Partial preview of the text
Download Summary WGU D345 Comprehensive Study Guide: Dr Cole Remediation for OA | Latest Update wit and more Exams Nursing in PDF only on Docsity!
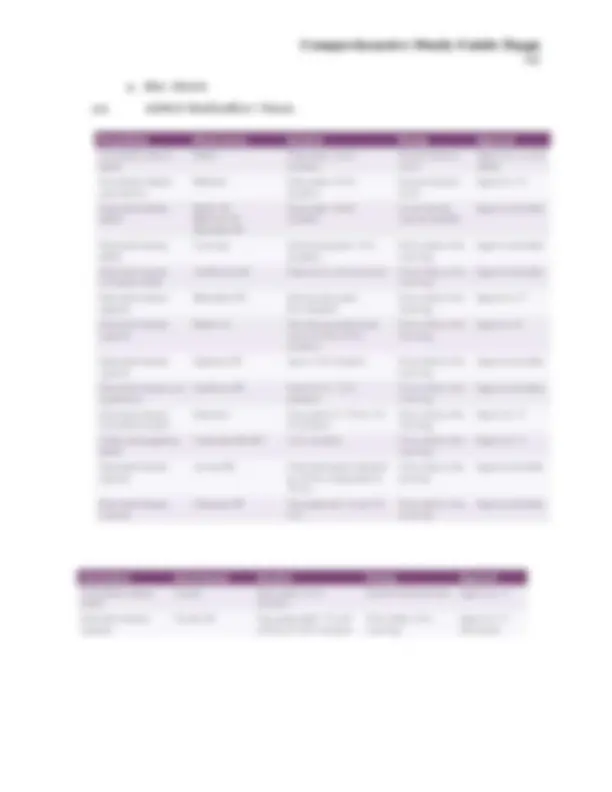
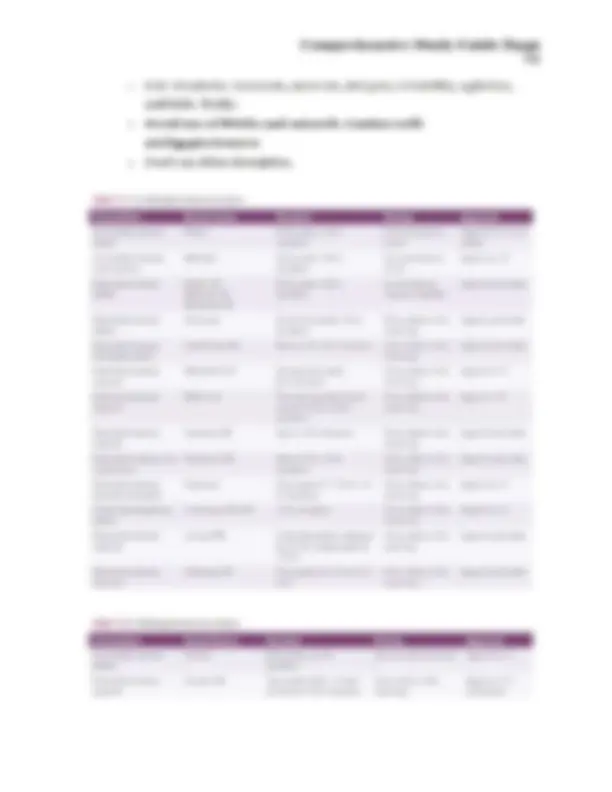
Comprchensive Study Guide D345 1 Section 1 Highlight Guide 1. Neurotransmitters: know all the neurotransmitters, the role of various neurotransmitters in various diagnosis and symptoms. Recommendation: Make a chart with various diagnosis and the role various neurotransmitters play in that diagnosis/symptom. The study of the magnitude and variation of drug response is the definition of pharmacodynamics. Psychodynamics is the study of what the body does to a drug and helps explain the relationship between the dose and response. Dopamine produced in substantia nigra and ventral tegmental area « D: Drive/Drugs = O: psychOsis » P: Prolactin Inhibition » A: Attention = M: Motivation « I: Involuntary Movements =» N: Nausea = E: Energy Serotonin is produced mostly in Raphe nucleus «= DOMAINS: Depression, Obsession, Migraines, Anxicty, Intestines, Nausea, and Sexual. « Serotonin Syndrome: Shils and SHIVERS. Shils(diarrhea), Shivering, Hyperreflexia, Increased temperature, Vital sign instability, Encephalopathy, Restlessness, and Sweating. Norepinephrine is produced in locus ceruleus of the pons » Receptors A1, A2, Bi, B2, and B3. More blood vessels. « Fight or flight. Sympathetic nervous system. « Concentraling, focusing, burst of energy, increased BP/HR, mobilizing glucose Epinephrine produced by the adrenal glands = More heart « Fight or flight. Sympathetic nervous system. Acetylcholine synthesized by the Basal Nucleus of Meynart Comprchensive Study Guide D345 ey » Parasympathetic Nervous system. Rest and Digest. Feed and breed. oc Muscarinic Receptors Comprchensive Study Guide D345 4 first messenger "| ‘The first messenger causes the receptor to change G protein can now bind to the receptor Figure 1-13 First messenger. In this figure, the neurotransmitter has docked into its receptor. The Se cain eceeng ieteteraioe st G protein the receptor to that the receptor can bind to the G protein, indicated here by the receptor tuming the same color as the hneurotransmiter and changing @ shape at the bottom in order to make @ capable of binding to the G protein and eahouinueet eieal messengers, Having many as Alte hannel-linked G-protein-linked neurotransmitter Neurotansmitter — hormone First Messenger - 4 = Second Messenger Third Messenger Fourth Messenger/ cell nucleus Comprchensive Study Guide D345 5 Activating a Third-Messenger Kinase through Cyclic AMP first messenger neurotransmitter ko second out activation inactive third messenger protein kinase active protein kinase 4. Pharmacokinetics and Pharmacodynamics are factors that affect both. c Pharmacokinetics- What the BODY does to the drug or how it is processed by the body. co Pharmacodynamics- What the Drug does to the body and how it produces the therapeutic effect. The MOA. c Pharmacokinelics processes vary belween palienls because they are affected by body factors such as gender, age, weight, genctics, and also drug-drug interactions. The process is affected by a pregnancy and a patient's pathophysiology. c Pharmacodynamics is another process involving the relationship belween drug concentration al the sile of aclion and ils effects. Medicalion binding determines drug impact al the site of movement with a receptor. Understanding cach medication's full range of receptor interactions is critical 5. Agonisl, anlagonisl, partial agonist, inverse agonist, depolarizalion, repolarizalion c Agonisl- Substance which iniliales a physiological response when combined with a receptor. «© Antagonist- Substance that interferes/inhibits the physiological action of another. © Partial Agonist- Binds to a receptor and activates it, but to a Comprchensive Study Guide D345 Zz oc Inverse agonist- Substance that binds to a receptor and produces an effect opposite of the agonist. ce Depolarizalion- Rapid increase in membrane polential(becomes less negalive) and posilively charged ions rush into the cell. Excites and causes an action. «© Repolarization- Return to resting membrane potential(becoming more negative) as positive ions leave the cell. Rest phase. Comprchensive Study Guide D345 8 Neurotransmitter G-protein Pharmacological Therapeutic receptor and action action pharmacological subtype directly targeted Dopamine D, Antagonist or Antipsychotic; antimanic partial agonist Serotonin SHT 2, Antagonist or Antipsychotic actions in Parkinson's disease inverse agonist —_ psychosis Antipsychotic actions in dementia-related psychosis Reduced drug-induced parkinsonism Possible reduction of negative symptoms in schizophrenia Possible mood stabilizing and antidepressant actions in bipolar disorder Improve insomnia and anxiety Agonist Psychotomimetic actions Experimental treatment of refractory depression and other disorders, especially accompanying psychotherapy SHTiano Antagonist or Possible pro-cognitive and antidepressant actions partial agonist SHT oc Antagonist Antidepressant SHT, ? ? SHT, Antagonist Possible pro-cognitive and antidepressant actions SH... Partial agonist Reduced drug-induced parkinsonism Anxiolytic Booster of antidepressant actions of SSRis/SNRIs Norepinephrine Alpha 2 Antagonist Antidepressant actions Agonist Improved cognition and behavioral disturbance in ADHD Alpha 1 Antagonist Improved sleep (nightmares) Improved agitation in Alzheimer disease Side effects of orthostatic hypotension and possibly sedation GABA GABAB Agonist Cataplexy Sleepiness in narcolepsy Possible enhanced slow-wave sleep Pain reduction in chronic pain and fibromyalgia Possible utility for alcohal use disorder and alcohol withdrawal Melatonin MT, Agonist Improvement of insomnia and circadian rhythms MT, Agonist Improvement of insomnia and circadian rhythms Comprchensive Study Guide D345 10 Agonist Spectrum no agonist or silent antagonist inverse Ses agonist agonist 1. Anxiolytics, Sleep Medications-page 366 in the review and resource manual, see supplemental learning materials in course Lips. 2. Benzodiazepines: indicalions, short lerm use, risk of tolerance and dependence, contraindications (ex: PTSD or delirium). 3. Hypnotics/sleep medications: short acting, intermediate acting and long-acting medications. Page 365-366 in review and resource manual. Benzodiazepines and Nonbenzodiazepines. Flurazepam, Temazepam, Triazolam, Sonata, Lunesta, Ambien, Rozerem, Belsomra, Elavil, doxepin, Remeron, Trazodone a. Z-Drugs: Zaleplon, zolpidem, zopiclone. Allosteric Modulators of GABA-A. i. Zolpidem CR(controlled release) extends the duration of action form 2-4 to 6-8 hours. Can be sublingual for faster onset with a fraction of the usual nighttime dose. ii. Binda to GABA-A receptors and some bind selectively to A1(zaleplone&zolpidem). b. Benzo(also zopiclone/eszopiclone) bind to A1, A2, A3, and A5. A1 is crilical for producing sedalion. Comprchensive Study Guide D345 oe i. A1 receptor is also links lo daylime sedation, anticonvulsant actions, and possibly to amnesia. ii. iii. iv. Comprchensive Study Guide D345 13 1. Off label Bipolar. Dizzy, somnolence, headache, alaxia, N, S. Serious Stevens Johnson. Angioedema. Monitor serum sodium(especially first 3 months). NA channel blocker. POTENT INDUCE CYP3A4. Comprchensive Study Guide D345 14 v. Asian descent screen for HLA-B. Increased risk of steven johnson syndrome. vi. Can be used as mood stabilizer. Trileptal reduces effectiveness of birth control. 4. Benzodiazepines: Flurazepam (long lasting agent), Temazepam (intermediate acting agent), Triazolam (short acling agent) 5. P450 syslem-inducers, inhibitors. See supplemental learning materials under course tips. a. Pharmacokinctic actions via hepatic and gastrointestinal drug- metabolizing systems. P450(CYP450 2D6 enzyme to help break down). Comprchensive Study Guide D345 16 e f. GABA-a is subtypes a1-a6. B is b1 to bg. And y1-y3. Ther are also 6, e, 1, 8, and p (with three isoforms p1 to p93). Comprchensive Study Guide D345 17 g- Y subunit tend to be synaptic to mediate phasic neurotransmission and be sensitive to Benzodiazepines. h. GABA-a with 6 subunit are extrasynaptic and mediate tonic(low level release of neurotransmitters) neurotransmission. Tnserste ts haeces ‘Two Types of GABA, Mediated Inhibition GABA GABA, — (e405 Me - (S) eB ae hast © 3 d Comprchensive Study Guide D345 19 nicoline thal is delivered and presumably desensilizes an important number of resensitizing and craving nicotinic receptors. ii. iii. Comprehensive Study Guide D345 20 Varenicline(Chantix): A selective A4B2 nicotinic acetylcholine receptor partial agonists. Stabilizes the channel in the closed state but does not desensitize the receptors. Less used is reducing cravings by boosting dopamine with the norepinephrine-dopamine reuplake inhibilor(NDRI) bupropion(Wellbutrin). 1. Releases a bit of dopamine in the nucleus accumbens making the craving less. b. Opioid: i. ii. iii. iv. vi. Both clonidine and lofexidine are a2-adrenergic agonists that reduce signs of autonomic hyperactivity during withdrawal and aid in the detoxification process. Naltrexone: Shortens the withdrawal lime of an A2 agonist administered with methadone or buprenorphine. 1. Monthly injections and assist in adherence. Chooses once to take every 30 vs choosing to take a pill daily. Non-pharmacologic: running out of money, drug supply, and incarceration. Pharmacological: Methadone and buprenorphine(combo of naloxone/buprenorphine is Suboxone). . Buprenorphine: Buprenorphine is a p-opioid partial agonist that has less powerful agonist effects, yet can suppress withdrawal symptoms especially when mild withdrawal has already begun after stopping abused opioids. 1. Sublingual. Several day supply. 2. Can be 6-month implantable or 1 month injection. Naloxone: injection. Narcan(nasal) and zimhi(injection). ce. Alcohol: i. The actions of alcohol on opioid synapses create the rationale for blocking p-opioid receptors with antagonists such as naltrexone(Vivitrol) or nalmefene(Outside the US: Opvee, Zurnai, Revex, and Selincro).