



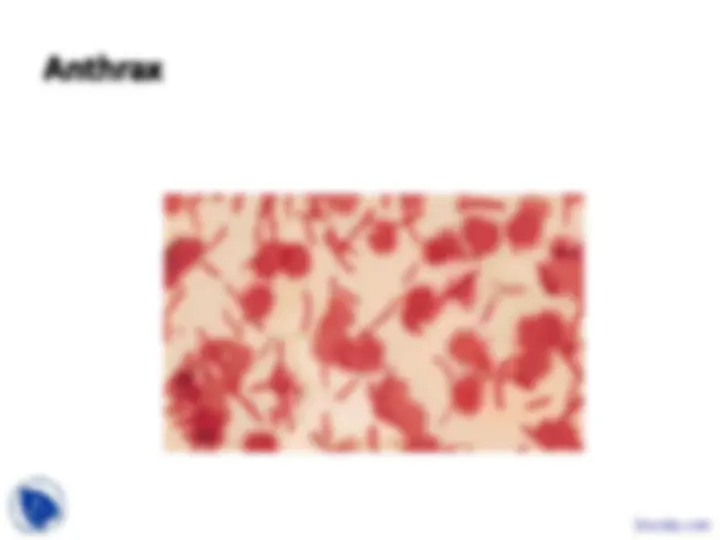
ANTHRAX
Docsity.com




Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
Comprehensive information on anthrax, a zoonotic and agricultural disease caused by bacillus anthracis. It covers the etiology, transmission, forms of the disease, diagnosis, and treatment of anthrax, including cutaneous, gastrointestinal, and inhalational forms. The document also discusses the severity and fatality rates of each form, as well as the diagnostic methods and therapies for anthrax.
Typology: Slides
1 / 18

This page cannot be seen from the preview
Don't miss anything!
244 cases/US 1944-
Cutaneous Gastrointestinal-
oropharyngeal/abdominal Inhalational
hemorrhage, edema, necrosis
Pediatric Guidelines