


Assoc. Prof. Iv. Lambev
www.medpharm-sofia.eu
Medical University of Sofia, Faculty of Medicine
Department of Pharmacology and Toxicology
•Antidepressants
•Mood stabilizers
•Psychostimulants
•Nootropic drugs
•CNS stimulants
(Abstract)











Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
Pharmacy lecture note for student
Typology: Lecture notes
1 / 58

This page cannot be seen from the preview
Don't miss anything!
Assoc. Prof. Iv. Lambev
www.medpharm-sofia.eu
Antidepressants
Mood stabilizers
Psychostimulants
Nootropic drugs
CNS stimulants
(Abstract)
(1) brief reactive or secondary depression (most common),
occurring in response to real stimuli such as grief, illness , etc;
(2) major depression (melancholic and recurrent depression)
a genetically determined biochemical disorder manifested
by an inability to experience ordinary pleasure or to cope with
ordinary life events;
(3) manic-depressive depression (depression associated with
bipolar affective disorder )
Pharmacologic treatment of depressions is very important, although
a continuing role for electroconvulsive therapy for severe forms of
life-threatening depression is also noted.
Depression is one of the most common psychiatric disorders.
At any given moment, about 3–5% of the population is depressed,
and an estimated 10% of people may become depressed during
their lives. The symptoms of depression are often subtle and
unrecognized both by patients and by physicians. Patients with
vague complaints that resist explanation as manifestations of
somatic disorders and those who might be simplistically described
as “neurotic” should be suspected of being depressed.
Soon after the introduction of reserpine (1948), it became
apparent that the drug could induce depression by inhibiting the
neuronal storage of amine neurotransmitters 5-HT and NE.
Reserpine-induced depression and depleted stores of amine neuro-
transmitters. It was reasoned, depression must be associated
with decreased functional amine-dependent synaptic transmission.
Rauwolfia serpentina
(a small indian shrub)
Reserpine
Ajmaline
Pathogenesis of depression
The idea that depression must be associated with decreased
functional amine-dependent synaptic transmission
By extension, drugs that increased amine function in appropriate
synaptic areas would relieve depression.
The amine hypothesis has provided the major experimental
models for the discovery of new antidepressants.
All currently available antidepressants, except bupropion,
are classified as having their primary actions on the
metabolism, reuptake, or selective receptor antagonism
of 5-HT, NA, or both.
(CREB) protein which in turn is involved in
n eurotrophic f actor ( BDNF ) which exerts effects on
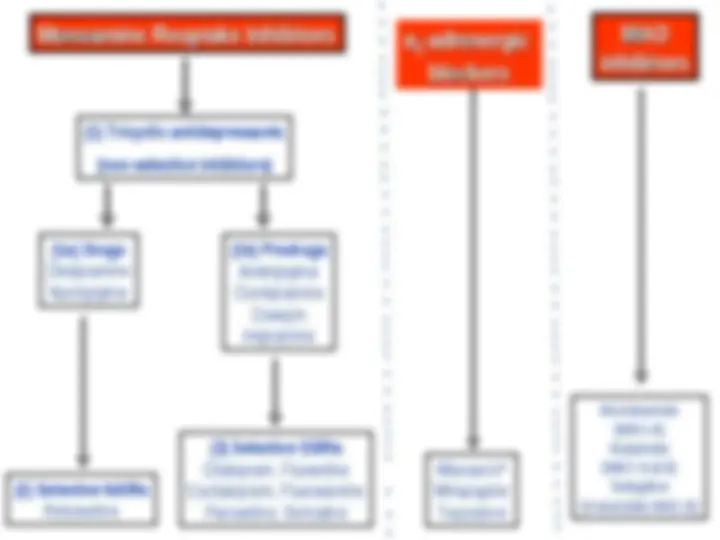
Monoamine Reuptake Inhibitors
Monoamine Reuptake Inhibitors
α
α
22
-adrenergic
-adrenergic
blockers
blockers
MAO
MAO
inhibitors
inhibitors
(1a) Drugs
Desipramine
Nortriptyline
(1b) Prodrugs
Amitriptyline
Clomipramine
Doxepin
Imipramine
(2) Selective NARIs
Reboxetine
(3) Selective SSRIs
Citalopram, Fluoxetine
Escitalopram, Fluvoxamine
Paroxetine, Sertraline
Mianserin*
Mirtazapine
Trazodone
(1) Tricyclic antidepressants
(non-selective inhibitors)
Moclobemide
(MAO-A)
Nialamide
(MAO-A & B)
Selegiline
(irreversible MAO-B)
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - Structural relationships between
various tricyclic antidepressants (TCAs).
Their structures are similar to phenothiazines.
Pharmacokinetics
The antidepressants are generally well absorbed
after oral administration. Steady-state plasma
concentrations of TCAs show great individual
variation but correlate with therapeutic effect.
Antidepressants in general are inactivated princi-
pally by metabolism by hepatic cytochrome P
enzymes (2D6 and 3A4). Other cytochrome
enzymes are CYP 1A2 inhibited by the SSRI
fluvoxamine, and induced by cigarette smoking,
caffeine and the atypical antipsychotics (clozapine
and olanzapine).
Several of these drugs produce active metabolites
which prolong their action (e.g. fluoxetine is
metabolized to norfluoxetine, t
1/
200 h). The meta-
bolic products of certain TCAs are antidepressants
too, e.g. nortriptyline (from amitriptyline),
desipramine (from imipramine).
Half-lives of TCAs and SSRIs are long (> 15 h).
Around 7% of the Caucasian population have
very limited CYP 2D6 enzyme activity.
Such “poor metabolizers” may find standard
doses of tricyclic antidepressants intolerable and
it is often worth starting at a very low dose.
(fluoxetine – in higher doses)
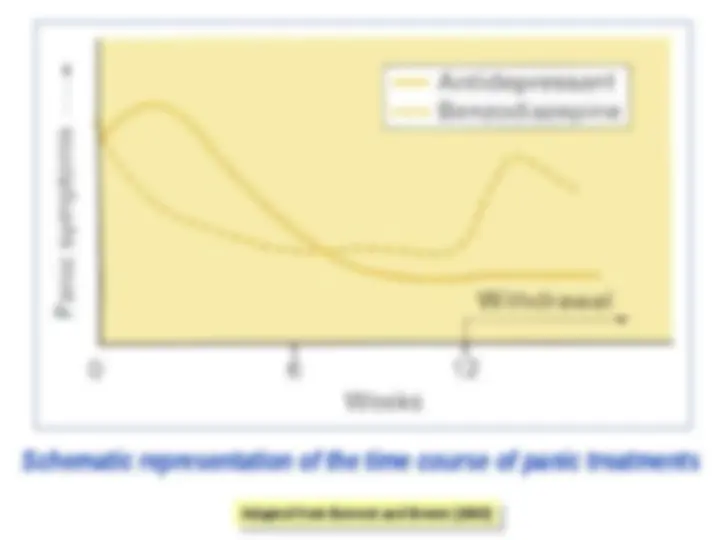
Schematic representation of the time course of panic treatments
Adapted from Bennett and Brown (2003)
Adapted from Bennett and Brown (2003)