in contradistinction to melena, or tarry stools)
● Obstruction promotes rapid reproduction of intestinal bacteria. o Some produce endotoxins. o Affected wall becomes necrotic and more permeable o Bacteria and toxins leak into peritoneal cavity (peritonitis) or into blood (bacteremia and septicemia). ● Perforation of the necrotic segment may occur. o Generalized peritonitis and septic shock ● Functional obstructions or paralytic ileus from: o Abdominal surgery (follows surgery) o Spinal shock following spinal cord injuries o Inflammation related to severe ischemia o Pancreatitis, peritonitis, infection in the abdominal cavity o Hypokalemia o Mesenteric thrombosis o Toxemia ● Mechanical obstruction from: o Adhesions that twist or constrict intestine o Hernias o Strictures caused by scar tissue o Masses—tumors or foreign bodies o Intussusception o Volvulus o Hirschsprung’s disease o Gradual obstruction from chronic inflammatory conditions ● Mechanical obstruction of small intestine o Severe colicky abdominal pain o Intermittent bowel sounds can be heard. ● Paralytic ileus o Pain is steady. o Bowel sounds decrease or are absent. ● Vomiting and abdominal distention o Occurs quickly with obstruction of small intestine o Vomiting is recurrent, eventually with bile-stained content ● Obstruction of the small intestine is a medical emergency! ● Obstruction of large intestine o Develops slowly, with mild signs o Constipation o Mild abdominal pain, followed by abdominal distention o Anorexia, vomiting, more severe pain ● Treatment o Treatment of underlying cause o Fluid and electrolyte replacement o Surgery and antimicrobial therapy
Gastritis ● Inflammatory disorder of the gastric mucosa ● Acute gastritis
GASTRIC AND DUODENAL ULCERS
- Most caused by H. pylori infection
- **Usually occur in the proximal duodenum (duodenal ulcers)
- Also found in the antrum of the stomach (gastric ulcers)** o Development begins with breakdown of mucosal barrier o Decreased mucosal defense more common in gastric ulcer development o Increased acid secretion predominant factor in duodenal ulcers
- Damage to mucosal barrier predisposes to development of ulcers and is associated with: o Inadequate blood supply ▪ Caused by vasoconstriction (e.g., by stress, smoking, shock, circulatory impairment in older adults, scar tissue, anemia) ▪ Interferes with rapid regeneration of epithelium o Excessive glucocorticoid secretion or medication o Ulcerogenic substances break down mucous layer. o Aspirin, NSAIDs, alcohol o Atrophy of gastric mucosa ▪ Chronic gastritis
- Increased acid pepsin secretions o Increased gastrin secretion o Increased vagal stimulation o Increased sensitivity to vagal stimuli o Increased number of acid pepsin secretory cells in the stomach (genetic anomaly) o Increased stimulation of acid pepsin secretion o Alcohol, caffeine, certain foods o Interference with normal feedback mechanisms o Rapid gastric emptying
- Complications of peptic ulcer o Hemorrhage ▪ Caused by erosion of blood vessels ▪ Common complication ▪ May be the first sign of a peptic ulcer o Perforation ▪ Ulcer erodes completely through the wall. ▪ Chyme can enter the peritoneal cavity. ▪ Results in chemical peritonitis o Obstruction ▪ May result later because of the formation of scar tissue
- Signs and symptoms