@ShopWithKey on Etsy
1
Growth and Development
Description: Growth and development follow an orderly yet individual pattern. Nurses should assess growth and the emergence of developmental skills in all pediatric clients. Knowledge
of cognitive abilities allows a nurse to adapt teaching to the level of the child. Knowledge of appropriate toys and interests of children at different ages enables the nurse to use play to
facilitate the child's development and minimize problems caused by the hospitalization.
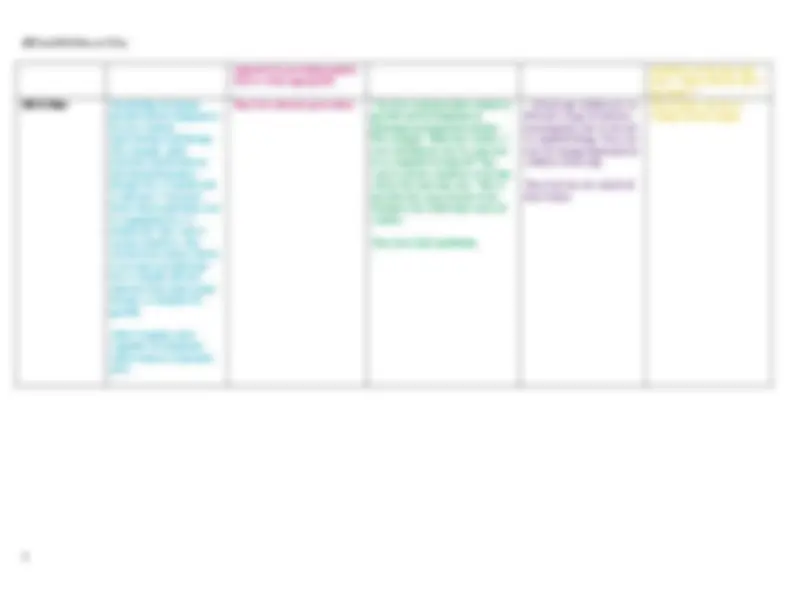
INFANT (BIRTH TO 1 YEAR)
TODDLER (1 TO 3 YEARS)
PRESCHOOL (3 - 6 Years)
SCHOOL-AGE (6 - 12 Years)
ADOLESCENT (12 - 19 YRS)
Erickson's Theory
trust vs mistrust
autonomy vs doubt & shame
initiative vs guilt
industry vs inferiority
identity vs role confusion
Developmental
milestones
1. Birth weight 2x by 6
months, 3xs by 12 months.
2. Birth length increases by
50% at 12 months.
3. Posterior fontanel closes
by 8 weeks.
4. Social smile at 2 months
5. Head turns to locate
sounds at 3 months.
6. Moro reflex disappears
4 months.
7. Steady head control at 4
months.
8. Rolls from abdomen to
back and back to abdomen
at 5 to 6 months.
9. Peek-a-boo 6 months.
10. Transfers objects from
hand to hand at 7 months.
11. Develops stranger
anxiety at 7 to 9 months.
12. Sits unsupported at 8
months.
13. Crawls at 10 months.
14. Fine pincer grasp
appears at 10 to 12 months.
15. Waves bye-bye at 10
months.
16. Walks with assistance
at 10 to 12 months.
17. Says a few words in
addition to “mama” or
“dada” at 12 months.
1. Birth weight quadruples by
30 months.
2. Achieves 50% of adult
height by 2 years.
3. Growth velocity slows.
4. Appears to be bowlegged
and potbellied.
5. All primary teeth (20)
6. Anterior fontanel closes by
12 to 18 months.
7. Throws a ball overhand at 18
months.
8. Kicks a ball at 24 months.
9. Feeds self with spoon and
cup at 2 years.
10. Daytime toilet training can
usually be started around 2
years.
11. Two- to three-word
sentences are spoken by 2
years.
12. Three- to four-word
sentences are spoken by 3
years.
13. Own first and last name can
be stated by 2½ to 3 years.
14. Temper tantrums are
common.
1. Each year, a child gains about 5
pounds and grows 2½ to 3 inches.
2. A child stands erect with more
slender posture.
3. A child learns to run, jump, skip,
and hop.
4. A 3-year-old can ride a tricycle.
5. Handedness is established.
6. A child uses scissors at 4 years.
7. A child ties shoelaces at 5 years.
8. A child learns colors, shapes.
9. Visual acuity approaches 20/20.
10. Thinking is egocentric and
concrete.
11. A child uses sentences of five
to eight words.
12. A child learns sexual identity
(curiosity and masturbation are
common).
13. Imaginary playmates and fears
are common.
14. Aggressiveness at 4 years is
replaced by more independence at
5 years.
1. Each year, a child gains 4
to 6 pounds and about 2
inches in height.
2. Girls may experience
menarche.
3. Loss of primary teeth and
eruption of most permanent
teeth occurs.
4. Fine and gross motor
skills mature.
5. A child is able to write
script at 8 years of age.
6. A child can dress self
completely.
7. Egocentric thinking is
replaced by social
awareness of others.
8. A child learns to tell time
and understands past,
present, and future.
9. A child learns cause-and-
effect relationships.
10. Socialization with peers
becomes important.
11. Molars (6-year) erupt.
1. Girls' growth spurts
during adolescence begin
earlier than boys' (may
begin as early as 10 for
girls).
2. Boys catch up at around
14 and continue to grow.
3. Girls finish growth at
around 15, boys 17
4. Secondary sex
characteristics develop.
5. Adult-like thinking
begins around 15. They can
problem-solve and use
abstract thinking.
6. Family conflicts develop.