Download Study for some slides and notes and more Slides Nursing in PDF only on Docsity!
HEMATOLOGY AND
INFECTIOUS DISEASE
AGENDA
Anemias
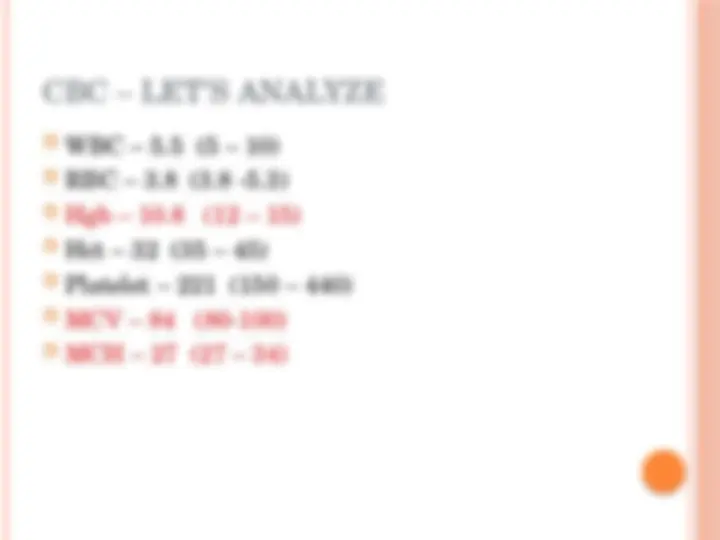
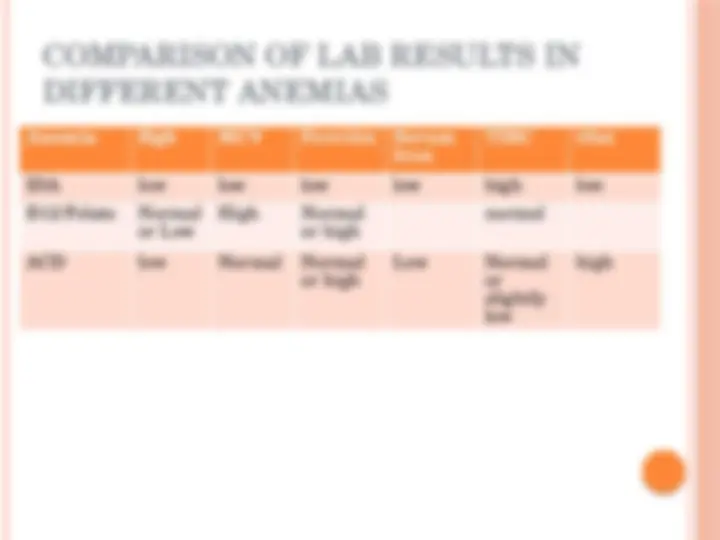
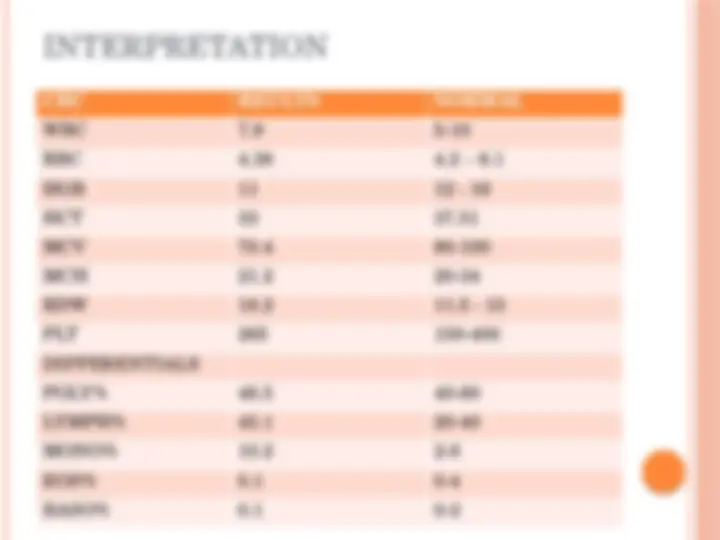
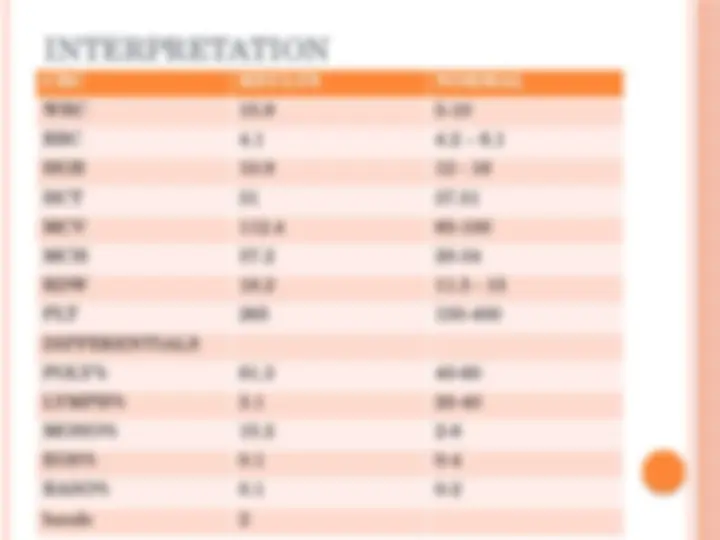
Interpreting RBC, Hgb and RBC indices
Microcytic Anemia
Macrocytic Anemia
Normocytic
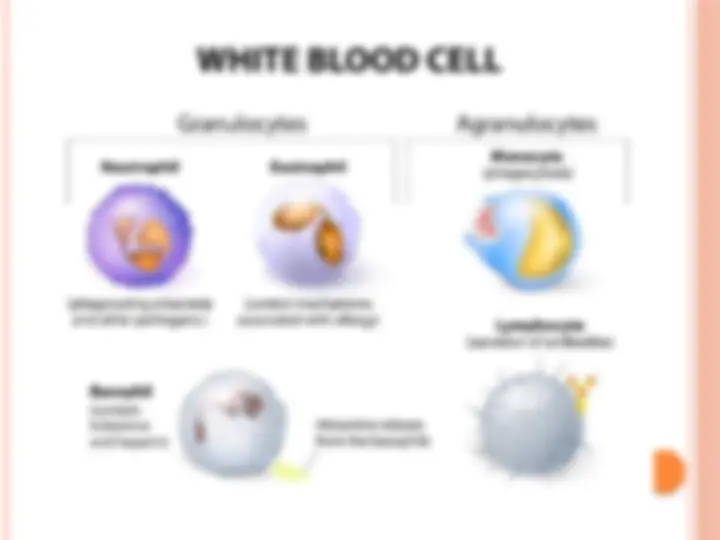
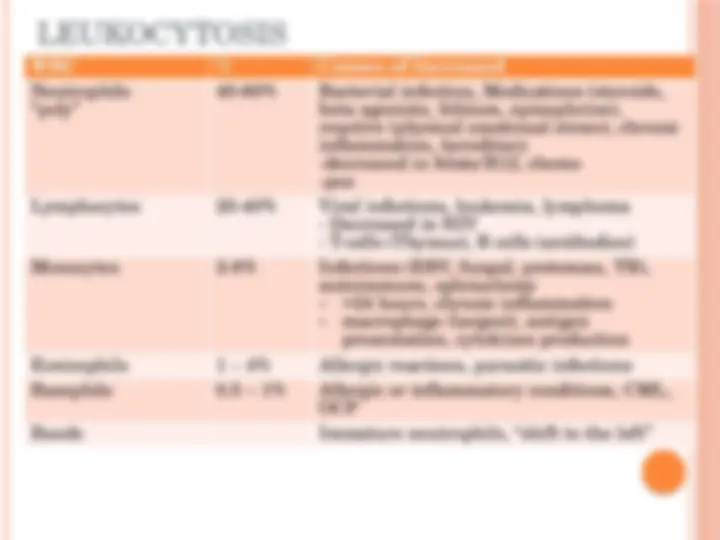
WBC interpretation
Infectious Mono
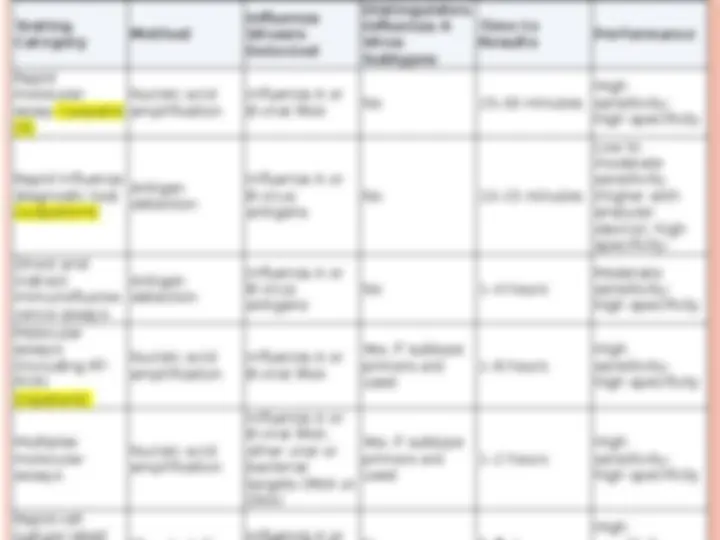
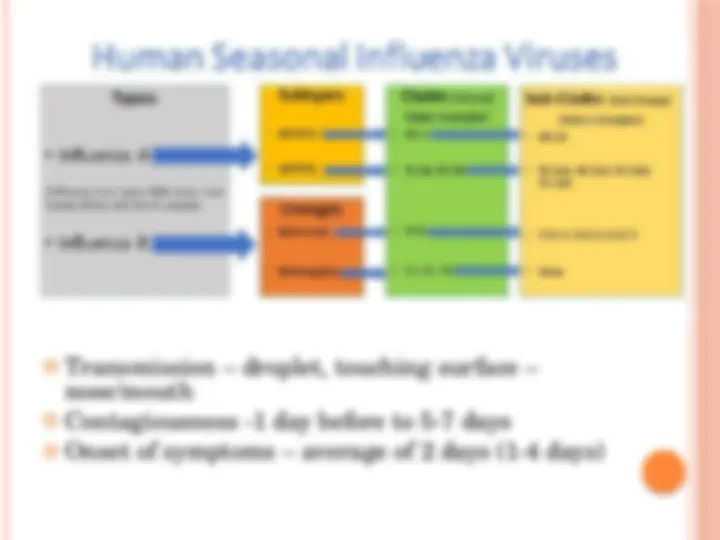
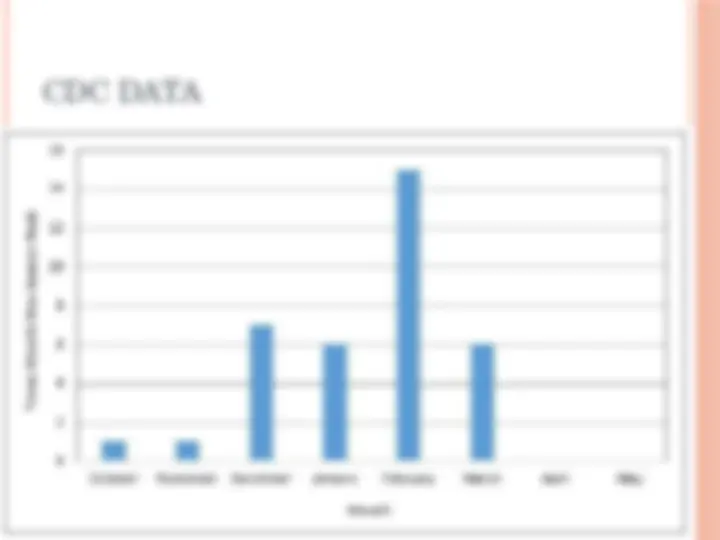
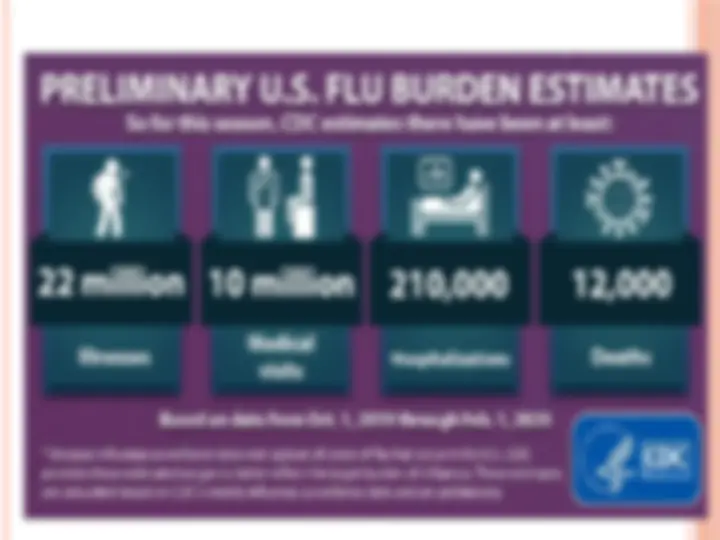
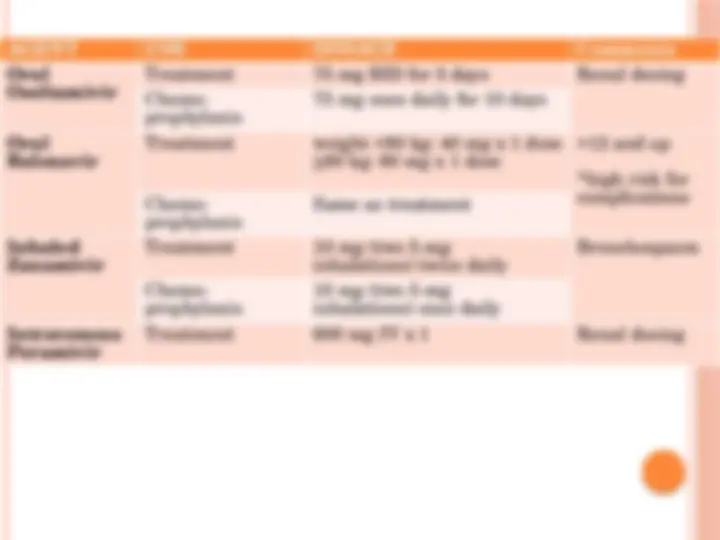
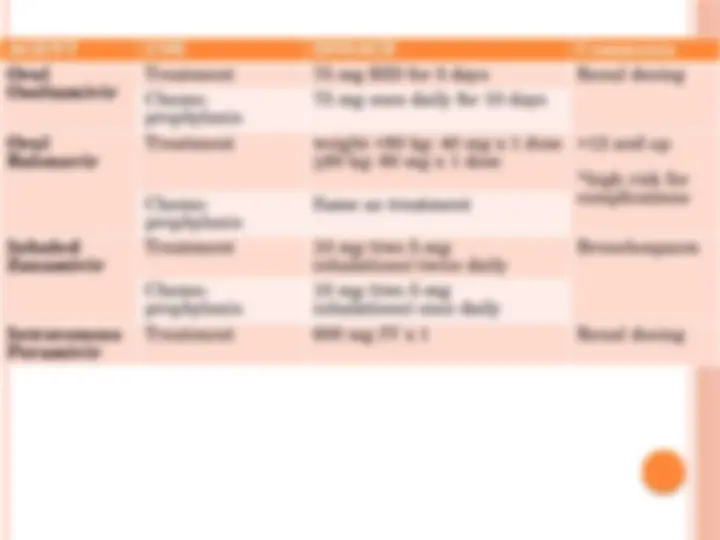
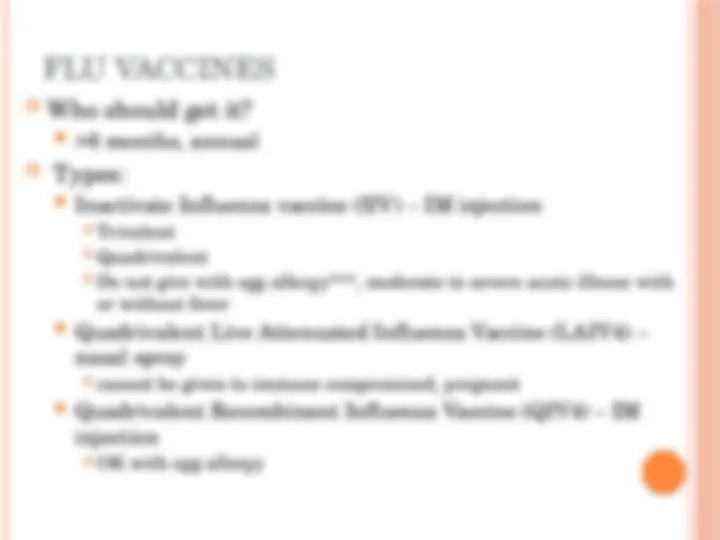
Influenza
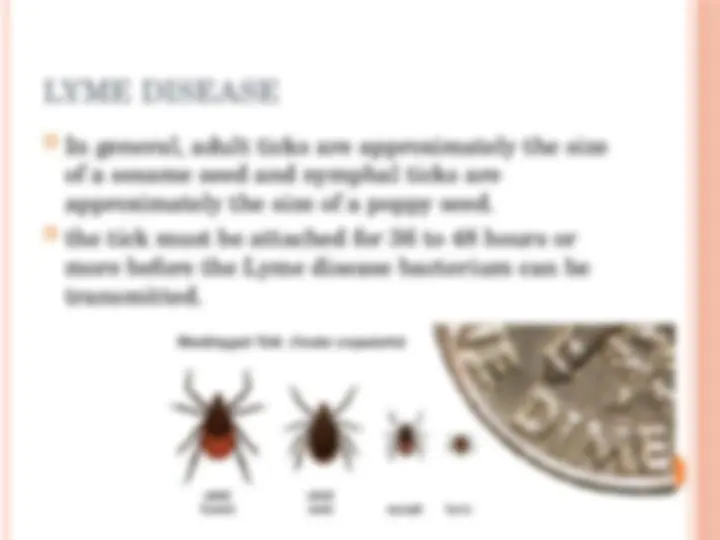
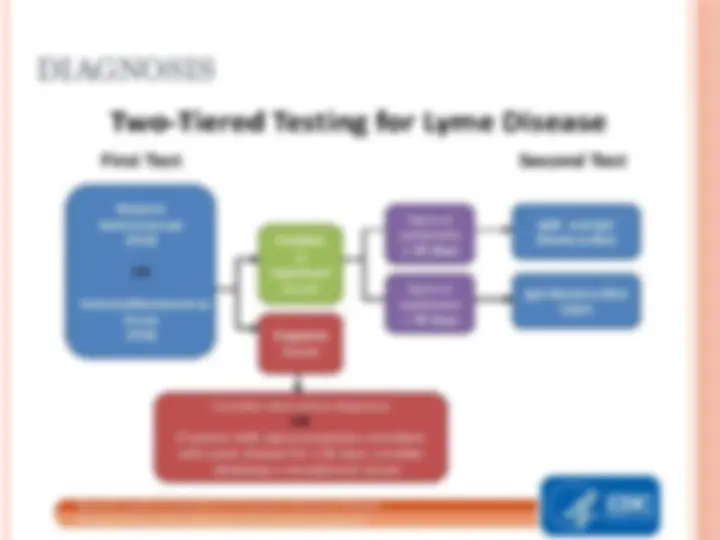
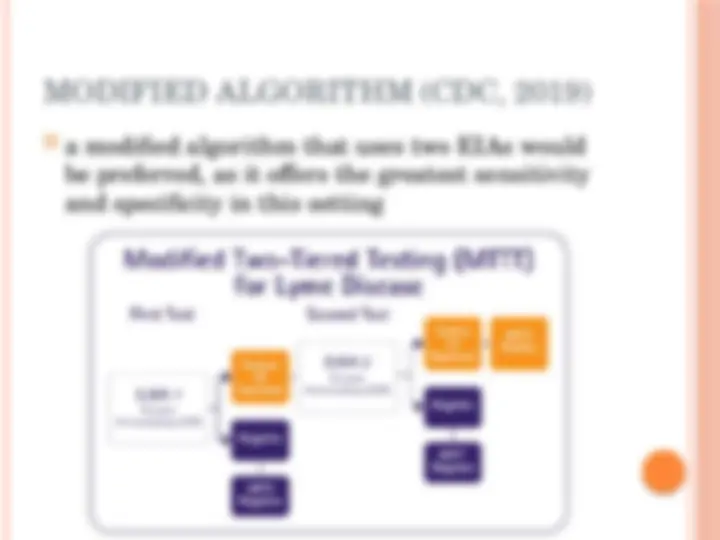
Lyme Disease
ANEMIA
Not a disease but a sign/symptom of an
underlying disorder
Defined by low Hgb (<12 g/dl in women, <14 g/dl
in men
decreased RBC production, increased RBC
destruction, and blood loss
Important to identify underlying condition or
cause
MCH – MEAN CORPUSCULAR
HEMOGLOBIN
Amount of Hgb in RBC
27 – 34 pg
Hypochromic anemia
Hyperchromic anemia
MCV - MEAN CORPUSCULAR
VOLUME
Size of average RBC
Categorizing anemia
Microcytic < 80 (80-100 fl)
Fe deficiency
Thalassemia
Anemia of Chronic Disease (ACD) - occasionally
Normocytic < 80 – 100
Acute blood loss
ACD – including renal failure
Macrocytic >
Megaloblastic anemia – B12 or folate deficiency
CASE STUDY 1
M.B. is a 42 year old Caucasian female who
presents to the office for an annual physical. She
offers no specific complaints other than lack of
energy and feeling fatigued at the end of the day
for the past 3 – 4 months. She attributes it to
being a busy mom and working full-time but
admits to feeling worse in the past few months.
Meds – none
Allergies - none
PMH – C-section 2014
FH – father HTN, mother A&W
PE
(^) Ht – 5’6” Wt – 140 lbs. (^) BP =126/68 HR =88 RR = 16 Temp =98. (^) General – well-groomed, skin smooth, dry intact (^) HEENT – normocephalic, PERRLA, conjunctiva slightly pale, oral membranes moist, neck supple, thyroid non palpable (^) Lungs – eupneic, CTA bil (^) CV – S1S2 RRR, no edema (^) Abd – soft, non-distended, non –tender, + BS (^) MS – full ROM 5/5 strength, no swelling or deformities Neuro – AAO x 3
CLINICAL PRESENTATION
May not have any symptoms until anemia is
severe (Hgb < 6 g/dl)
Iron Deficiency anemia (IDA) – can cause
symptoms with Hgb <11 g/dl
Most common presentation – fatigue, mild
dyspnea and mild exercise intolerance
Moderate to severe anemia – marked dyspnea,
activity intolerance, pallor, tachycardia
Elderly patients may present with exacerbation of
comorbidities – dementia, chest pain, HF
IRON DEFICIENCY ANEMIA (IDA)
Most common cause of anemia
Most common nutritional deficiency
Most common cause is chronic blood loss
Menorrhagia, GI bleed – NSAID/ASA
In women, include menstrual hx – menorrhagia or
pregnancy?
Also caused by:
inadequate diet
Malabsorption – celiac, H. pylori, gastric bypass
increase iron requirements – pregnancy
Extreme athletes
QUESTION
In a patient with Iron-Deficiency Anemia, which
blood work would indicate the earliest
abnormality to confirm the diagnosis?
A. Transferrin
B. Total Iron binding capacity
C. Serum Iron
D. Ferritin
FERRITIN
Iron stores
Earliest lab abnormality
Most accurate test to diagnose IDA
Women – 12- 150 ng
Men - 15 – 300 ng
Decreased – IDA
Increased - ACD, sideroblastic anemia
In chronic states of inflammation - <50ng is
considered IDA
OTHER TESTS
Usually not necessary:
Reticulocyte count – new immature RBCs (1%)
decreased
Peripheral smear – provides information of count and
morphology
Bone marrow – rare
Other tests:
o Stool OB – r/o GI beed
o HCG test
DIFF DX - THALASSEMIA
Labs:
RDW – normal
Retic count – increased
Ferritin – normal
high-performance liquid chromatography (HPLC)/
Hgb electropheresis – diagnostic standard
Globin gen – diagnostic confirmation
Pre-conception and pre-natal testing and counselling
ACD
Non- anemia diff dx
Hypothyroid
Pregnancy
Uterine fibroid