


Shoulder girdle
Normal X-ray of the shoulder girdle
Normal X-ray of the shoulder girdle






Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
A comprehensive overview of common fractures affecting the shoulder girdle, humerus, forearm, and hand. It details the anatomy, mechanisms of injury, and management strategies for each fracture type. Illustrative x-ray images and explanations of the key neurovascular structures at risk for each fracture. It is a valuable resource for students and professionals in the fields of medicine, anatomy, and orthopedics.
Typology: Schemes and Mind Maps
1 / 10

This page cannot be seen from the preview
Don't miss anything!
The clavicle acts to transmit forces from the upper limb to the axial skeleton. Given its relative size, this leaves it particularly susceptible to fracture. The most common mechanism of injury is a fall onto the shoulder or onto an outstretched hand. With the clavicle arbitrarily divided into thirds: ● 15% of fractures occur in the lateral third ● 80% occur in the middle third ● 5% occur in the medial third. After a fracture, the lateral end of the clavicle is displaced inferiorly by the weight of the arm and displaced medially by the pectoralis major. The medial end is pulled superiorly by the sternocleidomastoid muscle. Management of a clavicular fracture can be conservative (e.g. sling immobilization) or operative (e.g. open reduction and internal fixation). The supraclavicular nerves lie in close proximity to the clavicle and are occasionally sacrificed during a surgical repair – resulting in a numb patch over the upper chest and shoulder. X-Ray of a clavicular fracture.
X-ray left shoulder (AP view) fracture of the proximal humerus at the level of the surgical neck (red arrow), and the fracture is overriding by > 1cm. The greater tuberosity is also fractured but not significantly displaced, and the posterior part of the humeral head is angulated towards the midline of the body.
Proximal humerus fracture There is a humerus fracture at the anatomical neck (red overlay), with a slightly medially displaced fragment. However, the head of the humerus still articulates with the glenoid fossa. Additionally, a nondisplaced fracture of the greater tubercle (green overlay) can be seen. A mid-shaft fracture of the humerus risk damage to the radial nerve and profunda brachii artery (as they are tightly bound in the radial groove).
Normal X-ray of forarm bones The forearm is a common site for bone fractures. A fracture of the ulna alone (not involving the radius) usually occurs as a result of the ulna being hit by an object. The shaft is the most likely site of fracture. In this situation, the normal muscle tone will pull the proximal ulna posteriorly. Less commonly, the olecranon process can be fractured. This is caused by the patient falling on a flexed elbow. The triceps brachii can displace part of the fragment proximally. Ulnar fracture
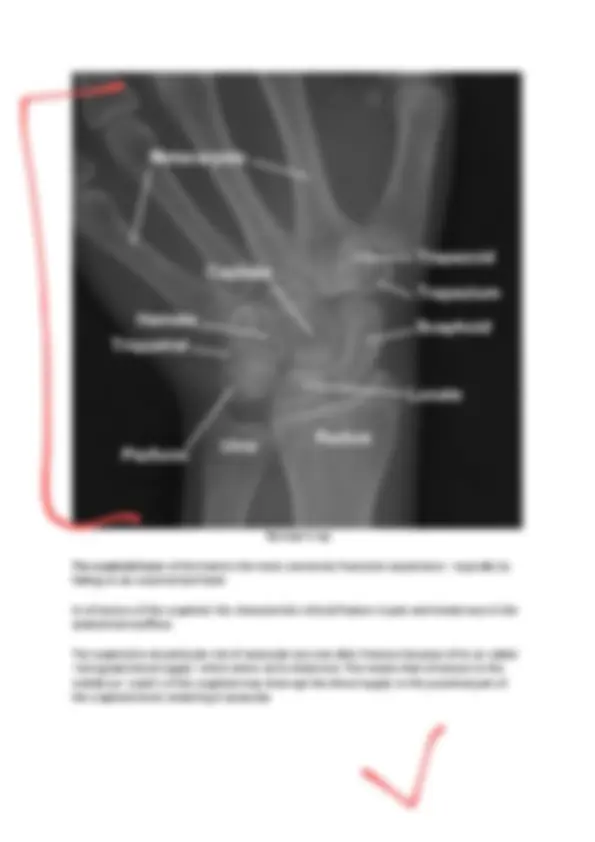
Normal X-ray The scaphoid bone of the hand is the most commonly fractured carpal bone – typically by falling on an outstretched hand In a fracture of the scaphoid, the characteristic clinical feature is pain and tenderness in the anatomical snuffbox. The scaphoid is at particular risk of avascular necrosis after fracture because of its so-called ‘retrograde blood supply’ which enters at its distal end. This means that a fracture to the middle (or ‘waist’) of the scaphoid may interrupt the blood supply to the proximal part of the scaphoid bone rendering it avascular.
There are two common fractures of the metacarpals : Boxer’s fracture – A fracture of the 5th metacarpal neck. It is usually caused by a clenched fist striking a hard object. The distal part of the fracture is displaced anteriorly, producing shortening of the affected finger. Bennett’s fracture – A fracture of the 1st metacarpal base, caused by forced hyperabduction of the thumb. Bennett’s fracture. Boxer’s fracture