Download PREVACID (lansoprazole) Indications, Dosage, and Adverse Events and more Lecture notes Pharmacokinetics in PDF only on Docsity!
PREVACID®, PREVACID®^ FasTab Product Monograph Page 1 of 80
PRODUCT MONOGRAPH
INCLUDING PATIENT MEDICATION INFORMATION
Pr PREVACID®
lansoprazole
Capsule (delayed-release), 15 mg and 30 mg, Nasogastric and Oral
Pr PREVACID® FasTab
lansoprazole Tablet (delayed-release), 15 mg and 30 mg, Nasogastric and Oral
Prescribed
Proton-Pump Inhibitors
PREVACID® is a trademark of Takeda Pharmaceuticals U.S.A., Inc. and used under license by BGP Pharma ULC.
Takeda Pharmaceuticals America, Inc. 95 Hayden Avenue Lexington, MA 02421, U.S.A.
Distributed by: BGP Pharma ULC 85 Advance Road Etobicoke, Ontario, M8Z 2S
Date of Preparation: MAY 12, 1995
Date of Previous Revision: MAR 4, 2021
Date of Revision: SEP 15, 2021
Submission Control Number: 251460
RECENT MAJOR LABEL CHANGES
TABLE OF CONTENTS
PREVACID®, PREVACID®^ FasTab Product Monograph Page 4 of 80
PART I: HEALTH PROFESSIONAL INFORMATION
1 INDICATIONS
PREVACID® (lansoprazole delayed-release capsules) and PREVACID® FasTab (lansoprazole delayed- release tablets) are indicated in the treatment of conditions where a reduction of gastric acid secretion is required, such as:
● Duodenal ulcer
● Gastric ulcer
● Reflux esophagitis including patients with Barrett's esophagus, and patients poorly responsive to an adequate course of therapy with histamine H 2 -receptor antagonists
● Healing of non-steroidal anti-inflammatory drug (NSAID)-associated gastric ulcer; treatment of NSAID-associated gastric ulcer in patients who continue NSAID use (controlled studies did not extend beyond 8 weeks)
● Reduction of risk of NSAID-associated gastric ulcers in patients with a history of gastric ulcers who require to continue taking a NSAID (a controlled study did not extend beyond 12 weeks)
● Symptomatic Gastroesophageal Reflux Disease (GERD); treatment of heartburn and other symptoms associated with GERD
● Pathological hypersecretory conditions including Zollinger-Ellison Syndrome (4. Recommended Dose and Dosage Adjustment)
● Eradication of Helicobacter pylori ( H. pylori )
Lansoprazole, in combination with clarithromycin plus amoxicillin as triple therapy, is indicated for the treatment of patients with H. pylori infection and active duodenal ulcer disease. Eradication of H. pylori has been shown to reduce the risk of duodenal ulcer recurrence (see 14 CLINICAL TRIALS and 4 DOSAGE AND ADMINISTRATION).
1.1 Pediatrics (1 to 17 years of age)
Based on the data submitted and reviewed by Health Canada, the safety and efficacy of PREVACID in pediatric patients has been established. Therefore, Health Canada has authorized an indication for pediatric use (see 7.1.3 Pediatrics).
PREVACID® is indicated for treatment of erosive and non-erosive GERD in children, aged 1 to 17 years. The clinical trial treatment period did not extend beyond 12 weeks.
1.2 Geriatrics
Geriatrics (>65 years of age): Evidence from clinical studies and experience suggests that use in the geriatric population is associated with differences in safety or effectiveness. The daily dose should not exceed 30 mg (see 7.1.4 Geriatrics).
PREVACID®, PREVACID®^ FasTab Product Monograph Page 5 of 80
2 CONTRAINDICATIONS
Lansoprazole is contraindicated in patients who are hypersensitive to this drug or to any ingredient in the formulation, including any non-medicinal ingredient, or component of the container. For a complete listing, see 6 DOSAGE FORMS, STRENGTHS, COMPOSITION AND PACKAGING.
Amoxicillin is contraindicated in patients with a known hypersensitivity to any penicillin (Please refer to the Amoxicillin Product Monograph before prescribing).
Clarithromycin is contraindicated in patients with known hypersensitivity to clarithromycin, erythromycin or other macrolide antibacterial agents. Clarithromycin is also contraindicated in patients receiving concurrent therapy with astemizole, terfenadine, cisapride or pimozide (Please refer to the Clarithromycin tablets Product Monograph before prescribing).
Co-administration with rilpivirine is contraindicated. See 9.4 Drug-Drug Interactions, Table 12.
3 SERIOUS WARNINGS AND PRECAUTIONS BOX
Serious Warnings and Precautions
If taking lansoprazole in combination with clarithromycin, note that clarithromycin should not be used in pregnancy except where no alternative therapy is appropriate, particularly during the first 3 months of pregnancy. If pregnancy occurs while taking the drug, the patient should be apprised of the potential hazard to the fetus. Clarithromycin has demonstrated adverse effects on pregnancy outcome and/or embryo- fetal development in monkeys, mice, rats and rabbits at doses that produced plasma levels 2 to 17 times the serum levels obtained in humans treated at the maximum recommended doses (see WARNINGS AND PRECAUTIONS section in the Clarithromycin Product Monograph).
4 DOSAGE AND ADMINISTRATION
4.1 Dosing Considerations
Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated.
Withdrawal of long-term PPI therapy can lead to aggravation of acid related symptoms and may result in rebound acid hypersecretion.
Duodenal Ulcer
Triple Therapy (PREVACID®/clarithromycin/amoxicillin): For the eradication of H. pylori to reduce the risk of duodenal ulcer recurrence, amoxicillin and clarithromycin should not be administered to patients with renal impairment since the appropriate dosage in this patient population has not yet been established.
Gastric Ulcer
PREVACID® (lansoprazole delayed-release capsules) and PREVACID® FasTab (lansoprazole delayed-release tablets) are not indicated for maintenance therapy in the treatment of patients with gastric ulcer.
PREVACID®, PREVACID®^ FasTab Product Monograph Page 7 of 80
† (^) Patients were included in the analysis if they had documented H. pylori infection at baseline as defined above and had a confirmed duodenal ulcer. ‡ (^) “Worst case” included patients with no available data as failures. Patients were included in the analysis if they had documented duodenal ulcer (active) and H. pylori infection at baseline defined as at least 2 of 3 positive endoscopic tests from CLOtest®, histology and/or culture.
Gastric Ulcer
The recommended adult oral dose is 15 mg once daily before breakfast for 4 to 8 weeks. No dosage adjustment is necessary in patients with renal impairment. No dosage adjustment is necessary in the initial PREVACID® or PREVACID® FasTab dosing regimen for older patients and for patients with mild to moderate hepatic impairment. Dosing recommendations described in the labelling should be adhered to for older patients and patients with hepatic impairment.
NSAID-Associated Gastric Ulcer
The issue of whether or not eradication of H. pylori in patients with NSAID-associated ulcers might have beneficial effects remains unresolved. Healing of NSAID-Associated Gastric Ulcer: The recommended adult oral dose is 15 to 30 mg once daily before breakfast for up to 8 weeks. A trend for higher healing rates (4% and 12%, two studies) was observed with the 30 mg dose, as compared to the 15 mg dose (see 14 CLINICAL TRIALS). Reduction of Risk of NSAID-Associated Gastric Ulcer: The recommended adult oral dose is 15 mg once daily before breakfast for up to 12 weeks (see 14 CLINICAL TRIALS).
Reflux Esophagitis or Poorly Responsive Reflux Esophagitis Including Patients with Barrett’s Esophagus
The recommended adult oral dose is 30 mg once daily before breakfast for 4 to 8 weeks (see 1 INDICATIONS).
Maintenance Treatment of Healed Reflux Esophagitis
For the long-term management of patients with healed reflux esophagitis, 15 mg lansoprazole given once daily before breakfast has been found to be effective in controlled clinical trials of 12 months (see 14 CLINICAL TRIALS). The recommended adult oral dose of PREVACID® or PREVACID® FasTab for maintenance treatment of patients with healed reflux esophagitis is 15 mg once daily before breakfast (see 1 INDICATIONS).
Treatment and Maintenance of Pathological Hypersecretory Conditions Including Zollinger-Ellison Syndrome
The dosage of PREVACID® or PREVACID® FasTab in patients with pathologic hypersecretory conditions varies with the individual patient. Doses should be adjusted to individual patient needs and should continue for as long as clinically indicated. The recommended adult oral starting dose is 60 mg once a day. Dosages up to 90 mg twice daily have been administered. Daily dosages of greater than 120 mg should be administered in divided doses.
PREVACID®, PREVACID®^ FasTab Product Monograph Page 8 of 80
Some patients with Zollinger-Ellison Syndrome have been treated continuously with lansoprazole for more than 4 years (see 14 CLINICAL TRIALS).
Gastroesophageal Reflux Disease (GERD)
Short-Term Treatment of Symptomatic GERD: The recommended adult oral dose for the treatment of heartburn and other symptoms associated with GERD is 15 mg once daily before breakfast for up to 8 weeks. If significant symptom relief is not obtained within 4 to 8 weeks, further investigation is recommended.
Pediatric GERD (erosive and non-erosive esophagitis)
In clinical studies, lansoprazole was not administered beyond 12 weeks in 1 to 11 year olds. It is not known if lansoprazole is safe and effective if used longer than the recommended duration. Do not exceed the recommended dose and duration of use in children as outlined below. Children (1 to 11 years): The recommended pediatric oral dose is 15 mg (≤30 kg) and 30 mg (>30 kg) once daily for up to 12 weeks. Children (12 to 17 years): The same approved regimen for adults can be used.
Patients with Hepatic Impairment
The daily dose of PREVACID® or PREVACID® FasTab should not exceed 30 mg (see 7 WARNINGS AND PRECAUTIONS).
Patients with Renal Impairment
No dosage modification of PREVACID® or PREVACID® FasTab is necessary (see 7 WARNINGS AND PRECAUTIONS).
Elderly Patients
The daily dose should not exceed 30 mg (see 7 WARNINGS AND PRECAUTIONS).
4.4 Administration
PREVACID® and PREVACID® FasTab should be taken daily before breakfast. Where the product may be used twice daily, it should be taken prior to breakfast and another meal. PREVACID® capsules and PREVACID® FasTab SHOULD NOT BE CRUSHED, CHEWED, BROKEN OR CUT.
For adults and children who have difficulty swallowing capsules, there are the following alternative administration options:
PREVACID® (lansoprazole delayed-release capsules) - Oral:
PREVACID® capsules can be opened, and the intact granules contained within can be sprinkled on 1 tablespoon of applesauce and swallowed immediately. The granules should not be chewed or crushed.
For patients who have a nasogastric tube (≥16 French) in place, PREVACID® capsules can be opened and the intact granules mixed into 40 mL of apple juice or water and then injected through the nasogastric tube into the stomach. After administering the granules, the nasogastric tube should be flushed with additional apple juice or water to clear the tube.
The granules have also been shown in vitro to remain intact for up to 30 minutes when exposed to apple, cranberry, grape, orange, pineapple, prune, tomato, and V-8® vegetable juice.
PREVACID®, PREVACID®^ FasTab Product Monograph Page 10 of 80
Oral doses up to 5000 mg/kg in rats (approximately 1300 times the recommended human dose based on body surface area) and mice (about 675.7 times the recommended human dose based on body surface area) did not produce deaths or any clinical signs.
For management of a suspected drug overdose, contact your regional poison control centre.
6 DOSAGE FORMS, STRENGTHS, COMPOSITION AND PACKAGING
Table 2. Dosage Forms, Strengths, Composition and Packaging
PREVACID® (lansoprazole delayed-release capsules)
PREVACID® (lansoprazole delayed-release capsules) is supplied in delayed-release capsules for oral administration. The delayed-release capsules contain the active ingredient, lansoprazole, in the form of enteric-coated granules and are available in two dosage strengths: 15 mg and 30 mg of lansoprazole per capsule.
PREVACID® 15 mg capsules are supplied as opaque, hard gelatin capsules with a pink cap printed with “PREVACID 15” and a bluish-green body printed with “TAP” logo. PREVACID® 15 mg capsules are available in bottles of 30 and 100.
PREVACID® 30 mg capsules are supplied as opaque, hard gelatin capsules with a pink cap printed with “PREVACID 30” and a black body printed with “TAP” logo. PREVACID® 30 mg capsules are available in bottles of 30 and 100.
Route of Administration
Dosage Form / Strength/Composition
Non-medicinal Ingredients
Oral, nasogastric Capsule (delayed-release) 15 mg, 30 mg
Colloidal silicon dioxide, D&C Red No. 28, FD&C Blue No. 1, FD&C Green No. 3 (15 mg capsules only), FD&C Red No. 40, gelatin, hydroxypropyl cellulose, low substituted hydroxypropyl cellulose, magnesium carbonate, methacrylic acid copolymer, polyethylene glycol, polysorbate 80, starch, sugar spheres, sucrose, talc, and titanium dioxide.
Oral, nasogastric Tablet (delayed-release) 15 mg, 30 mg
Aspartame*, citric acid, crospovidone, ferric oxide, glyceryl monostearate, hydroxypropyl cellulose, hydroxypropyl methylcellulose, lactose monohydrate, magnesium stearate, magnesium carbonate, mannitol, methacrylic acid, microcrystalline cellulose, polyacrylate, polyethylene glycol, polysorbate 80, strawberry flavor, talc, titanium dioxide, and triethyl citrate.
- Phenylketonurics: Contains Phenylalanine 2. mg per 15 mg Tablet and 5.1 mg per 30 mg Tablet.
PREVACID®, PREVACID®^ FasTab Product Monograph Page 11 of 80
PREVACID® FasTab (lansoprazole delayed-release tablets)
PREVACID® FasTab (lansoprazole delayed-release tablets) contain the active ingredient, lansoprazole in the form of enteric-coated microgranules. The tablets are available in 15 mg and 30 mg dosage strengths.
PREVACID® FasTab 15 mg tablets are supplied as white to yellowish white with orange to dark brown speckles, round, flat-faced, bevel-edged, uncoated, orally disintegrating tablets with “15” debossed on one side with a strawberry flavor. PREVACID® FasTab 15 mg tablets are available in blister packages of 30.
PREVACID® FasTab 30 mg tablets are supplied as white to yellowish white, with orange to dark brown speckles, round, flat-faced, bevel-edged, uncoated, orally disintegrating tablets with “30” debossed on one side with a strawberry flavor. PREVACID® FasTab 30 mg tablets are available in blister packages of 30 and 100.
7 WARNINGS AND PRECAUTIONS
Please see 3 SERIOUS WARNINGS AND PRECAUTIONS BOX.
General
Gastric Malignancy: Symptomatic response to therapy with PREVACID® (lansoprazole delayed-release capsules) or PREVACID® FasTab (lansoprazole delayed-release tablets) does not preclude the presence of gastric malignancy.
Pseudomembranous Colitis: Pseudomembranous colitis has been reported with nearly all antibacterial agents, including clarithromycin and amoxicillin, and may range in severity from mild to life threatening. Therefore, it is important to consider this diagnosis in patients who present with diarrhea subsequent to the administration of antibacterial agents. Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of clostridia. Studies indicate that a toxin produced by Clostridium difficile is a primary cause of "antibiotic-associated colitis".
After the diagnosis of pseudomembranous colitis has been established, therapeutic measures should be initiated. Mild cases of pseudomembranous colitis usually respond to discontinuation of the drug alone. In moderate to severe cases, consideration should be given to management with fluids and electrolytes, protein supplementation, and treatment with an antibacterial drug effective against Clostridium difficile colitis.
Clostridium Difficile-Associated Diarrhea: Decreased gastric acidity due to any means, including proton pump inhibitors (PPIs), increases gastric counts of bacteria normally present in the gastrointestinal tract. Treatment with proton pump inhibitors can lead to an increased risk of gastrointestinal infections such as Salmonella, Campylobacter and Clostridium difficile.
An increased risk for Clostridium difficile infection (CDI) and Clostridium difficile -associated diarrhea (CDAD) has been observed in association with PPI use in several observational studies. CDI/CDAD should be considered in the differential diagnosis for diarrhea that does not improve. Additional risk factors for CDI and CDAD include recent hospitalization, the use of antibiotics, old age and the presence of co-morbidities.
PREVACID®, PREVACID®^ FasTab Product Monograph Page 13 of 80
triglycerides, deep vein thrombosis and QT prolongation, are recommended. Dose reduction of saquinavir should be considered from the safety perspective for individual patients (see INVIRASE® Product Monograph).
Endocrine and Metabolism
Hypomagnesemia: Hypomagnesemia, symptomatic and asymptomatic, has been reported rarely in patients treated with PPIs for at least three months, in most cases after a year of therapy. Serious adverse events include tetany, arrhythmias, and seizures. Hypomagnesemia may lead to hypocalcemia and/or hypokalemia (see 8.5 Post-Market Adverse Reactions). In most patients, treatment of hypomagnesemia (and hypomagnesemia associated hypocalcemia and/or hypokalemia) required magnesium replacement and discontinuation of the PPI. For patients expected to be on prolonged treatment or who take PPIs with medications such as digoxin or drugs that may cause hypomagnesemia (e.g., diuretics), health care professionals may consider monitoring magnesium levels prior to initiation of PPI treatment and periodically (see 8 ADVERSE REACTIONS).
The chronic use of PPIs may lead to hypomagnesemia.
Cyanocobalamin (Vitamin B 12 ) Deficiency: The prolonged use of proton pump inhibitors may impair the absorption of protein-bound Vitamin B 12 and may contribute to the development of cyanocobalamin (Vitamin B 12 ) deficiency.
Gastrointestinal
When gastric ulcer is suspected, the possibility of malignancy should be excluded before therapy with PREVACID® capsules or PREVACID® FasTab tablets are instituted as treatment with these drugs may alleviate symptoms and delay diagnosis.
Long-term use of PREVACID® capsules or PREVACID® FasTab tablets is associated with an increased risk of fundic gland polyps, especially beyond one year (see 8.5 Post-Market Adverse Reactions). Most fundic gland polyps are asymptomatic. Use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated.
Genitourinary
In the 24-month toxicology study in rats, after 18 months of treatment, Leydig cell hyperplasia increased above the concurrent and historical control level at dosages of 15 mg/kg/day or higher.
Testicular interstitial cell adenoma also occurred in 1 of 30 rats treated with 50 mg/kg/day (13 times the recommended human dose based on body surface area) in a 1-year toxicity study.
These changes are associated with endocrine alterations which have not been, to date, observed in humans. For further details, see 16 NON-CLINICAL TOXICOLOGY.
Hepatic/Biliary/Pancreatic
Use in Patients with Hepatic Impairment: It is recommended that the initial dosing regimen need not be altered for patients with mild or moderate liver disease, but for patients with moderate impairment, doses higher than 30 mg per day should not be administered unless there are compelling clinical indications. Dose reduction in patients with severe hepatic disease should be considered.
Immune
Allergic reactions (including anaphylaxis) have been reported in patients receiving clarithromycin orally.
PREVACID®, PREVACID®^ FasTab Product Monograph Page 14 of 80
Serious and occasionally fatal hypersensitivity (anaphylactic) reactions have been reported in patients on penicillin therapy. These reactions are more apt to occur in individuals with a history of penicillin hypersensitivity and/or a history of sensitivity to multiple allergens.
There have been well documented reports of individuals with a history of penicillin hypersensitivity reactions who have experienced severe hypersensitivity reactions when treated with a cephalosporin. Before initiating therapy with any penicillin, careful inquiry should be made concerning previous hypersensitivity reactions to penicillins, cephalosporins, and other allergens. If an allergic reaction occurs, amoxicillin should be discontinued and the appropriate therapy instituted.
Serious anaphylactic reactions require immediate emergency treatment with epinephrine, oxygen, corticosteroids, and airway management, including intubation, as indicated.
Subacute cutaneous lupus erythematosus: Subacute cutaneous lupus erythematosus (SCLE) has been reported with the use of PPIs. If lesions occur, especially in sun-exposed areas of the skin, and if accompanied by arthralgia, the patient should seek medical help promptly and the health care professional should consider stopping PREVACID® or PREVACID® FasTab. The occurrence of SCLE with previous PPI treatment may increase the risk of SCLE with other PPIs (see 8.5 Post-Market Adverse Reactions).
Monitoring and Laboratory Tests
During treatment with antisecretory drugs, chromogranin A (CgA) increases due to decreased gastric acidity. Increased CgA levels may interfere with investigations for neuroendocrine tumours. To avoid this interference, PREVACID® or PREVACID® FasTab treatment should be stopped 14 days before CgA measurements (see 9.7 Drug-Laboratory Test Interactions).
Musculoskeletal
Bone Fracture : Several published observational studies suggest that PPI therapy may be associated with an increased risk for osteoporosis-related fractures of the hip, wrist, or spine. The risk of fracture was increased in patients who received high-dose, defined as multiple daily doses, and long-term PPI therapy (a year or longer). Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated. Patients at risk for osteoporosis-related fractures should be managed according to established treatment guidelines (see 4 DOSAGE AND ADMINISTRATION and 8 ADVERSE REACTIONS).
Ophthalmologic
Retinal atrophy: In animal studies, retinal atrophy was observed in rats dosed orally for 2 years with lansoprazole at doses of 15 mg/kg/day and above. These changes in rats are believed to be associated with the effects of taurine imbalance and phototoxicity in a susceptible animal model. Clinical data available from long-term PREVACID® capsules studies are not suggestive of any drug- induced eye toxicity in humans. In humans, there are presently no concerns for ocular safety with short-term lansoprazole treatment and the risks associated with long-term use for nearly 5 years appear to be negligible.
The finding of drug-induced retinal atrophy in the albino rat is considered to be species-specific with little relevance for humans. For further details, see 16 NON-CLINICAL TOXICOLOGY.
Renal
No dosage adjustment of PREVACID® or PREVACID® FasTab is necessary in patients with renal impairment. See 4.2 Recommended Dose and Dosage Adjustment and 10 CLINICAL PHARMACOLOGY.
PREVACID®, PREVACID®^ FasTab Product Monograph Page 16 of 80
population is supported by evidence of adequate and well controlled studies of lansoprazole in adults with additional clinical, pharmacokinetic, pharmacodynamic, and safety studies performed in pediatric patients. The adverse events (AEs) profile in pediatric patients is similar to that of adults. There were no adverse events reported in U.S. clinical studies that were not previously observed in adults. Dose safety and effectiveness have not been established in patients <1 year.
Developmental toxicity studies revealed that exposure to lansoprazole in juvenile rats starting at postnatal Days 7, 14, and 21 (approximately equivalent to neonatal, 1, and 2 year old human, respectively) resulted in development of heart valve thickening (see 16 NON-CLINICAL TOXICOLOGY, Juvenile Toxicity). However, the development of heart valve thickening has not been reported in pediatric clinical trials or in post-market reports.
7.1.4 Geriatrics
Benefits of use of PPIs should be weighed against the increased risk of fractures as patients in this category (>71 years of age) may already be at high risk for osteoporosis-related fractures. If the use of PPIs is required, they should be managed carefully according to established treatment guidelines (see 4 DOSAGE AND ADMINISTRATION and 8 ADVERSE REACTIONS).
Ulcer healing rates in elderly patients are similar to those in younger age groups. The incidence rates of adverse events and laboratory test abnormalities are also similar to those seen in other age groups. The initial dosing regimen need not be altered for elderly patients, but subsequent doses higher than 30 mg per day should not be administered unless additional gastric acid suppression is necessary.
8 ADVERSE REACTIONS
8.1 Adverse Reaction Overview
The most common adverse drug reactions (occurring in at least 1% of subjects) reported in adult patients treated with PREVACID in placebo and positive-controlled trials were headache, diarrhea, abdominal pain, nausea, and dizziness. The adverse reaction profile observed in adolescent patients ( to 17 years of age) was similar to that of adults.
8.2 Clinical Trial Adverse Reactions
Clinical trials are conducted under very specific conditions. The adverse reaction rates observed in the clinical trials; therefore, may not reflect the rates observed in practice and should not be compared to the rates in the clinical trials of another drug. Adverse reaction information from clinical trials may be useful in identifying and approximating rates of adverse drug reactions in real-world use.
Combination Therapy with Clarithromycin and Amoxicillin: In clinical trials using combination therapy with lansoprazole delayed-release capsules plus clarithromycin and amoxicillin, and lansoprazole delayed-release capsules plus amoxicillin, no adverse reactions related to these drug combinations were observed. Adverse reactions that have occurred have been limited to those that have been previously reported with lansoprazole delayed-release capsules, clarithromycin, or amoxicillin.
For more information on adverse reactions with clarithromycin or amoxicillin, refer to their respective Product Monographs, under the ADVERSE REACTIONS section.
Triple Therapy: PREVACID®/clarithromycin/amoxicillin: The most frequently reported adverse events for patients who received triple therapy were diarrhea (7%), headache (6%), and taste perversion (5%).
PREVACID®, PREVACID®^ FasTab Product Monograph Page 17 of 80
Patients in the 7-day triple therapy regimen reported fewer adverse events than those in the 10 and/or 14-day triple therapy regimens. There were no statistically significant differences in the frequency of reported adverse events between the 10 and 14-day triple therapy regimens.
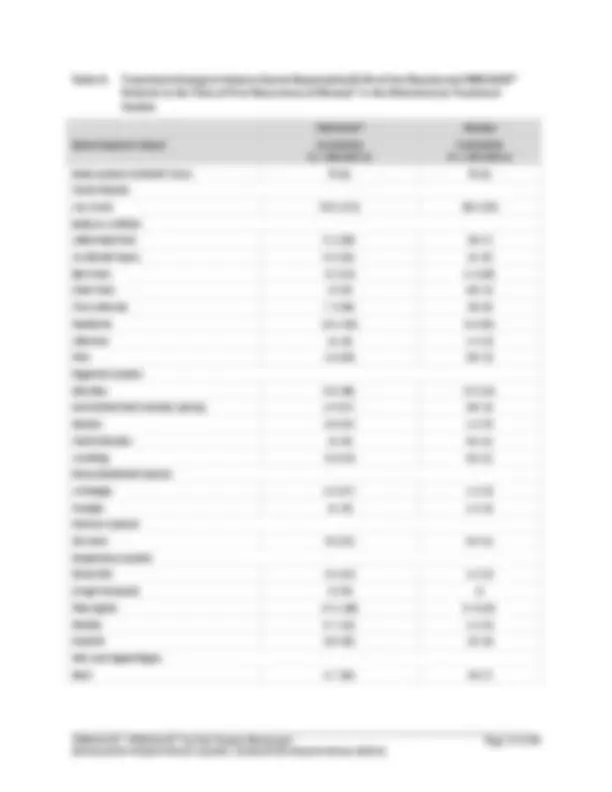
PREVACID® (lansoprazole delayed-release capsules): The following adverse events were reported to have a possible or probable relationship to drug as described by the treating physician in 1% or more of PREVACID®-treated patients who participated in short-term placebo- and positive-controlled trials (Table 3 and Table 4, respectively). Numbers in parentheses indicate the percentage of the adverse events reported.
Table 3. Incidence of Possibly or Probably Treatment-Related Adverse Events in Short-Term, Placebo-Controlled Studies in Takeda Safety Database*
Body System/Adverse Event†
PREVACID®‡ (N = 817) N (%)
Placebo (N = 254) N (%)
Body as a Whole
Headache 63 (7.7) 31 (12.2)
Abdominal Pain 19 (2.3) 3 (1.2)
Digestive System
Diarrhea 29 (3.5) 6 (2.4)
Nausea 9 (1.1) 5 (2.0)
Vomiting 7 (0.9) 3 (1.2)
Liver Function Tests Abnormal 2 (0.2) 3 (1.2)
Nervous System
Dizziness 8 (1.0) 2 (0.8)
- Takeda Pharmaceuticals America Inc. † (^) Events reported by at least 1% of patients on either treatment are included ‡ (^) Doses 15, 30 and 60 mg once daily for 4 to 8 weeks
In the Takeda Safety Database, all short-term, Phase II/III studies, one or more treatment-emergent adverse events were reported by 715/1359 (52.6%) PREVACID®-treated patients; of those considered to be possibly or probably treatment-related adverse events, one or more were reported by 276/ (20.3%) PREVACID®-treated patients. In all short-term, Phase II/III studies, one or more treatment- emergent adverse events were reported by 150/254 (59.1%) placebo-treated patients; of those considered to be possibly or probably treatment-related adverse events, one or more were reported by 56/254 (22.0%).
The most frequent adverse events reported in the European short-term studies were diarrhea (3.3%), laboratory test abnormal (2.3%), headache (1.5%), constipation (1.2%), asthenia (1.1%), dizziness (1.1%), and abdominal pain (1.0%). The most frequent adverse events reported in the Asian short-term studies were unspecified laboratory test abnormalities (7.3%), eosinophilia (1.0%), and increased SGPT (1.0%).
PREVACID®, PREVACID®^ FasTab Product Monograph Page 19 of 80
Table 6. Most Frequently Reported*^ Treatment-Emergent Adverse Events by Treatment Group and Dose in the Principal Reduction of Risk of NSAID-Associated Gastric Ulcer Studies†
Body System/ COSTART Term
PREVACID® 15 mg once daily (N = 136) % (n)
PREVACID® 30 mg once daily (N = 132) % (n)
Misoprostol 200 mcg four times daily (N = 134) % (n)
Placebo (N = 133) % (n)
Body as a Whole
Abdominal Pain 7% (9) 6% (8) 10% (14) 7% (9)
Digestive System
Diarrhea 10% (14) 13% (17) 25% (33)‡,§,¶^ 7% (9)
Nausea 1% (2) 5% (6) 6% (8) 5% (6)
Respiratory System
Pharyngitis 7% (10) 9% (12)‡^ 9% (12) 3% (4)
Sinusitis 5% (7) 6% (8) 2% (3) 2% (3)
Urogenital System
Urinary Tract Infection
4% (6) 1% (1) 7% (9) 2% (2)
- Reported by ≥5% of patients in any treatment group † (^) Treatment Duration: 12 weeks ‡ (^) Statistically significant difference versus placebo ( p ≤0. 0 5 ) § (^) Statistically significant difference versus PREVACID® 15 mg once daily ( p ≤0. 0 5 ) ¶ (^) Statistically significant difference versus PREVACID® 30 mg once daily ( p ≤0. 0 5 )
Gastroesophageal Reflux Disease (GERD) Studies
All adverse events reported from U.S. placebo-controlled studies that were considered to be possibly/probably treatment-related with an incidence of at least 5% in any treatment group are displayed by COSTART body system and term and by treatment group in Table 7.
Table 7. Adverse Events Possibly/Probably Related to Treatment, Reported by ≥ 5% of Patients in the U.S. Placebo-Controlled Non-Erosive GERD Studies
Body System/COSTART Term
PREVACID® N = 249 % (n)*
Placebo N = 71 % (n)
Total Patients
Any Event 28.5 (71)†^ 16.9 (12)
Body as a Whole
Headache 7.6 (19) 7.0 (5)
Abdominal Pain 6.0 (15) 1.4 (1)
Digestive System
Diarrhea 5.2 (13) 2.8 (2) † (^) Statistically significantly different versus placebo at p = 0.05 level
- Doses 15 and 30 mg once daily for 8 weeks
PREVACID®, PREVACID®^ FasTab Product Monograph Page 20 of 80
The most commonly reported (incidence ≥ 5% in any treatment group) treatment-emergent adverse events for PREVACID® patients were headache (14.9%), pharyngitis (9.6%), abdominal pain (8.8%), diarrhea (7.6%) and rhinitis (6.4%) and for placebo patients were headache (9.9%) and pharyngitis (9.9%). There were no clinically or statistically significant differences between PREVACID® and placebo when evaluated for treatment-emergent adverse events.
All adverse events reported from U.S. positive-controlled studies that were considered to be possibly/probably treatment-related with an incidence of at least 5% in either treatment are displayed by body system, COSTART term, and treatment in Table 8.
Table 8. Most Frequently Reported Possibly/Probably Treatment-Related Adverse Events by Treatment in the Positive-Controlled Non-Erosive GERD Studies*
Body System/COSTART Term
PREVACID®† 15 and 30 mg once daily (N = 572) % (n)
Ranitidine 150 mg twice daily (N = 283) % (n)
Total Patients
Any Event 16 (91) 17 (49)
Body as a Whole
Abdominal Pain 5 (29)‡^ 2 (5)
Digestive System
Diarrhea 4 (23) 6 (18)
- Reported by ≥ 5% of patients in any treatment † (^) Doses 15 and 30 mg once daily for 8 weeks ‡ (^) Statistically significantly different versus ranitidine at p = 0.05 level
The most frequently reported (≥ 5% of patients in any treatment) treatment-emergent adverse events for PREVACID®-treated patients were abdominal pain (9%), diarrhea (7%), and headache (6%) and for ranitidine-treated patients were diarrhea (9%), abdominal pain (7%), and headache (7%). There were no clinically or statistically significant differences between PREVACID®- and ranitidine-treated patients in the percentage of patients reporting specific treatment-emergent adverse events.
Treatment-emergent adverse events with an incidence of at least 2% in any treatment group of the maintenance treatment studies occurring from the start of maintenance treatment to the first recurrence of disease are displayed by body system and COSTART term, and by treatment group in Table 9.
There were no frequently reported (≥ 2.0%, incidence) severe adverse events in the treatment-emergent or the possibly/probably treatment-related event categories with onset at any point from the start of maintenance treatment to the time of first recurrence of disease.