Download Patient Safety: Root Cause Analysis and more Slides Nursing in PDF only on Docsity!
Patient Safety: Root Cause Analysis
Lisa Ayoub-Rodriguez M.D. Credit to: Heidi Lyn M.D. Session time: 1:40pm – 2:25pm
Objectives
- Become familiar with the use of Root Cause Analysis in evaluating adverse outcomes in patient care
- Identify root cause/contributing factors in a given case.
- Categorize the root causes/identifying factors
- Suggest an action plan based on the factors identified.
Sentinel Event
- An unexpected occurrence involving death or serious psychological or physical injury, signaling the need for immediate investigation and response.
Process for Root Cause Analysis
- Step 1 – Investigate the Occurrence
- Step 2 – Identify Proximate Causes
- Step 3 – Identify the Root Cause
- Step 4 – Identify Previous Missed Opportunities
- Step 5 – Develop Corrective Actions
Identify Proximate Causes
- Qualify, validate, and verify all information collected in the investigation.
- Conduct a literature review of evidence- based practice and best practices. Include a search for Sentinel Event Alerts on the Joint Commission website.
Identify the Root Cause
- The process is the focus, not individual performance.
- The event or combination of events that initiate a failure.
- Consider WHY the individual committed the inappropriate act.
- Determine HOW the system influenced the individual’s thinking.
- Root Cause
- Event or events that initiate failure
- Contributory Cause
- Did not initiate the failure, but contributed to the outcome
Identify Previous Missed
Opportunities
- Determine whether previous similar occurrences have happened in the past
- Evaluate the effectiveness of corrective actions for these events
Develop Corrective Actions
- Include remedial and interim actions to reduce the risk of occurrence during the short term
- Assure robust corrective actions that address the Root Cause(s) and Latent Factors
Example
- A patient in a locked ward was found on the floor in his room with 3rd^ degree burns to his chest and arm. The patient had last been seen requesting a cigarette. A partially burned restraint was still attached to the patient’s wheelchair.
Brief Timeline
- Patient in locked ward
- Patient in wheelchair
- Restraint used to maintain position in wheelchair
- Patient requests cigarette and lighter
- Staff provide smoking materials - Short staffed - Patient left unattended - Patient uses lighter to ignite restraint - Restraint burns and patient slips out of chair - Patient found burned, laying on floor
Guidelines for Corrective Action Plans
- RCA Corrective Action Plans are based on investigation findings. Action items should address: - System weaknesses that are most directly associated with the event. - Steps in the process that are susceptible to failure or breakdown.
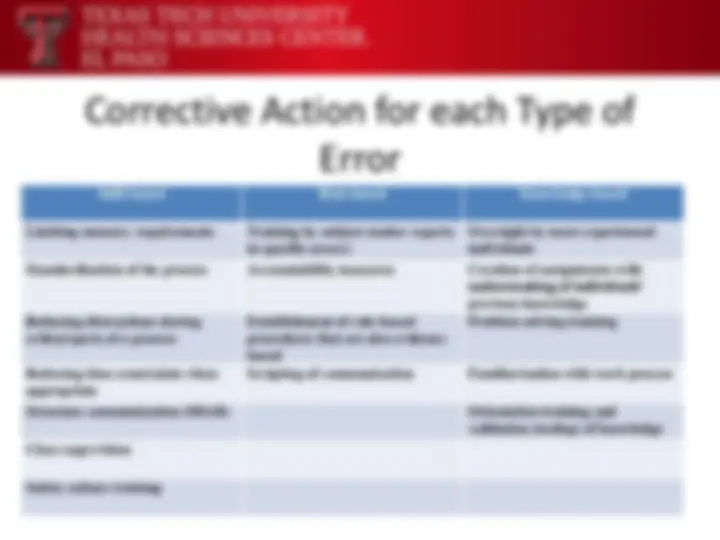
Hierarchy of Corrective Actions
Weaker Impact Intermediate Impact Stronger Impact Training / education Workload or staffing changes Engineering controls Change of a form (^) Reduction of interruptions and / or distractions Physical and / or structural changes to the environment Utilization of a label Checklists Standardization and hardwiring of a process Additional study Cognitive aids Cultural change New procedures Doublebacks -checks and / or read- Software changes Redundancy (^) Simplification of the process (reduce or change number of Communication structure^ steps)
Effectiveness of Error-Prevention Strategies
- Design process for minimum error: “ Mistake-Proof ” it.
- Control errors with active safety devices.
- Provide warning devices for manual actions.
- Use procedures for reduction of error and control.
- Use administrative controls for reduction of error.
- Rely on knowledge and skill of staff.
Most Effective
Least Effective
Type of SERIOUS SAFETY EVENT: List the Latent Weaknesses that contributed to the event (Inappropriate acts; system failures; equipment/deviceissues; etc.):
State the Root Cause(s):
List Corrective Action(s) for each Root Cause and Contributing Factor: # Corrective Actions Person(s) Responsible Due Date