Download All about Hematology II and more Lecture notes Hematology in PDF only on Docsity!
HemaTOLOGY II
HEMATOLOGY 2
HEMOSTASIS
Maintenance of blood flow within the vascular system
Participants of primary hemostasis may also participates in secondary
hemostasis and vice versa
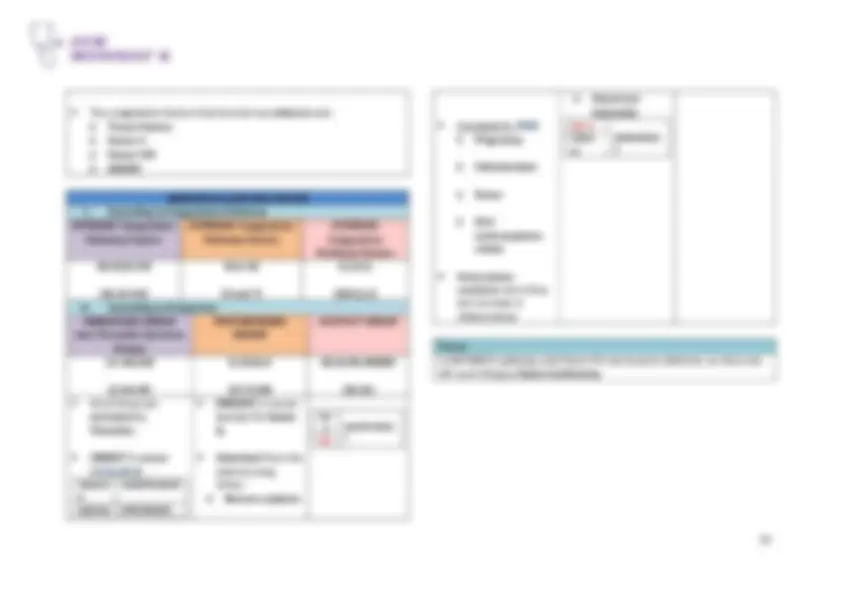
Important Considerations In Blood Collection For Hemostasis Testing:
If the patient has many bruises or mentions a tendency to bleed (a reason to expect excessive bleeding), the phlebotomist should extend the time for observing the venipuncture site from 1 to 5 minutes and should apply a pressure bandage before dismissing the patient.
Factors V and VIII Considered as labile factors (easily destroyed)
Cold temperature (1 to 6 OC) storage (placing plasma specimen in ref): Causes precipitation of: Von Willebrand factor Activation of: Factor VII (7)
Destruction of: Platelets
Storage temp for EDTA tubes (for CBC) : REF. TEMP
0.105 to 0.109 M (3.2%) buffered Sodium Citrate Found in LIGHT BLUE TOP tubes (inverted for 3-4 times) Excessive inversion may activate the platelets which may lead to shortening of clotting times
Ratio of anticoagulant : blood is 1:
May INCREASE the stability of factors V and VIII
Preferred anticoagulant for coagulation test
Citrate, Theophylline, Adenosine, Dipyridamole (CTAD) Found in LIGHT BLUE TOP tubes (ACD may also be seen in yellow tube)
For platelet functions assays PF4 (Platelet factor- 4 ) and β -TG assays (Beta-thromboglobulin) From alpha granules of platelets
Factors that may affect coagulation test results (PT and/or APTT): Shortened Test Results:
Hemolysis
Excessive agitation
Prolonged tourniquet application
Excessive needle manipulation
Platelet contamination
Prolonged Test Results:
Presence of clots (clotting factors has been consumed)
HemaTOLOGY II
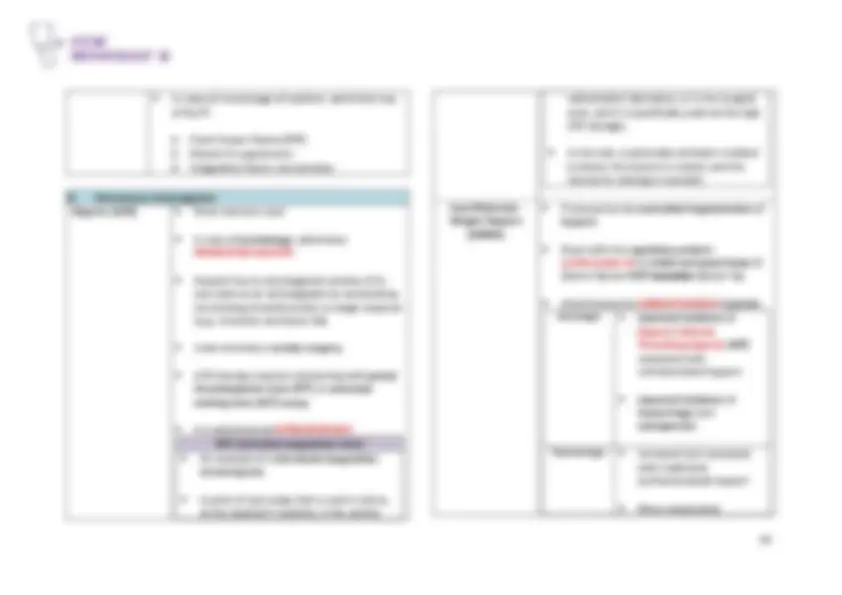
Increased AC concentration
Caused by: Short draw Elevated hematocrit (>55%) Notes: Phlebotomist must provide tubes with relatively decreased anticoagulant volumes for collection of blood from a patient whose hematocrit is high.
The following formula may be used for the adjustment: C = (1.85 X 10*) (100-H) The answer we will get is the Volume of anticoagulant to use where: C is the volume of sodium citrate in milliliters, V is volume of whole blood-sodium citrate solution in milliliters, H is the hematocrit in percent
There is NO evidence suggesting a need for increasing the volume of anticoagulant for specimens from patients with anemia, even when the hematocrit is < 20%.
Sample problem: To collect 5 mL of blood and anticoagulant mixture from a patient whose hematocrit is 65%, calculate the volume of sodium citrate as follows: C = (1.85 X 10 3) (100-H) V C = (0.00185)(100-65) x 5.0 mL C = (0.00185)(35) x 5.0 mL
C = 0.32mL of 3.2% sodium citrate
REMEMBER: Volume of anticoagulant can be adjusted if the patient’s hematocrit is >55%
**1mL – 0.32 mL = 0.68mL is the volume of anticoagulant to REMOVE
Related Terms: Thrombosis Pathological formation of blood clots in veins or arteries that obstruct blood flow Antithrombotics Used to prevent thrombosis includes: Antiplatelets Suppress platelet activation Anticoagulant Suppress coagulation . Examples of Antiplatelet Drugs: Aspirin Inhibits cyclooxygenase (enzyme inside the platelets) Clopidogrel and Prasugrel
Bind platelet P2Y 12 (ADP receptor)
Prevent platelet activation Abciximab and Tirofiban
Bind GP IIb/IIIa (fibrinogen receptor)
Block fibrinogen from binding to platelets to avoid platelet aggregation Examples of Anticoagulants: Warfarin (Coumadin)
Inhibits synthesis of factors II,VII,IX,X (2,7,9,10)
Heparin (UFH) (^) Accelerates the binding of antithrombin to thrombin and factor Xa
HemaTOLOGY II
Hemostasis Specimen Storage Times and Temperatures Application Temperature Time PT with NO unfractionated heparin (UFH) in specimen
18 to 24OC 24 hours
PTT with NO unfractionated heparin (UFH) in specimen
18 to 24 OC 4 hours
PTT for monitoring UFH therapy 18 to 24 OC Separate within 1 hour,
test within 4 hours PT when UFH is present in specimen
18 to 24 OC Separate within 1 hour,
test within 4 hours Storage of LIGHT BLUE TOP Not stored in refrigerator because this will cause destruction of platelets and activation of factors VII
Two Stages of Hemostasis: PRIMARY SECONDARY Involves the following: Constriction of damages blood vessels
Formation of platelet plugs
Formation of fibrin meshwork through activated coagulation factors
Inhibition of activated coagulation factors Key participants: Blood vessels Platelets
Coagulation factors
Note: They can participate in other stages
HemaTOLOGY II
PRIMARY HEMOSTASIS
BLOOD VESSELS
A. 3 coats (tunics) composing the tissue in a blood vessel wall: 1.) TUNICA INTIMA Also known as tunica interna
Endothelium — simple squamous epithelium lining the blood vessels
Forms the smooth glistening surface of endothelium that lines the inner tubular cavity (lumen) 2.) TUNICA MEDIA Composed of smooth muscle and elastic fiber
Thickest coat 3.) TUNICA ADVENTITIA
Also known as tunica externa
Outermost coat
Composed of fibrous connective tissue that contains autonomic nerve endings and the vasa vasorum (small networks of blood vessels that supply nutrients to the tissues of the wall). B. Types of Blood Vessels Arteries (size: 4 mm)
Distributing blood vessels that LEAVE the heart
Have the thickest walls of the vascular system
Arterioles (30 um}: microscopic continuation
of arteries that give off branches called metarterioles, which in turn join the capillaries Veins (5 mm)
Collecting blood vessels that RETURN to the heart
Larger, have a more irregular lumen than arteries
Venules (size: 20 um} — microscopically sized veins;
connect the capillaries to the veins Capillaries (8 um)
Blood passes from the arterial to the venous system via the capillaries
Capillaries are the thinnest walled and most numerous of the blood vessels.
Composed of only one cell layer of simple squamous epithelium (unlike the vessels of the arterial and venous systems), which permits a more rapid rate of transport of materials between blood and tissue.
Sinusoids — specialized types of capillaries found in locations such as the bone marrow, spleen and liver
HemaTOLOGY II
Plasmin Aka: Fibrinolysin (enzyme) Enzyme that dissolves clot
von Willebrand Factor (vWF)
Major Functions:
- Aids in platelet adhesion
- Acts as a carrier protein for factor VIII Sites of Synthesis:
- Endothelial cells
- Megakaryocytes Sites of Storage:
- Weibel-Palade bodies (found in blood vessels)
- Alpha granules (found in platelets)
Newly made and long vWF is ULVWF that will cause thrombosis
ADAMTS 13 : Enzyme that cuts long vWF ADAMTS 13 A Disintegrin and Metalloproteinase with a Thrombospondin Type 1 motif, Member 13
aka: vWF – cleaving protease
a plasma enzyme secreted by the:
regulates the size of circulating VWF by
cleaving ultra-long VWF multimers (ULVWF) into shorter segments (have less hemostatic potential)
Thrombotic Thrombocytopenic Purpura (TTP)= caused by deficiency of ADAMTS-
↓Platelets ↑Clots
PLATELETS
aka: THROMBOCYTES
Arise from a bone marrow cell called megakaryocytes important in both primary and secondary hemostasis described as cells with granular cytoplasm but no nuclear material platelets cluster with the RBCs near the center of the blood vessel platelets move back and forth with the WBCs from venules into the white pulp of the spleen
LIFE SPAN: 9 - 10 DAYS
On a Wright-stained PBS: Platelets are spread throughout the RBC monolayer (7 to 21 cells per 100x field)
Platelets have an average diameter of 2.5 um (or, 2 to 4 um)
3 major functions:
- To form an aggregate plug of platelets that can slow down or
HemaTOLOGY II
stop blood loss
- To participate in plasma coagulation
- To preserve the endothelial lining of the blood vessels Reticulated Platelets
aka: stress platelets
Appear in compensation for thrombocytopenia
newly released from megakaryocytes and still contain RNA
Markedly larger than the usual platelets (diameter in PBS: exceeds 6 um [MPV reaches 12 to 14 fL])
Clinical use: Can help differentiate bone marrow failure from peripheral destruction in thrombocytopenia
Early predictor of bone marrow recovery after chemotherapy and transplantation
Potentially prothrombotic (may be associated with increased risk of cardiovascular disease)
SIZE OF THE PLATELETS
Normal: 2.5 um (average)
Mean Platelet Volume (MPV)
Reference Range: 6.8 to 10.2 fL
Average volume of individual platelets in a specimen
EDTA causes swelling of platelets (causes approximately 20% increase in MPV during the first hour).
Should be based on EDTA specimens that are between 1 to 4 hours old
Examples of disorders characterized by: Small Platelets Large/ Giant Platelets WAS (Wiskott-Aldrich Syndrome) Inheritance: X-linked recessive
Some of the characteristics: Small platelets Eczema Thrombocytopenia (↓) DENSE granule def.
TORCH infections Toxoplasma Other agents Rubella virus Cytomegalovirus Herpesvirus
BSS (Bernard-Soulier Syndrome) Inheritance: Autosomal recessive
Some of the characteristics: Giant platelets Thrombocytopenia (↓) Gp Ib/IX/V complex def.- primary platelet surface receptor for vWF
Defect in platelet adhesion
HemaTOLOGY II
Cytoplasm of Platelets On a Wright-stained PBS, platelets appear lavender and granular
2 General parts: Chromomere (^) Aka Granulomere
Centrally located
Granular Hyalomere Peripherally-located
Non-granular .
Megakaryocytopoiesis aka MEGAKARYOPOIESIS
process by which megakaryocytes develop
Thrombopoietin (TPO) Major regulator of platelet production
Produced primarily by: LIVER
MPL- TPO receptor site
MEGAKARYOCYTES Largest cell in Bone Marrow (size: 30 - 50 um)
<0.5% of all bone marrow cells
2 - 4 megakaryocytes per 10x LPF Megakaryocytes Progenitors Progenitor cell is an immature hematopoietic cell that CANNOT be recognized using the light microscope (you will not be able to know to which cell line does it belong)
All of the following resemble LYMPHOCYTES MFU-Meg Least mature
Participates in normal mitosis
Burst forming unit CFU-Meg (^) Participates in normal mitosis
Colony Forming Unit LD-CFU-Meg (^) Light Density Colony Forming Unit
Most mature
Loses its capacity to divide
Performs endomitsosis (nuclear division WITHOUT cytoplasmic divisions .
3 Precursors of Megakaryocytes Precursor cells an immature hematopoietic cell but can already be recognized under light microscope
HemaTOLOGY II
Megakaryoblast (MK-I)
Most immature
Promegakaryocyte (MK-II) Megakaryocyte (MK-III)
Most abundant
Easily recognized (basis is size: 30 - 50 um)
One megakaryocyte may shed 2000 - 4000 platelets
PLATELET SHEDDING
Aka: thrombopoiesis, thrombocytopoiesis
Demarcation system (DMS)= Ultimately delinates individual platelets during thrombocytopoiesis
HemaTOLOGY II
of blood (well-mixed) into 1,980 uL of 1% ammonium oxalate
- Mix the dilution properly and charge the counting chamber. (NOTE: A special thin, flat-bottomed hemocytometer is used for phase-microscopy platelet counts.)
- The charged hemocytometer is then placed in a moist chamber for 15 minutes to allow the platelets to settle.
(MOIST CHAMBER = may be prepared by placing a piece of damp filter paper in the bottom of a Petri dish. An applicator Stick broken in half can serve as a support for the hemocytometer.)
For manual WBC count the charged hemocytometer must stay in a moist chamber for 10 minutes
- Platelets are counted using the 40x objective lens (400x total magnification). To distinguish the platelets from highly refractile dirt and debris, one must remember the platelets’ characteristics when they are seen using a phase-contrast microscope. The platelets have the following characteristics: Diameter: 2 – 4um Shape : Round to Oval Color: Light purple sheen
(NOTE: “ Ghost ” erythrocytes are frequently seen in the background.)
- Platelets are counted in the 25 small squares of the central large square ( 1 mm^2 ) of the hemocytometer. On the other side
of the counting chamber, repeat the counting process. IMPORTANT:
o Difference between the total cells counted on each side should be < 10%.
o Greater difference could indicate uneven distribution (requires that the procedure be repeated)
o Formula for percentage difference :
V1= larger no. V2= smaller no.
- Average the number of platelets counted on the two sides. Using the average, compute the PLT count using the following formula:
(Reminder: This is the general formula used for manual cell counts and can be used to compute any type of cell count.)
Usual dilution factor = 100
Average
HemaTOLOGY II
Area (mm^2 )= 1
Sample Problem: Platelets counted (one side): V1= 208 Platelets counted (another side): V2= 200
Solution: Percentage difference :
Average: 208+200= 204
Platelet count:
or
204 X10^9 / L
A normal (wedge) blood smear should demonstrate approximately 7 to 21 cell per 100x field
For estimation of the platelet count:
Scan ten (10) of oil immersion fields for the number of platelets Average number of platelets/ OIF x 20,000 = ESTIMATED plt ct. per uL In occasions of significant anemia or erythrocytosis, use the following formula for the platelet estimate:
***** 200-** average number of RBCs per oil immersion field in the optimal assessment area
Estimates may be reported PLATELET ESTIMATE OF REPORT AS: 0 to 49,000 /uL Marked decrease 50,000 to 99,000 /uL Moderate decrease 100,000 to 149,000 /uL Slight decrease 150,000 to 199,000 /uL Low Normal 200,000 to 400,000 /uL Normal 401,000 to 599,000 /uL Slight Decrease
B. Platelet Aggregometry PLATELET AGGREGOMETRY LIGHT-TRANSMITTANCE (OPTICAL) PLATELET AGGREGOMETRY Designed to test Platelet-Rich Plasma (plasma with a platelet count of 200,000 to 300, 000/uL )
To prepare PRP: Sodium citrate -anticoagulated blood is checked visually for clots
Then it is centrifuged at 50 x g for 30 minutes with the stopper in place to maintain the pH.
HemaTOLOGY II
DISORDERS OF PRIMARY HEMOSTASIS
Vascular Disorders
General laboratory test results: NORMAL RESULTS in these tests = (^) Platelet Count Platelet Function Test Coagulation Test ABNORMAL RESULTS in these tests= (^) Bleeding Time (prolonged)
Rumple-Leede Test . VASCULAR DISORDERS COMMENTS Hereditary Hemorrhagic Telangiectasia
(a.k.a. Osler-Weber- Rendu Disease )
Most common inherited vascular bleeding disorder
Inherited as Autosomal Dominant
Characterized by localized dilation of capillary walls (skin & mucous membrane) Ehlers-Danlos Syndrome
(a.k.a. Cutis Hyperelastica )
Characterized by hyperextensible joints , hyperplastic skin
Inherited as Autosomal Dominant
Marfan's Syndrome (^) Characterized by: skeletal defects (long extermities), arachnodactyly (“spider fingers)
Inherited as Autosomal Dominant
Senile Purpura (^) Characterized by the presence of bruised areas on the forearms of elderly persons (due to degeneration of collagen ) Henoch-Schonlein Purpura
(a.k.a.: Allergic Purpura or Nonthrombocytopenic Purpur a)
Most commonly seen in children - vascular abnormalities : most probably caused by immunologic damage to the endothelial cells
Characterized by gastrointestinal hemorrhage and joint swelling
Waterhouse- Friderichsen Syndrome
Characterized by severe capillary damage following meningococcal septicemia
Kasabach-Meritt Syndrome
(a.k.a. Congenital Hemangiomata )
Associated with tumors composed of vessels that commonly swell and bleed at the surface
Scurvy
(a.k.a. Ascorbic acid (Vitamin C) deficiency )
Characterized by defects in the synthesis of collagen and hyaluronic acid
Vitamin C is important for the integrity of blood vessel wall
So deficient vitamin C can lead to patient easily bleeding due to weakened blood vessel
HemaTOLOGY II
Does not manifest an abnormality in platelet count, platelet function test nor in coagulation test
Prolonged bleeding time
Abnormal Rumple-Leede test . Note: General results seen in vascular disorders: Prolonged bleeding time Abnormal Rumple-Leede test
Platelet Disorders A. QUANTITATIVE THROMBOCYTOPENIA ( decreased platelet count ) Examples of conditions with: Impaired or Decreased Platelet Production
Decrease production of platelets in BM Bernard-Soulier syndrome
Deficiency of GP Ib/IX/V
Autosomal Recessive disorder
Giant platelets
Thrombocytopenia ↓ Fanconi anemia Characterized by: Aplastic anemia
Cancer susceptibility
Chromosomal abnormalities
Physical abnormalities: Thumb malformations
Skin abnormalities
Short stature TAR syndrome (^) Thrombocytopenia with Absent Radius (TAR)
Inherited disorder
Viral infections
Leukemia
Megaloblastic anemias
WAS
(Wiskott-Aldrich syndrome)
Small platelets
MYHS9 gene mutations Group of disorders: Fechtner syndrome Sebastian syndrome Epstein syndrome May-Hegglin Anomaly
HemaTOLOGY II
Cirrhosis of the liver A late stage of scarring (fibrosis) of the liver caused by many forms of liver diseases and conditions Portal hypertension Portal hypertension is an increase in the pressure within the portal vein (the vein that carries blood from the digestive organs to the liver). The increase in pressure is caused by a blockage in the blood flow through the liver. Massive Blood Transfusions Occurs when a patient has been transfused continuously with fresh whole blood
In a whole blood transfusion there are plasma which may dilute the platelets of the patient decrease platelet count
That’s why physicians usually give a packed RBC to the patient
THROMBOCYTOSIS (Increased Platelet Count) GROUPS EXAMPLES OF ASSOCIATED CASES A.) Reactive Thrombocytosis
aka: SECONDARY THROMBOCYTOSIS
characterized by: Moderate increased platelet count
Recovery from splenectomy pupunta sa circulation yung plt.
Acute blood loss
Major surgery B.) Autonomous Thrombocytosis
aka: PRIMARY THROMBOCYTOSIS
Essential Thrombocytemia (ET)
Polycythemia Vera (PV)
characterized by: Markedly increased platelet count Chronic Myelogenous Leukemia (CML)
Primary Myelofibrosis (PMF)
B. QUALITATIVE
Examples of conditions with: PLATELET ADHESION DISORDER When platelets adhere in foreign surface Bernard Soulier Syndrome (BSS)
Deficiency of the GP Ib/IX/V (a receptor for vwF which is important for plt adhesion to occur)
Inherited as AUTOSOMAL RECESSIVE (AR)
Associated with ↓PLATELET count (impaired platelet production in BM)
Giant platelets Normal aggregation ADP, Collagen, Epinephrine Abnormal aggregation Ristocetin . Von Willebrand Disease (vWD)
Deficiency of the vWF
Inherited as AUTOSOMAL DOMINANT (AD)
Associated with Dec. factor VIII (Vwf is carrier protein of factor VIII)
HemaTOLOGY II
Normal PT, Prolonged APTT
Normal aggregation ADP, Collagen, Epinephrine Abnormal aggregation Ristocetin . . Examples of conditions with: PLATELET AGGREGATION DISORDER When platelets adhere to other platelets
Glanzmann’s thrombasthenia
Deficiency of GP IIb/IIIa
Characterized by: Very prolonged bleeding time
Abnormal clot retraction Normal aggregation Ristocetin Abnormal aggregation ADP, Collagen, Epinephrine . Hereditary afibrinogenemia
Absence of fibrinogen in blood
. Examples of conditions with: PLATELET SECRETION DISORDER
Thromboxane pathway disorders
Cyclooxygenase or thromboxane synthetase deficiency
Storage pool diseases
ALPHA GRANULE
DEFICIENCY
Gray platelet syndrome
Autosomal Recessive disorder
Characterized with: Mild bleeding tendency Thrombosis of BM Thrombocytopenia Large platelets
DENSE GRANULE
DEFICIENCIES
Hermansky-Pudlak syndrome
Chediak-Higashi syndrome
TAR syndrome
Wiskott-Aldrich syndrome (SMALL platelets) .