Download WGU D116 FNP Comprehensive Pharmacology Study Guide 100 % correct and more Exams Advanced Education in PDF only on Docsity!
Symbol Key:
✅ = First-Line Drug
⚠️ = Pregnancy Category X (Contraindicated in Pregnancy)
☠️ = Black Box Warning (BBW)
WGU D116 FNP Comprehensive Pharmacology Study Guide
ADVANCED PRACTICE NURSING
FNP Comprehensive Pharmacology Study Guide
Family Nurse Practitioner Board Exam Reference
Prepared for: Brandon | Date: May 13, 2026 | River Oaks, TN For use as a comprehensive board review reference. Covers all major pharmacology modules for FNP certification preparation.
TABLE OF CONTENTS
1. APRN Prescribing Framework — Rational Drug Selection, Adherence, Cost
2. Pharmacogenomics & CYP System — SNPs, Haplotypes, CYP Enzyme Tables
3. Cardiovascular Drugs — Antihypertensives, Heart Failure, Anti-dysrhythmics, Lipids
4. Blood Disorders — Anticoagulants, Antiplatelets, Anemia
5. Obesity / Anorexiants / CNS — Anorexiant Drugs, Serotonin Syndrome, MAOI Interactions
6. Gastrointestinal Drugs — Antacids, H2 Blockers, PPIs, Diabetes Medications
7. Thyroid & Adrenal — Lab Interpretation, Drug Treatment
8. Reproductive / Hormones — Testosterone, Estrogens, STIs, UTIs
9. Antivirals / HIV — Drug Classes, MOA, Interactions
10. Dermatology — Topical Corticosteroids — Potency Classes, Indications
★ = High-Yield Board Topic
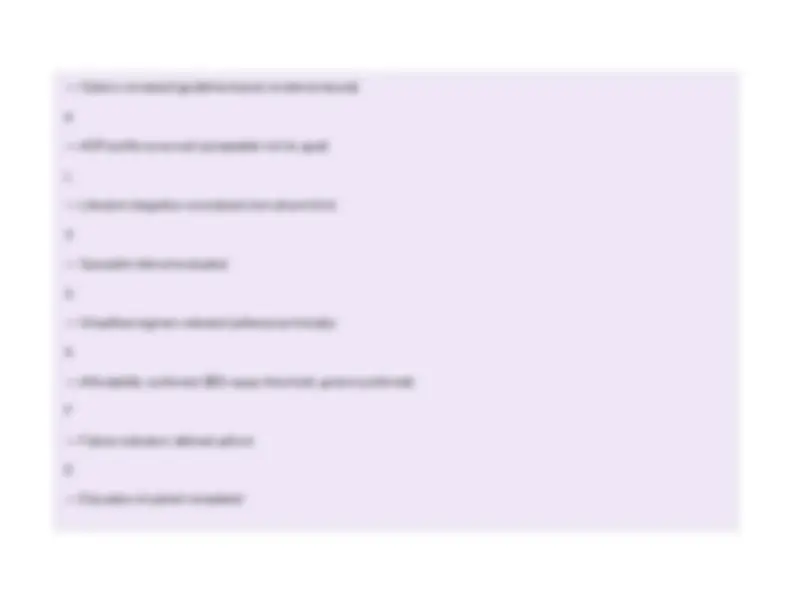
🧠 Mnemonic — "GOALS-SAFE" Rational Drug Selection Framework
G
— Goal of therapy defined (cure vs. chronic control)
O
Clinical Question Key Consideration for APRN Is there a clear indication? Must establish diagnosis before prescribing; avoid empiric prescribing without clinical basis What drugs are effective? Review nationally recognized guidelines (AHA, ACC, JNC, ADA, etc.); use evidence-based resources (Micromedex, Lexicom, Epocrates) What is the therapeutic goal? Cure vs. control vs. palliation — this changes the acceptable risk-benefit profile What indicates drug failure? Define outcome markers upfront (lab values, symptom thresholds, functional measures) Is a specialist needed? Recognize scope boundaries; refer appropriately for complex pharmacotherapy Are there drug duplications? Reconcile all medications; avoid therapeutic duplication and additive ADR risk Is there an OTC equivalent? Prefer OTC if equally effective and more affordable; reduces cost barriers to adherence What is the cost / insurance coverage? (^) $50 copay threshold — adherence drops significantly above this amount; generic preferred What are the ADR risks? If goal = cure: side effects more tolerable; if goal = chronic management: SE, cost, lifestyle fit are critical Can lifestyle replace or augment? Always combine with lifestyle + non-pharm approaches; rely on communication, education, nutrition Is the regimen adherence-friendly? Simplify dosing schedules; complex regimens reduce adherence; once-daily preferred Are there restricted prescribing rules? Pay attention to drugs NPs cannot prescribe in your state; newest is not always best
— Options reviewed (guideline-based, evidence-based)
A
— ADR profile assessed (acceptable risk for goal)
L
— Lifestyle integration considered (non-pharm first)
S
— Specialist referral evaluated
S
— Simplified regimen selected (adherence-friendly)
A
— Affordability confirmed ($50 copay threshold; generic preferred)
F
— Failure indicators defined upfront
E
— Education of patient completed
Key Facts: Single-Nucleotide Polymorphisms (SNPs — "Snips")
- 99.9% of nucleotide bases are identical in all humans; the 0.1% difference accounts for ~3 million nucleotide differences
- 80% of human genetic variation is due to SNPs SECTION 2: PHARMACOGENOMICS & CYP SYSTEM
Pharmacogenomics is the branch of pharmacology studying how genetic variation influences drug response. It
correlates gene expression with drug efficacy and toxicity to optimize drug combinations for individual genetic makeup.
The ultimate goal is development of prediction models to forecast adverse events in specific individuals before
prescribing.
2A. SNP Key Facts
- Drug selection must always be based on clinical judgment + diagnosis + assessment
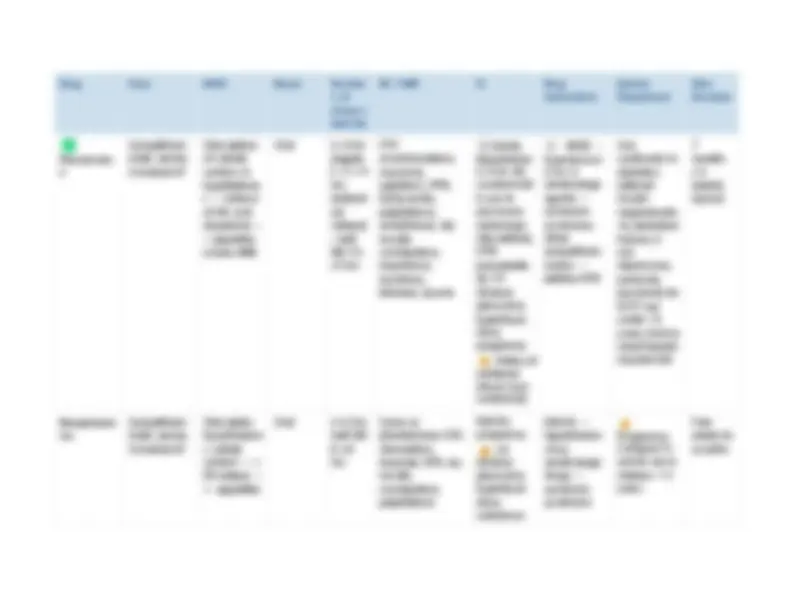
2B. SNP Types & Clinical Impact SNP Type Location Effect on Protein Clinical Impact Linked SNP Outside the gene No direct effect on protein production or function Used as genetic markers; no direct drug response impact Non-coding Causative SNP Inside the gene (non-coding region) Changes amount of protein produced (over/under-expression) Altered enzyme expression → changed drug metabolism rates Coding Causative SNP Inside the gene (coding region) Changes amino acid sequence → structural change in protein Altered enzyme function → poor, intermediate, or ultra-rapid metabolizer phenotype 2C. Warfarin CYP2C9 Variants ★
- 1.4 million locations where SNPs occur in humans
- A variation must be present in at least 1% of the population to be classified as a SNP
- SNPs are responsible for: drug response, physical appearance, disease susceptibility
- Example: Normal = AGCT; SNP = ATCT (single base change)
- Haplotype : each combination of SNPs = one haplotype; one inherited from mother + one from father = haplotype pair
2D. Major CYP Enzyme Table ★
CYP3A4 is the
largest family of CYP enzymes
, metabolizing approximately 50% of all drugs. Understanding key substrates, inducers, and inhibitors is critical for
preventing drug interactions.
CYP
Enzyme Major Drug Substrates Key Inducers (↑ metabolism → ↓ drug level) Key Inhibitors (↓ metabolism → ↑ drug level) CYP2C9 Warfarin, phenytoin, tolbutamide, NSAIDs (ibuprofen, celecoxib), losartan, glipizide Rifampin, carbamazepine, phenobarbital, St. John's Wort Fluconazole, amiodarone, fluvastatin, metronidazole, sulfonamides CYP3A4 Statins (except pravastatin), cyclosporine, tacrolimus, benzodiazepines, CCBs, HIV PIs, many opioids, erythromycin, carbamazepine Rifampin, carbamazepine, phenytoin, phenobarbital, St. John's Wort, dexamethasone Ketoconazole, itraconazole, erythromycin, clarithromycin, grapefruit juice, ritonavir, amiodarone, diltiazem, verapamil CYP2D6 Codeine (→ morphine), tramadol, TCAs, SSRIs (paroxetine, fluoxetine), antipsychotics (haloperidol), beta-blockers (metoprolol, carvedilol), tamoxifen Rifampin (weak inducer); dexamethasone Fluoxetine, paroxetine, bupropion, quinidine, amiodarone, cinacalcet CYP2C19 Clopidogrel (prodrug activation), PPIs (omeprazole, Rifampin, carbamazepine, St. Omeprazole, esomeprazole, fluoxetine,
🧠 Mnemonic — CYP Inhibitors vs. Inducers
Inhibitors: "AMIGOS Kill Enzymes"
A
miodarone
M
etronidazole
I
CYP
Enzyme Major Drug Substrates Key Inducers (↑ metabolism → ↓ drug level) Key Inhibitors (↓ metabolism → ↑ drug level) lansoprazole), diazepam, phenytoin, citalopram, escitalopram John's Wort fluvoxamine, ticlopidine, ketoconazole CYP1A2 Caffeine, theophylline, clozapine, olanzapine, tacrine, warfarin (minor), acetaminophen Cigarette smoke, omeprazole (weak), rifampin, cruciferous vegetables Ciprofloxacin, fluvoxamine, cimetidine, amiodarone
arbamazepine
B
arbiturates (phenobarbital)
A
lcohol (chronic)
R
ifampin
S
t. John's Wort
Remember: Inhibitors INCREASE drug levels (toxicity risk); Inducers DECREASE drug levels (therapeutic failure risk)
SECTION 3: CARDIOVASCULAR DRUGS
Cardiovascular pharmacology is among the highest-yield areas on the FNP board exam. Drugs are grouped by
indication. The autonomic nervous system forms the physiologic backbone: the sympathetic system (epinephrine,
norepinephrine, dopamine) and parasympathetic system (acetylcholine) govern cardiac and vascular tone.
Understanding receptor selectivity is essential for drug selection.
💎 Clinical Pearl: Pharmacogenomics in Practice
- Poor metabolizers of CYP2D6 cannot convert codeine to morphine → no analgesia; conversely, ultra-rapid metabolizers may experience toxicity
- Clopidogrel is a prodrug requiring CYP2C19 activation — poor CYP2C19 metabolizers (e.g., with PPI use) have reduced antiplatelet effect → increased thrombosis risk ★
- Pharmacogenomic testing (SNP panels) can guide warfarin dosing, antidepressant selection, and oncology drug choice
- CYP3A4 metabolizes ~50% of all marketed drugs — most clinically significant interactions involve this enzyme
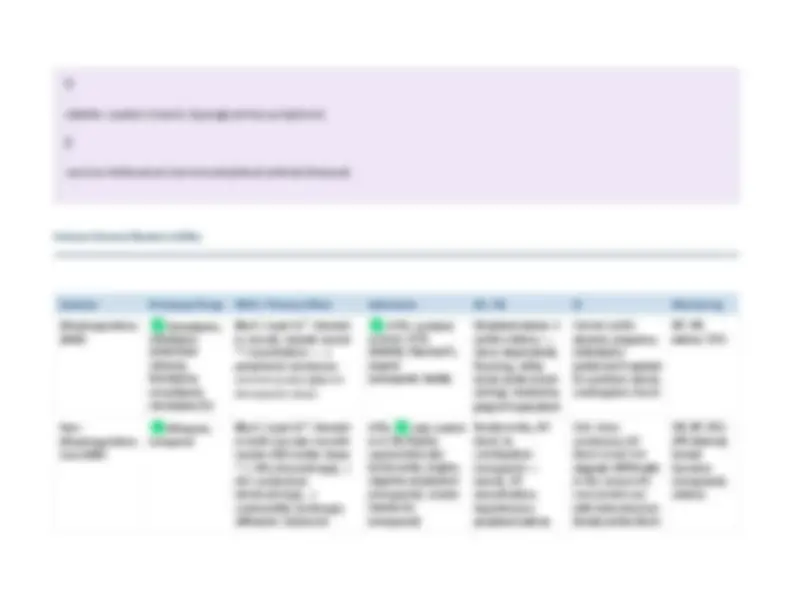
Feature Details Prototype Drugs (^) Hydrochlorothiazide (HCTZ) , chlorthalidone, indapamide, metolazone MOA Inhibit NaCl reabsorption in the distal convoluted tubule → natriuresis → reduced plasma volume → reduced peripheral vascular resistance with chronic use Indications (^) First-line uncomplicated HTN; edema; osteoporosis (calcium-sparing); heart failure (adjunct) SE / AE Hypokalemia^ ★, hyponatremia, hyperglycemia, hyperuricemia (gout), hyperlipidemia (transient), hypercalcemia, sexual dysfunction, photosensitivity Contraindications Anuria; sulfonamide allergy (relative); gout (relative); pregnancy (can use if necessary) CYP Interactions Not significantly metabolized by CYP; NSAIDs reduce efficacy; lithium toxicity increased (↓ renal clearance) Special Considerations Preferred in African American patients (without DM/CKD); less effective if GFR <30 mL/min; chlorthalidone preferred over HCTZ (longer duration, outcomes data) Monitoring BMP (K+, Na+, glucose, Cr/BUN), uric acid, lipid panel; BP response in 4 – 6 weeks Loop Diuretics Feature Details Prototype Drugs (^) Furosemide , torsemide, bumetanide, ethacrynic acid MOA Inhibit Na+/K+/2Cl− co-transporter in the thick ascending limb of Loop of Henle → potent diuresis; most powerful diuretics Indications Acute pulmonary edema, CHF with volume overload, cirrhotic ascites, hypercalcemia, hypertensive urgency, CKD with fluid overload (effective even at low GFR) SE / AE (^) Hypokalemia ★(worse than thiazides), hyponatremia, hypomagnesemia, hypocalcemia, metabolic alkalosis, ototoxicity
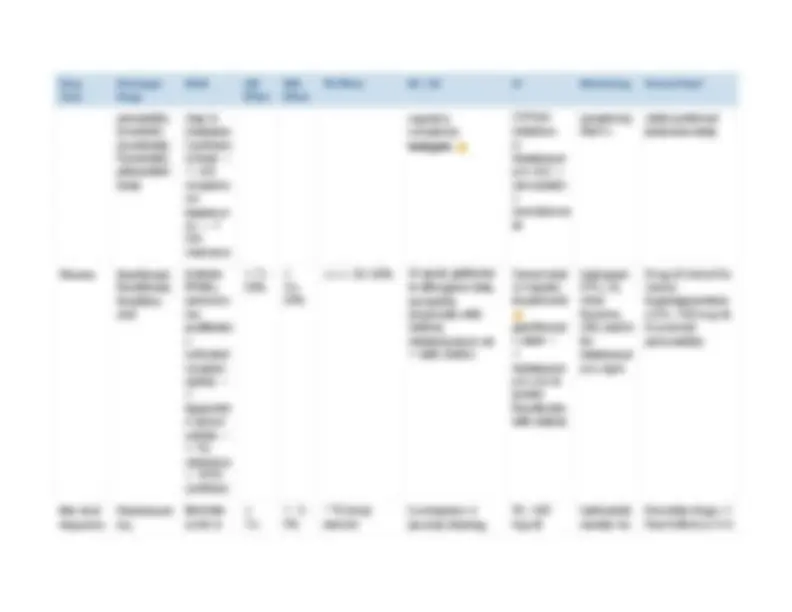
Feature Details (especially high doses/rapid IV), hyperuricemia, dehydration, hypotension Contraindications Anuria; sulfonamide allergy (furosemide; use ethacrynic acid instead); severe electrolyte depletion CYP Interactions NSAIDs reduce efficacy; aminoglycoside co-use → additive ototoxicity; digoxin toxicity risk with hypokalemia Monitoring BMP (electrolytes, Cr/BUN), daily weights, I&O, BP, hearing (with IV doses) Potassium-Sparing Diuretics Feature Details Prototype Drugs Spironolactone (aldosterone antagonist), eplerenone; Triamterene , amiloride (direct ENaC blockers) MOA Spironolactone/eplerenone: competitively antagonize aldosterone at collecting duct → retain K+, excrete Na+; Triamterene/amiloride: directly block sodium channels (ENaC) in collecting duct Indications (^) HF with reduced EF (spironolactone, eplerenone — mortality benefit); primary hyperaldosteronism; ascites; hypokalemia prevention; adjunct HTN; used with thiazide/loop to prevent K+ loss SE / AE Hyperkalemia^ ★^ (life-threatening), gynecomastia/breast tenderness (spironolactone^ —^ less with eplerenone), menstrual irregularities, metabolic acidosis Contraindications Hyperkalemia, severe renal insufficiency (K+ retention risk), concurrent use of ACE inhibitors + ARBs (triple therapy — avoid) Monitoring BMP (K+, Na+, Cr/BUN) in 1 – 2 weeks after initiation; renal function ACE Inhibitors ★
Angiotensin II Receptor Blockers (ARBs) Feature Details Prototype Drugs (^) Losartan , valsartan, candesartan, irbesartan, olmesartan, telmisartan, azilsartan (all end in "-sartan") MOA Selectively block AT1 angiotensin II receptors → ↓ vasoconstriction, ↓ aldosterone → ↓ BP; does NOT affect ACE → no bradykinin buildup → NO cough Indications (^) HTN, CKD/DM nephropathy, HF (ACE intolerance), post-MI LV dysfunction SE / AE (^) Hyperkalemia, hypotension (first dose), dizziness, fetopathy ; angioedema (rare — less than ACE inhibitors) Contraindications (^) Pregnancy, bilateral renal artery stenosis, hyperkalemia; do NOT combine with ACE inhibitor (dual RAAS blockade — ↑ AKI, hyperkalemia risk) CYP Interactions Losartan metabolized by CYP2C9 → fluconazole/rifampin interactions; NSAIDs reduce efficacy Monitoring BMP (K+, Cr/BUN), BP; no need to monitor for cough Renin Inhibitors (Direct Renin Inhibitor) Feature Details Prototype Drug Aliskiren (Tekturna) MOA Directly inhibits renin (first enzyme in RAAS) → prevents conversion of angiotensinogen to Ang I → ↓ entire RAAS cascade
Feature Details Indications HTN (monotherapy or combination); rarely used as primary agent SE / AE (^) Hyperkalemia, diarrhea, hypotension, rarely angioedema; teratogenic Contraindications (^) Pregnancy; concurrent use with ACE inhibitor or ARB in patients with DM or CKD (FDA black box warning); GFR <60 + ACE/ARB Monitoring BMP (K+, Cr/BUN), BP Central Alpha- 2 Agonists Feature Details Prototype Drugs Clonidine (Catapres), methyldopa (Aldomet), guanfacine, guanabenz MOA Stimulate alpha- 2 adrenergic receptors in the brainstem → inhibit cardioacceleration and vasoconstriction centers → ↓ peripheral outflow of NE → ↓ peripheral resistance, ↓ renal vascular resistance, ↓ heart rate, ↓ BP Indications (^) Methyldopa: HTN in pregnancy (safest); Clonidine: HTN, ADHD (guanfacine), opioid/nicotine withdrawal, hypertensive urgency; menopausal hot flashes SE / AE Sedation ★, dry mouth, bradycardia, orthostatic hypotension; clonidine: rebound hypertension with abrupt withdrawal ★; methyldopa: positive Coombs test, hemolytic anemia, hepatotoxicity Contraindications Clonidine: caution in depression; methyldopa: active liver disease; both: avoid abrupt discontinuation Monitoring BP, heart rate, sedation level, LFTs (methyldopa), CBC (methyldopa — Coombs/hemolytic anemia) Alpha- 1 Blockers (Selective Alpha- 1 Antagonists)