Download The Sheffield RA Models: Etanercept, BSRBR, AHRQ, and DMARDs and more Schemes and Mind Maps Swedish in PDF only on Docsity!
The Sheffield RA Models
Jon Tosh
School of Health and Related Research (ScHARR)
University of Sheffield
PLEASE DO NOT REPRODUCE
Presentation
Introduction
The ScHARR Model(s)
Etanacept Model
BSRBR Model
AHRQ Model
DMARDs Model
Key Assumptions
Conclusions
The ScHARR Model(s)
Individual Patient Sampling (IPS) model
Generates a simulated patient with a set ofcharacteristics
Patient{age,gender,HAQ,disease duration,DMARDs,TNFs}
Evaluates patient’s HAQ score over their lifetime
Estimates total cost and total QALYs
Model runs 000’s patients to estimate mean totalcost and total QALYs
Allows the comparison of alternative treatments
Incorporates uncertainty
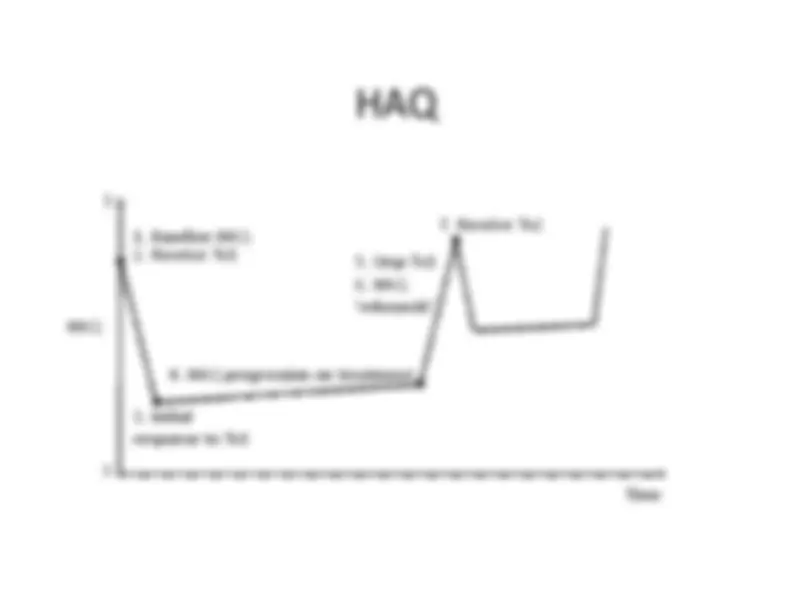
HAQ
Time
HAQ
1. Baseline HAQ 2. Receive Tx1 3. Initialresponse to Tx
4. HAQ progression on treatment
6. HAQ‘rebounds’
7. Receive Tx
5. Stop Tx
Etanercept Model
Parameter Etanercept DMARDs ACR20 response (%) Patient level trial data RCT DMARD arms Treatment withdrawal Observational data Observational data ACR20 HAQ improvement Patient level trial data Trial data mean HAQ improvement • Adjusted for disease duration • Adjusted for ACR20 responders only HAQ progression -responders Trial evidence applied to DMARDbase rate Pooled analysis from systematic review HAQ progression –non-responders ERAS observational data ERAS observational data HAQ ‘rebound’ afterwithdrawal Rebound equal to initial gain Rebound equal to initial gain Healthcare costs Applied linear function between HAQ and costs • Evidence taken from Swedish and US studies Utility Pooled relationship of HAQ to utility taken from four published studies
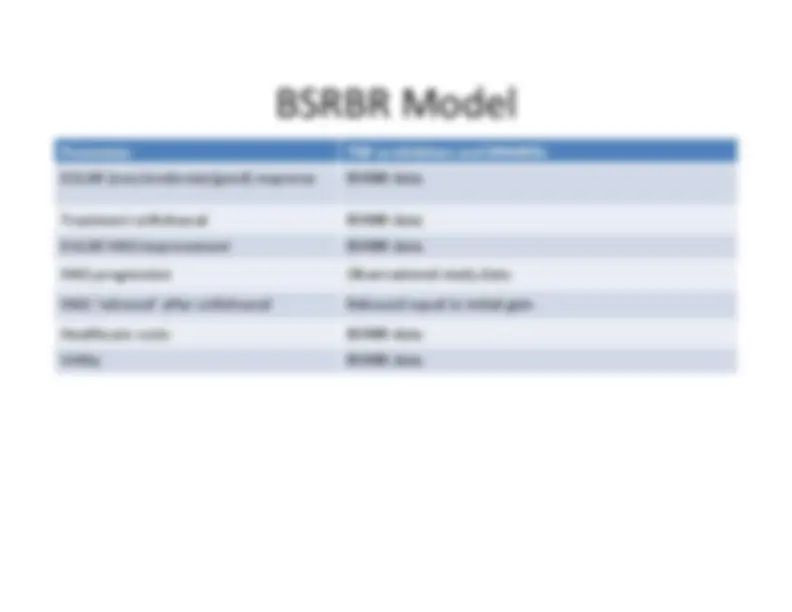
BSRBR Model
Was a research project using the British Societyfor Rheumatology Biologics Registry (BSRBR)dataset
Evaluates TNF-α inhibitors as third line therapy vssequential DMARD therapy
BSRBR provided patient level data
DAS28, HAQ and SF-36 outcomes
Patient level data allowed multivariate analysisfor parameters
TNF-α inhibitors £24k per QALY vs DMARDmonotherapy
AHRQ Model
Was a research project for the MedicarePrescription Drug Improvement andModernization Act (MMA)
Supported by the US Agency for Healthcare Researchand Quality (AHRQ)
Evaluates infliximab, etanercept, adalimumaband anakinra in patients who had not failed abiologic
Incorporates data from the National Databank forRheumatic Diseases (NDB)
Recommends the use of etanercept oradalimumab, and not infliximab or anakinra
AHRQ Model
Parameter TNF-α inhibitors Sub ACR20, ACR20 and ACR Published Mixed Treatment Comparison Treatment withdrawal BSRBR data – multivariate Weibull ACR HAQ improvement Multivariate analysis from the NDB HAQ progression Multivariate analysis from the NDB HAQ ‘rebound’ after withdrawal Rebound equal to initial gain Healthcare costs NDB HAQ to Medicare cost relationship derived Utility Multivariate analysis from the NDB – US EQ-5D
DMARDs Model
Parameter Combination DMARDs Monotherapy DMARD Sub ACR20, ACR20 and ACR50 response Mixed treatment comparison Meta-analysis Treatment withdrawal Trial withdrawal rate with constant risk ACR HAQ improvement AHRQ model analysis HAQ progression Published observational analysis HAQ ‘rebound’ after withdrawal Rebound equal to initial gain Healthcare costs Resource Utilisation Norfolk Arthritis Register (NOAR) HAQ toCost function Utility Published HAQ to EQ-5D function
Key Assumptions (1)
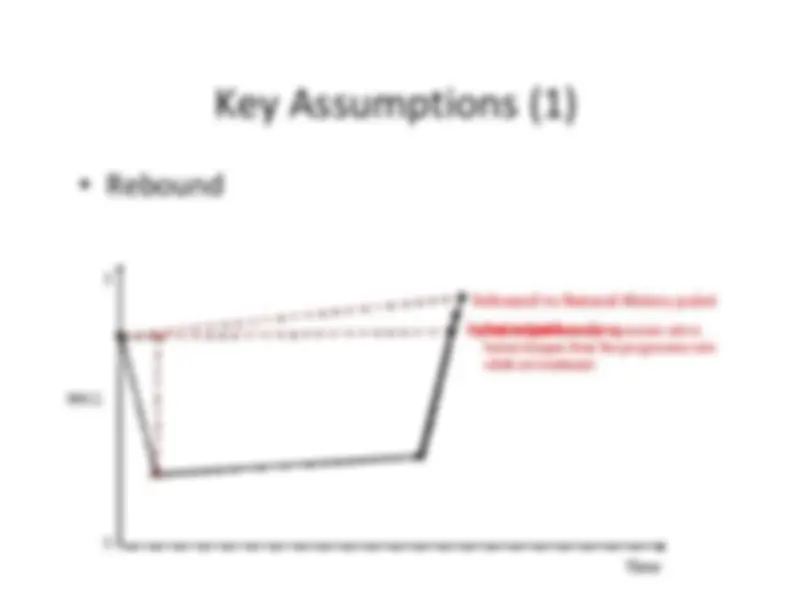
Rebound
Time
HAQ
Equal to gainRebound to baseline
Rebound to Natural History point
The natural history progression rate isfaster/steeper than the progression ratewhile on treatment
Key Assumptions (3)
HAQ
Used to track a patient’s “disease activity”
It is not a preference based measure
Ideal is for Health Related Quality of Life (HRQoL)instruments to be used (EQ-5D, SF-6D)
EQ-5D is preferred by NICE
HAQ correlates well with HRQoL’s
EQ-5D not widely used in international trials
Hence why ‘mapping’ from HAQ to EQ-5D is used,to meet NICE’s Methods Guide
Conclusions
The Sheffield models continue to be used/refined
The HAQ based ‘structure’ allows a flexible model to bedeveloped to meet a clients requirements
Observational data plays a key role in populating RAmodels
The decision space continues to get more complex
More treatment options, and more NICE guidance
Expert input is key at all stages of model development
Conceptual modelling
Population of model
Validation of model
References (1)
Etanercept model
A. Brennan, N. Bansback, A. Reynolds and P. Conway. Modelling the cost-effectiveness of etanercept in adults with rheumatoid arthritis in the UK.Rheumatology 2004. 43: 62-
BSRBR model
A. Brennan, N. Bansback, R. Nixon, J. Madan, M. Harrison, K. Watson, and D.Symmons. Modelling the cost effectiveness of TNF-α antagonists in themanagement of rheumatoid arthritis: results from the British Society forRheumatology Biologics Registry. Rheumatology 2007. 46(8):1345-
AHRQ model
A. J. Wailoo, N. Bansback, A. Brennan, K. Michaud, R. Nixon, F. Wolfe. Biologicdrugs for rheumatoid arthritis in the medicare program: A cost-effectivenessanalysis. Arthritis & Rheumatism. 2008. 58(4):939-
DMARDs model
Journal paper under review
Analysis published in NICE Clinical Guideline (CG79) Rheumatoid Arthritis inAdults. (see NICE website)
References (2)
Bayesian Clinical Trial Simulation in RA
Uses Bayesian clinical trial simulation methods to evaluate theprobability of drug registration based on uncertain parameters
R. Nixon, A. O’Hagan, J. Oakley, J. Madan, J. W. Stevens, N.Bansback, A. Brennan. The Rheumatoid Arthritis DrugDevelopment Model: A case study in Bayesian clinical trialsimulation. Pharmaceutical Statistics 2009;8:371-89.
Statin Therapy in RA
Evaluates the cardiovasular and anti-rheumatic benefits ofstatins
Incorporates Value of Information analysis
N. Bansback, R. Ara, S. Ward, A. Anis, H. K, Choi. Statin therapyin rheumatoid arthritis: a cost-effectiveness and value-of-information analysis. Pharmacoeconomics. 2009;27(1):25-