Download Top 10 Appointment Systems with Shortest Patient Access Time for Doctors and more Lecture notes Dermatology in PDF only on Docsity!
SIMULATION-BASED APPOINTMENT
SCHEDULING: A CASE-STUDY
Word count: 25.
Melis Ongun
Student number: 01203839
Supervisor: Prof. dr. Broos Maenhout
Master’s Dissertation submitted to obtain the degree of Master of Science in Business
Engineering
Academic year: 2017 – 2018
I
FOREWORD
This dissertation forms the final piece of my five-year journey to obtaining the degree of Master of Science in Business Engineering. It is addressed to anyone interested in the field of operations research, especially applied to outpatient scheduling. Developing this dissertation would not have been possible without the help and support of several individuals. Therefore, I would like to express my gratitude to Prof. dr. Broos Maenhout for his guidance and advice. I would also like to thank the Ghent University Hospital dermatology department and in particular Elfie Deprez, without whom it would not have been possible to complete this case study. Further, my sincere appreciation goes to Carl Demessemaeker for his tremendous help with developing the simulation model. And finally, a special thanks goes to my family and friends for their support and encouragement, not only during the realization of this dissertation, but throughout my studies in general. Gent, June 2018 Melis Ongun
II
TABLE OF CONTENTS
FOREWORD ............................................................................................................................... I
TABLE OF CONTENTS ............................................................................................................. II
LIST OF USED ABBREVIATIONS ...........................................................................................VI
LIST OF TABLES ....................................................................................................................VII
REFERENCE LIST ...................................................................................................................IX
VII
LIST OF TABLES
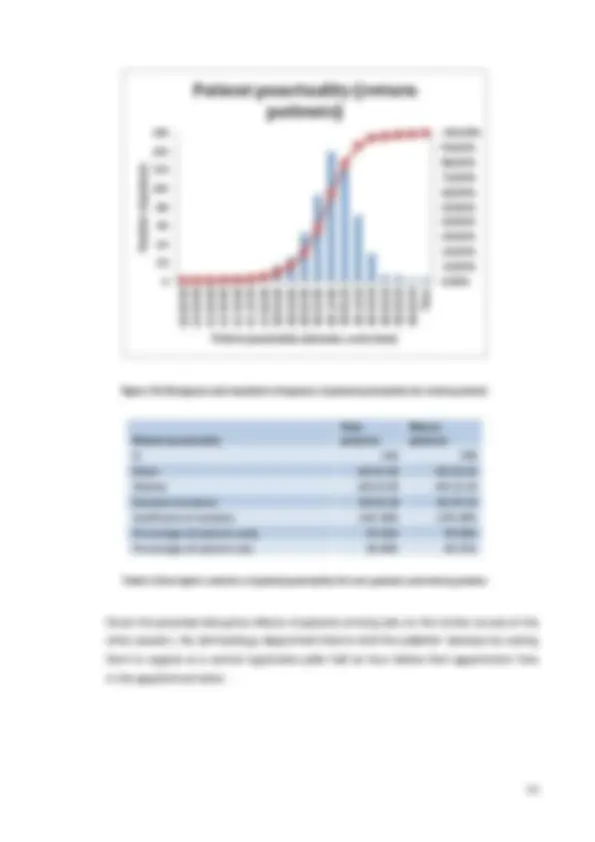
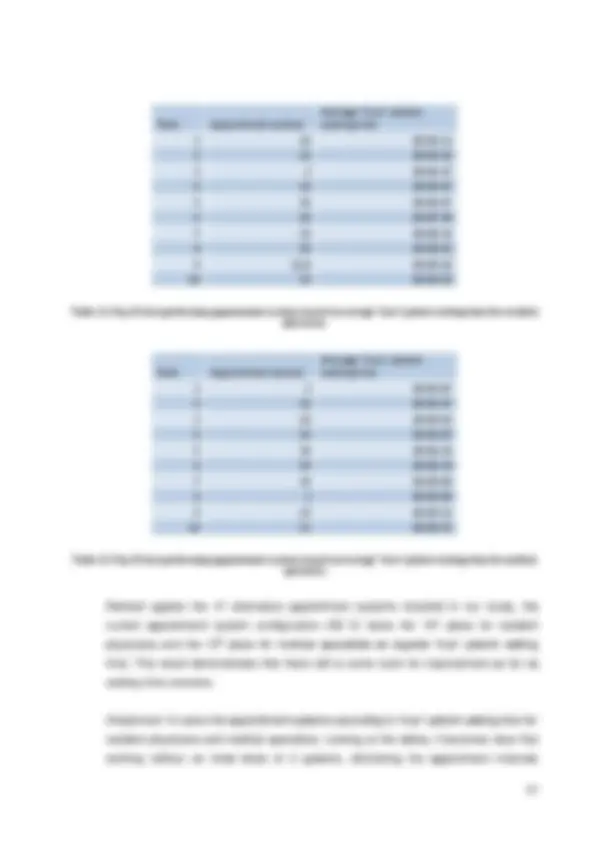
Table 1: Descriptive statistics of patient punctuality for all appointments, appointments with resident physicians and appointments with medical specialists ................................................ 50 Table 2: Descriptive statistics of patient punctuality for new patients and return patients.......... 53 Table 3: Month-to-month overview of the no-show percentages for 2014, 2015, 2016 and 2017 ................................................................................................................................................. 55 Table 4: Descriptive statistics of service time for resident physicians, medical specialists, new patients and return patients ...................................................................................................... 57 Table 5: Mean service time for all combinations of doctor and patient types ............................. 61 Table 6: Standard deviation of service time for all combinations of doctor and patient types .... 61 Table 7: Descriptive statistics of doctor lateness for all appointments, appointments with resident physicians and appointments with medical specialists ................................................ 62 Table 8: Descriptive statistics of “true” patient waiting time for all appointments, appointments with resident physicians and appointments with medical specialists ......................................... 68 Table 9: Mean and standard deviation of access time for appointment requests in April 2017.. 71 Table 10: Descriptive statistics of doctor overtime for all doctor types, resident physicians and medical specialists ................................................................................................................... 71 Table 11: Top 10 best performing appointment systems based on average “true” patient waiting time for resident physicians ...................................................................................................... 87 Table 12: Top 10 best performing appointment systems based on average “true” patient waiting time for medical specialists ....................................................................................................... 87 Table 13: Top 10 best performing appointment systems based on average patient access time for resident physicians .............................................................................................................. 88 Table 14: Top 10 best performing appointment systems based on average patient access time for medical specialists .............................................................................................................. 88 Table 15: Top 10 best performing appointment systems based on average doctor overtime for resident physicians ................................................................................................................... 90 Table 16: Top 10 best performing appointment systems based on average doctor overtime for medical specialists ................................................................................................................... 90 Table 17: Top 10 best performing appointment systems based on average doctor idle time for resident physicians ................................................................................................................... 92 Table 18: Top 10 best performing appointment systems based on average doctor idle time for medical specialists ................................................................................................................... 92 Table 19: Top 10 best performing appointment systems based on objective function value for resident physicians ................................................................................................................... 93
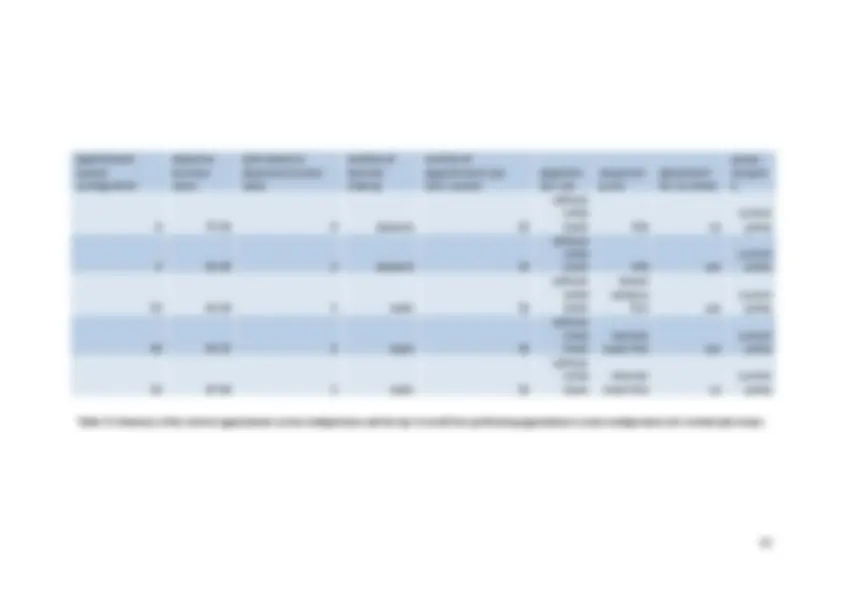
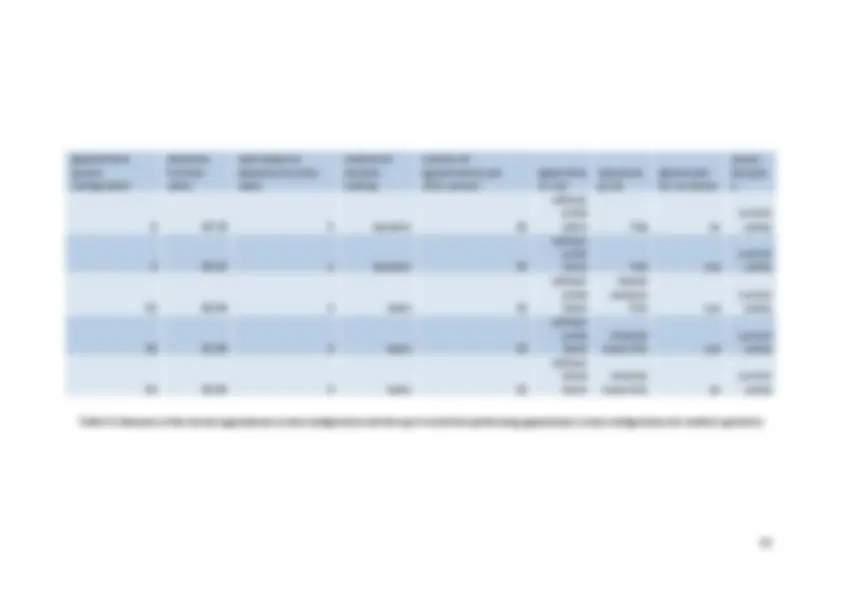
VIII Table 20: Top 10 best performing appointment systems based on objective function value for medical specialists ................................................................................................................... 93 Table 21: Summary of the current appointment system configuration and the top 3 overall best performing appointment system configurations for resident physicians .................................... 95 Table 22: Summary of the current appointment system configuration and the top 4 overall best performing appointment system configurations for medical specialists ..................................... 96 Table 23: Scenarios for sensitivity analysis .............................................................................. 97 Table 24: Average values for each performance measure and the resulting objective function value for AS 0 in the case of resident physicians ...................................................................... 99 Table 25: Average values for each performance measure and the resulting objective function value for AS 0 in the case of medical specialists ...................................................................... 99 Table 26: Average values for each performance measure and the resulting objective function value for AS 2 in the case of resident physicians .................................................................... 100 Table 27: Average values for each performance measure and the resulting objective function value for AS 2 in the case of medical specialists .................................................................... 100 Table 28: Average values for each performance measure and the resulting objective function value for AS 22 in the case of resident physicians .................................................................. 101 Table 29: Average values for each performance measure and the resulting objective function value for AS 22 in the case of medical specialists .................................................................. 101
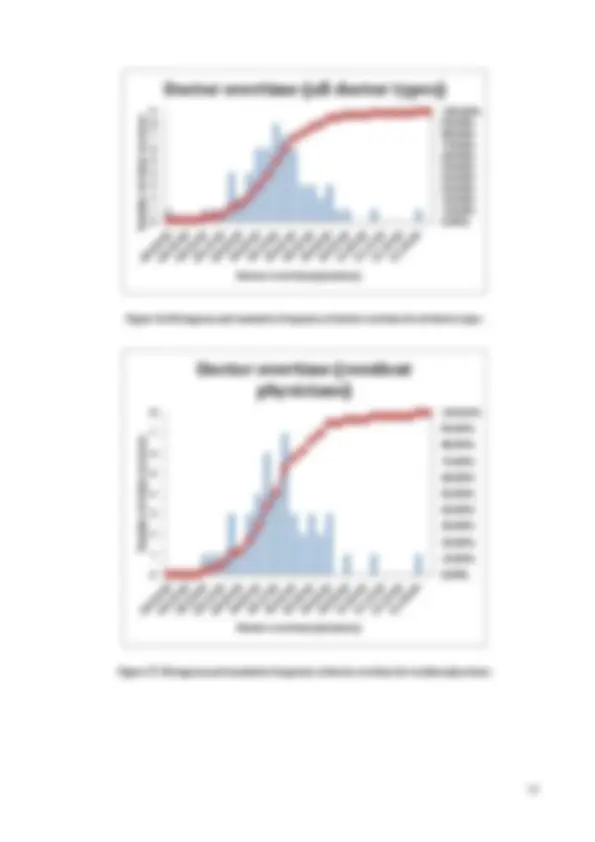
X Figure 33: Histogram and cumulative frequency of “true” patient waiting time for all appointments ............................................................................................................................ 69 Figure 34: Histogram and cumulative frequency of “true” patient waiting time for appointments with resident physicians............................................................................................................ 69 Figure 35: Histogram and cumulative frequency of “true” patient waiting time for appointments with medical specialists ............................................................................................................ 70 Figure 36: Histogram and cumulative frequency of doctor overtime for all doctor types ............ 72 Figure 37: Histogram and cumulative frequency of doctor overtime for resident physicians...... 72 Figure 38: Histogram and cumulative frequency of doctor overtime for medical specialists ...... 73 Figure 39: Experimental factors and their possible values/forms .............................................. 79
11
INTRODUCTION
In recent years, health care providers are being put under a great deal of pressure from two sides. On the one hand, being confronted with ever increasing health care costs and budget cuts, a lot of hospitals are struggling to survive financially^1. On the other hand, patients are becoming more and more assertive and expect high quality service.^2 As was already pointed out by Jackson in 1991, in addition to clinical competence, patients also expect reasonable waiting times. In fact, many studies have found that besides a high quality medical treatment, waiting time is one of the most significant predictors for patient satisfaction (Huang, 1994 ; Anderson, Camacho, & Balkrishnan, 2007 ). Health care institutions are thus at the same time prompted to reduce costs and improve quality of the services provided. In other words, hospitals are expected to do more with less. This means that the effective and efficient use of scarce resources (e.g. time and money) becomes increasingly important to survive in the health care industry. Taking into consideration the ageing of the population and as a result the growing demand for health care services, the optimal use of resources will continue to gain importance in the future. Another observation made during recent years, is the greater emphasis on preventive medicine practices and the shorter lengths of stay. Outpatient services are thus gradually becoming an essential component in health care. Hospitals that cannot make their outpatient departments more cost-effective find themselves in financially unviable positions in this fast-growing industry (Goldsmith, 1989). An outpatient clinic or ambulatory care clinic is the part of a hospital designed for the treatment of outpatients, people who arrive at the facility and leave the facility on the same day. In other words, it provides medical interventions such as diagnoses or treatments that do not require a bed or overnight stay. Nonetheless, outpatients are usually treated in the same departments as the patients that stay overnight. Outpatient clinics may be free-standing or part of a hospital. The latter is more common. They are usually organized around a single specialty or around a certain disease or symptom (Zonderland, 2014 , Chapter 1 ). Considering the two aforementioned observations made in the health care industry during recent years, the aspect of reducing costs while improving service in the specific context of outpatient clinics becomes an interesting area of research. A well-designed appointment system can help in reaching the two predefined goals. It has the potential to increase the utilization of expensive personnel and equipment-based medical resources, and in that way help to lower (^1) https://www.zorgneticuro.be/nieuws/besparingen-zetten-ziekenhuizen-onder-druk (^2) http://trends.knack.be/economie/beleid/het-is-tijd-voor-een-geintegreerde-aanpak-in-de-belgische- gezondheidszorg/article-opinion-877735.html
13 appointment scheduling are discussed in chapter five. Part two of the thesis contains the actual case study. A brief introduction to the case study is followed by four chapters. Chapter one gives the problem description. Chapter two covers the methodology for the case study. In chapter 3, the computational results are revealed. The next and final chapter, chapter four, concludes the case study and contains our recommendation for improvement of the appointment system.
14
PART 1: LITERATURE REVIEW
0. INTRODUCTION
The purpose of the literature review is to get a thorough understanding of the subject of outpatient scheduling and to identify all relevant information regarding the topic that will serve as the basis for the research. It will help to get familiar with the key terms, definitions and terminology related to the topic of outpatient scheduling. Cayirli & Veral (2003) present an extensive overview of the literature on outpatient scheduling. Their work will in fact serve as the base reference for the literature review. Since their review of literature was written more than a decade ago, it will be extended with some more recent articles that were published after the year 2003. The search for articles on appointment scheduling for outpatient services was mainly done using the databanks of Google Scholar, Science Direct and Web of Science, using keywords such as outpatient scheduling, appointment scheduling, appointment systems, outpatient planning and ambulatory health care. Subsequently, the results were refined to find articles on more specific topics (e.g. articles on appointment systems in the presence of walk-ins). The articles found were assessed on their relevance based on the content of their abstract. For the selected articles, we then further consulted their reference lists. Chapter one gives a problem definition for outpatient scheduling. Chapter two discusses the environmental factors used in literature to describe a clinical environment. A vital prerequisite to evaluate the current appointment system and to eventually come up with the ‘optimal’ design for the appointment system is to know which performance measure we want to optimize. Chapter three focuses on performance criteria used to evaluate appointment systems. Chapter four describes the decisions to be made when designing an appointment system and chapter five discusses the various analysis methodologies used in appointment scheduling literature.
16 affect the ultimate performance of the appointment system, it should be taken into account right from the start of the design of the system. From the above it is clear that outpatient scheduling, as was stated by Cayirli & Veral (2003), is an application of resource scheduling under uncertainty. The Project Management Institute (PMI) gives the following definition of resource scheduling: “Resource scheduling refers to the set of actions and methodology used by organizations to efficiently assign the resources they have to jobs, tasks or projects they need to complete, and schedule start and end dates for each task or project based on resource availability. Depending on industry, resources can be people (either employees or independent contractors), equipment and machines (this is frequent for construction, manufacturing or maintenance businesses) or rooms and facilities.” The problem of outpatient scheduling shows some clear similarities. In this case, the jobs/tasks to be done are the patients to be diagnosed/treated, the scheduled start date for each task corresponds with the assigned appointment time for a patient and the resources are the doctors, rooms and equipment. The uncertainty arises from a number of sources including uncertainty of the service time, the presence of no-shows or walk-ins and patient and doctor punctuality. With regard to the well-known hierarchical breakdown of strategic, tactical and operational decisions, the problem of outpatient scheduling is situated on the tactical level. Hulshof, Kortbeek, Boucherie, Hans, & Bakker (2012) give the following definition for strategic planning: “Strategic planning addresses structural decision-making. It involves defining the organization’s mission (i.e., ‘strategy’ or ‘direction’), and the decision-making to translate this mission into the design, dimensioning and development of the health care delivery process. Inherently, strategic planning has a long planning horizon and is based on highly aggregated information and forecasts.” Capacity dimensioning is part of strategic decision-making. For ambulatory care facilities, it involves dimensioning resources such as staff, equipment, space and time. Since capacity is considered given, strategic planning won’t be part of this research. “Tactical planning on the other hand translates strategic planning decisions to guidelines that facilitate operational planning decisions. While strategic planning addresses structural decision
17 making, tactical planning addresses the organization of the operations/execution of the health care delivery process (i.e., the ‘what, where, how, when and who’).” (Hulshof et al., 2012) Tactical planning is the level on which appointment scheduling takes place, and hence this is the level on which our research will focus. Finally, the lowest level of decision-making is the operational level. Hulshof et al. (2012) define operational planning as follows: “Operational planning involves the short-term decision making related to the execution of the health care delivery process. Following the tactical blueprints, execution plans are designed at the individual patient level and the individual resource level.”