Download Forearm Fractures and more Study notes Anatomy in PDF only on Docsity!
Forearm Fractures
Sean T. Campbell, MD
Assistant Attending
Orthopedic Trauma Service
Hospital for Special Surgery, New York, NY
Objectives
- Understand rationale for surgery for forearm fractures
- Understand which segment is unstable based on injury pattern
- Identify goals of surgery based on injury pattern
- Review surgical techniques
C ore C urriculum V
Anatomy
- Two bones that function as a forearm joint to allow rotation
- Radius
- Radial bow in coronal plane
- Ulna
- Proximal dorsal angulation in sagittal plane
- Not a straight bone
- Distinct bow in coronal plane (see next slides)
- Proximal radioulnar joint (PRUJ)
- Articulation of radial head with proximal ulna
- Distal radioulnar joint
- Articulation of ulnar head with distal radius
- Interosseous membrane Hreha J+, Snow B+ Image from: Jarvie, Geoff C. MD, MHSc, FRCSC; Kilb, Brett MD, MSc, BS,†; Willing, Ryan PhD, BEng‡; King, Graham J. MD, MSc, FRCSC‡; Daneshvar, Parham MD, BS* Apparent Proximal Ulna Dorsal Angulation Variation Due to Ulnar Rotation, Journal of Orthopaedic Trauma: April 2019 - Volume 33 - Issue 4 - p e120-e123 doi: 10.1097/BOT.
Anatomy
- Radial bow allows for pronosupination
- Must be restored surgically when compromised
- Multiple methods for assessment of radial bow
- Comparison to contralateral images
- Direct anatomic reduction of simple fractures
- Biceps tuberosity 180 degrees of radial styloid
- Note opposite apex medial bow of ulna
Image from: Rockwood and Green, 9e, fig 41-
Initial Presentation
- Antibiotics for open fractures
- Careful attention to neurovascular status
- Physical and radiographic exam of wrist and elbow joints
- Temporizing splint immobilization above the elbow
- High risk for compartment syndrome - Especially high energy mechanisms - Be familiar with technique for forearm compartment release: OTA video library
Surgical Indications
- Most fractures are operative in adults
- Both bone fractures- inherently unstable
- Loss of radial bow interferes with pronosupination
- Single bone diaphyseal injuries
- Often result in
- PRUJ instability (Monteggia)
- DRUJ instability (Galeazzi)
- Exceptions
- Some nondisplaced single bone injuries (i.e. nightstick fracture of ulna)
- Outcomes
- In general good
- Moderate decrease in perceived strength*
Surgical Goals for All Forearm Fractures
- Restoration of forearm anatomy
- Length/alignment/rotation (L/A/R) + correct bow
- Stable and congruent elbow and wrist joints
- Address fracture of sigmoid notch or radial head
- Robust fixation to allow early motion
- Avoid thin/tubular plates
- Intelligent fixation based on fracture pattern
- Simple patterns- anatomic reduction and compression
- Comminuted patterns- restoration of L/A/R/bow with bridge
plating
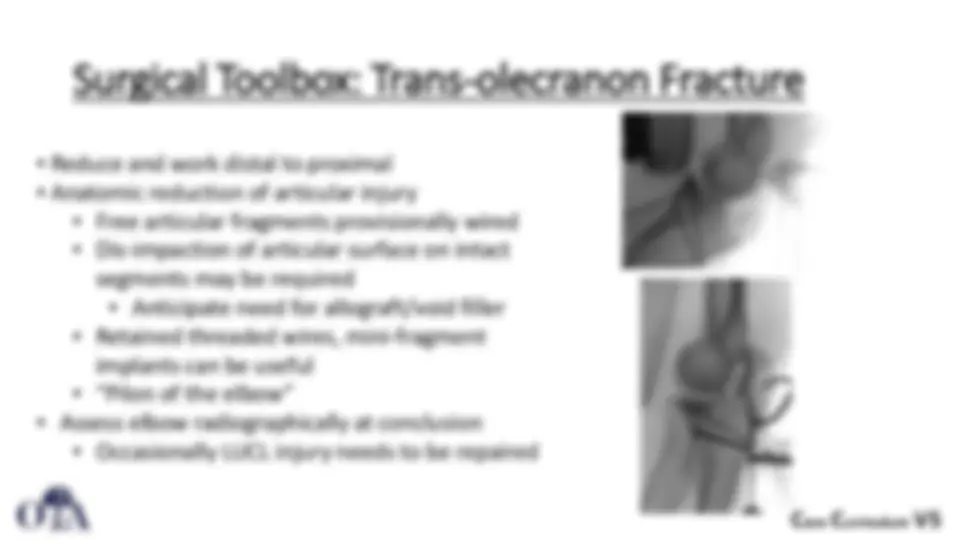
Surgical Toolbox: Diaphyseal Both Bone
Positioning
- Supine, radiolucent hand table
- Preferred: Most diaphyseal and distal fractures
- Disadvantage: must flex (and hold flexed) elbow to approach ulna
- Addressing radius first typically easier in this position
- Gives stability to forearm for treatment of ulna in the elbow-flexed position
- Lateral with elbow flexed 90 degrees
- Advantage: Complex proximal ulna fracture; transolecranon fracture-dislocation
- Disadvantage: unfamiliar positioning for radius- may require repositioning
- Indications:
- Difficult/segmental proximal ulna fracture
- Ipsilateral humerus fracture to be addressed with same anesthetic
Surgical Toolbox: Diaphyseal Both Bone
Clinical photos demonstrating the volar approach to the radius.
Middle: Elevator is pointing at the superficial branch of the radial nerve.
Right: The fracture has been exposed (elevator at fracture line). The white structure just ulnar to the elevator is the pronator teres tendon. White arrow points to radial artery.
Surgical Toolbox: Diaphyseal Both Bone
Ulnar Exposure
- ECU/FCU split
- Be aware of ulnar bow
- Ulna is not truly “subcutaneous” throughout full length
- ECU/FCU interval may “cross” over border of the bone
- Utilize correct interval to preserve muscle as possible
- Extensile proximally into posterior approach to humerus
- OTA video library example
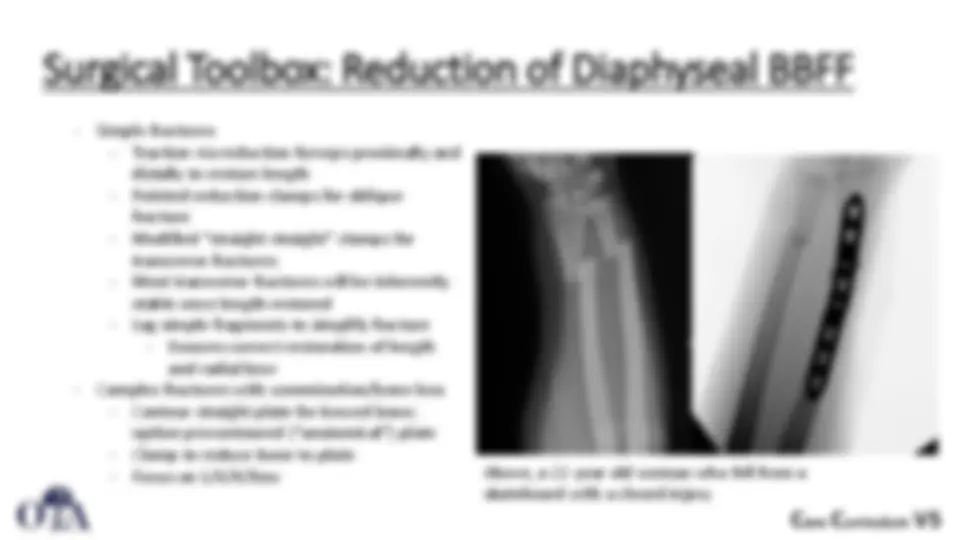
Surgical toolbox: Fixation of Diaphyseal BBFF
- Simple fractures
- Lag screw/neutralization plating for obliquity fracture
- Countersink volar 2.4mm lag screws if under plate
- Dynamic compression plating for transverse fracture
- Mini-fragment plate can be used for provisional reduction
- Plate selection
- 3.5mm LCDCP or similar on radius and ulna
- 2.7 DCP in smaller patients on ulna
- Avoid tubular or flexible plates
- Slight prebend needed if compression plating
- Comminuted/Segmental bone loss fractures
- Long contoured plates with well balanced screw spread preferred
- Full length films (flat plates) can be useful for assessing radial bow - Consider comparison views of contralateral side
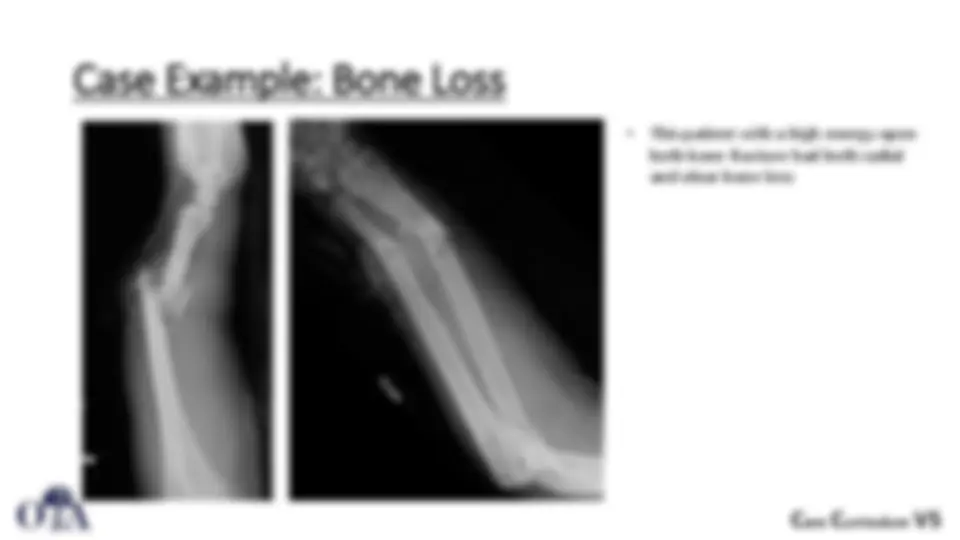
Case Example: Both Bone Forearm Fracture
- Bridge plating due to comminution
- Eccentric straight plate highlights restored radial bow
C ore C urriculum V
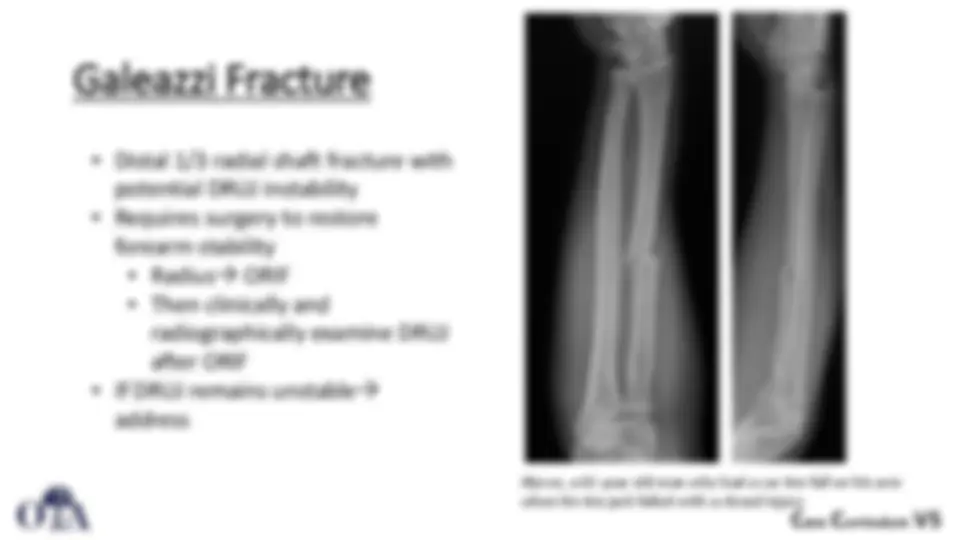
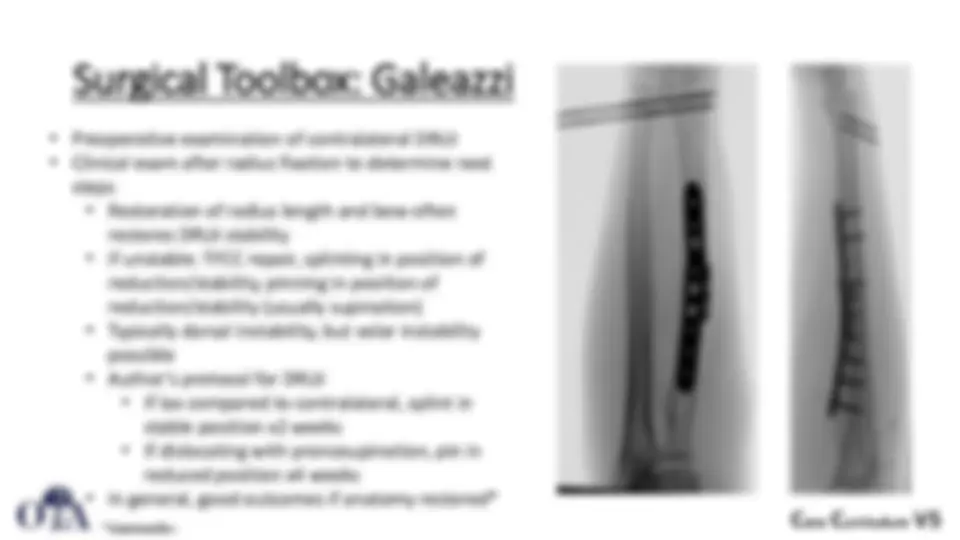
Surgical Toolbox: Galeazzi
- Preoperative examination of contralateral DRUJ
- Clinical exam after radius fixation to determine next
steps
- Restoration of radius length and bow often
restores DRUJ stability
- if unstable: TFCC repair, splinting in position of
reduction/stability, pinning in position of
reduction/stability (usually supination)
- Typically dorsal instability, but volar instability
possible
- Author’s protocol for DRUJ
- If lax compared to contralateral, splint in
stable position x2 weeks
- If dislocating with pronosupination, pin in
reduced position x4 weeks
- In general, good outcomes if anatomy restored* *Giannoulis+
C ore C urriculum V
Monteggia Fracture
- Ulna shaft fracture with radial head dislocation (PRUJ
instability)
- Classification system based on direction of
dislocation (next slide - diagram of classification)
- Associated injuries:
- LUCL injury, radial head fracture, coronoid
fracture
- Outcomes
- In general, good
- Poorer with Bado type II fractures (see next
slide), associated radial head and coronoid
fractures*
*Sreekumar+