Download Applied Biostatistics, Lecture Notes - Mathematics - 31 and more Study notes Mathematical Methods in PDF only on Docsity!
University of York
Department of Health Sciences M.Sc. programme
Reporting statistical analyses
Structure of a statistical report
Reports are much easier to read if they have structure, with headings and subheadings. One way of structuring a report of a statistical analysis is to make it follow the plan of a scientific paper:
- Introduction
- Methods
- Results
- Discussion
- Conclusions
It gives the statistical parts of these:
- Introduction: the questions to be answered and the data available.
- Methods: the statistical methods to be used and why they have been chosen.
- Results: what has been found.
- Discussion: any limitation of these analyses.
- Conclusions: what we can conclude from these analyses.
This is the method which I would recommend and which I use myself. Other methods are possible.
What should go into the report? Look at published research papers. They do not contain lots of computer printout. They contain the results of the analysis, extracted from the computer printout.
What analysis to do when
There are two main types of variable: continuous measurements and categorical classifications. The first thing to do in deciding on the analysis is to decide what kind of variable we have as the outcome variable, the one which we are trying to explain or investigate.
The next question is what kind of analysis are we going to do. This might be:
- descriptive analysis for a single variable,
- estimate for a single group,
- changes in a single group or in matched pairs,
- comparison of two independent groups,
- relationship between two or more variables.
The appropriate analysis can then be decided as in the following table:
Analysis Continuous Categorical Descriptive Histogram, mean, standard deviation, median, range
Frequencies and percentages Single group Confidence interval for mean
Confidence interval for proportion Changes in one group Paired t method, large sample Normal method, sign test, signed rank test
McNemar’s test*
Compare two groups Two sample t method, large sample Normal method
Chi-squared test, odds ratio or relative risk
Relationship between two variables
Scatter diagram, correlation coefficient, linear regression
Cross-tabulation, chi- squared test
- not included in this course.
An example
The data file contains data from a case control study of stroke, a group of stroke patients and a group of unmatched controls. It contains the following variables:
case Case control status case=1, control= age Age in years sex Sex female=1 male= chol Serum cholesterol in mmol/L evsmok Ever smoked no=1 yes=
Questions about these data
- Is there anything to suggest that cases and controls were not comparable in terms of age and sex?
- Do cases differ in cholesterol or smoking history?
- Could age or sex differences have any affect on the relationships between stroke and cholesterol or smoking history?
Introduction
The data consist of five variables measured on a group of stroke patients and controls who have not had strokes. First the data will be described and any errors checked for. The age and sex distributions of cases and controls will be compares. The mean cholesterol levels and the smoking history will be compared between cases and controls. We then consider possible effects of age or sex differences between cases and controls on any cholesterol and smoking differences found.
Methods
The distributions of the continuous variables, age and serum cholesterol, will be examined using histograms. The distributions of the categorical variable, case control status, sex, and smoking history, will be examined by tabulation. Any observations which appear to be mistakes will be identified and we will decide what to do about them. The mean age will be compared between the groups using a large sample Normal comparison of means, because this is a continuous variable and there are more than 100 observations in each group. The sex
40.00 50.00 60.00 70.00 80.00 90.
Age (years)
0
10
20
30
40
Frequency
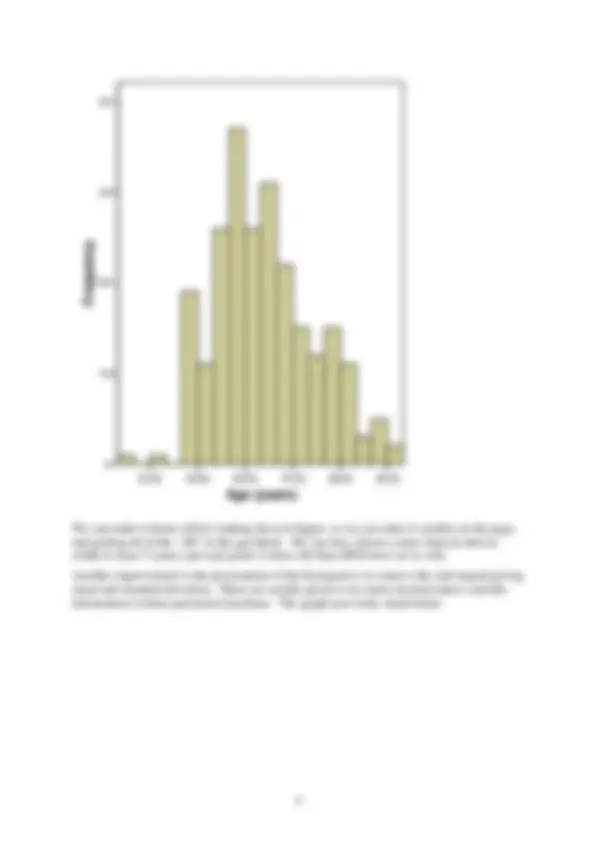
We can make it better still by making the text bigger, so we can make it smaller on the page, and getting rid of the “.00” in the age labels. We can also choose a more logical interval width (I chose 5 years) and start point (I chose 20) than SPSS does on its own.
Another improvement to the presentation of the histogram is to remove the side legend giving mean and standard deviation. These are usually given to too many decimal places and this information is better presented elsewhere. The graph now looks much better.
Age (years)
Frequency
The distribution has a positively skew shape with mean age 64.3 years and standard deviation 10.5 years. (Note that age is recorded in whole years, so we do need more than one decimal place for mean and standard deviation. Just because the computer prints them out, you do not have to use them. It is a good idea to give units when you quote means and standard deviations.)
We do the same for cholesterol:
Serum cholesterol (mmol/L)
Frequency
For the report, it is better to remove the mean and standard deviation from the graph and give them in the text instead: “Serum cholesterol has a positively skew distribution with mean 5. mmol/L and standard deviation 1.3 mmol/L.” There are serum cholesterol measurements for only 169 of the 238 subjects, so there are quite a high proportion of observations missing, 69/238 = 29%. We should mention this as it will be an important limitation which we should mention in the discussion.
The tables for the three categorical variables produces the following SPSS output:
Frequencies
Statistics
case evsmok sex N Valid (^238 238 ) Missing (^0 0 )
Frequency Table
case
Frequency Percent Valid Percent
Cumulative Percent 1.00 (^101) 42.4 42.4 42. 2.00 (^137) 57.6 57.6 100.
Valid
Total (^238) 100.0 100.
evsmok
Frequency Percent Valid Percent
Cumulative Percent .00 (^1) .4 .4. 1.00 (^130) 54.6 54.6 55. 2.00 (^107) 45.0 45.0 100.
Valid
Total (^238) 100.0 100.
sex
Frequency Percent Valid Percent
Cumulative Percent 1.00 (^110) 46.2 46.2 46. 2.00 (^128) 53.8 53.8 100.
Valid
Total (^238) 100.0 100.
You do not see this sort of thing in published papers. We need only the frequencies and the percentages and we should label the categories. We could do this either in SPSS using values in the variables view, or in the word processed report. We could give something like this:
There were no missing values for case control status, sex or smoking history. The proportions in each category were:
Case control status Frequency Case 101 (42.4%) Control 137 (57.6%)
Sex Frequency Female 110 (46.2%) Male 128 (53.8%)
Smoking history Frequency 0 1 (0.4%) Never smoked 130 (54.6%) Has smoked 107 (45.0%)
You could improve the report by having table numbers and legends for these tables and refer to them in the text as you would in a paper, e.g. “Table 2 shows the numbers of male and female subjects.”
Table 2. Numbers of male and female subjects Sex Frequency Female 110 (46.2%) Male 128 (53.8%)
I haven’t done this in these notes for reasons of time and space.
Smoking history has one impossible code, which we shall set to missing:
Table: Age (years) of cases and controls
Group Number Mean Std. Deviation Cases 100 64.9 9. Controls 137 63.9 11.
Because we are using the large sample Normal test, we need the comparison of means when equal variances are not assumed. We can say the difference in mean age (cases minus controls) is 1.0 years (SE=1.3, 95% confidence interval –1.6 to 3.7 years, P=0.4). Hence there is no evidence that the groups differ in mean age. The standard deviation is larger in the control group and the Levene test shows that this is significant (P=0.008), so the controls vary more in age than do the cases.
For sex, we cross-tabulate case control status by sex. As is conventional, I have put case control status as the row variable. I have also asked for row percentages in the cells, because this gives me the percentage of cases who are female. The percentage of females who are cases would be meaningless.
Crosstabs
Case Processing Summary
Cases Valid Missing Total N Percent N Percent N Percent case * sex (^238) 100.0% 0 .0% 238 100.0%
case * sex Crosstabulation
sex 1.00 2.00 Total 1.00 Count (^32 69 ) % within case 31.7%^ 68.3%^ 100.0% Count (^78 59 )
case
% within case 56.9%^ 43.1%^ 100.0% Total Count (^110 128 ) % within case 46.2%^ 53.8%^ 100.0%
Chi-Square Tests
Value df
Asymp. Sig. (2-sided)
Exact Sig. (2-sided)
Exact Sig. (1-sided) Pearson Chi-Square (^) 14.913(b) 1. Continuity Correction(a) 13.915^1. Likelihood Ratio (^) 15.156 1. Fisher's Exact Test (^) .000. Linear-by-Linear Association 14.851^1. N of Valid Cases (^238) a Computed only for a 2x2 table b 0 cells (.0%) have expected count less than 5. The minimum expected count is 46.68.
As before, we do not want this chunk of printout in the report. We could use a version of the cross-tabulation
Patient group Sex Female Male
Total
Cases 32 (31.7%) 69 (68.3%) 101 (100%) Controls 78 (56.9%) 59 (43.1%) 137 (100%)
Note that I have omitted the column totals, because in this case control study they do not mean anything. Cases and controls were sampled as two separate groups and there is a far greater proportion of cases in this sample than there would be in a general sample from the adult population. The same would be true in a clinical trial.
We can quote a test of the null hypothesis that these variables are independent. This is a large sample and all the expected frequencies are greater than 5 (check if you like, but SPSS tells you that the minimum is 46.68) and so we can use the chi-squared test, labelled “Pearson Chi-square” by SPSS: chi-squared = 14.91, df = 1, P < 0.001. Do not quote P = 0.000 as shown in the SPSS output. This is a technically correct representation of the probability to 3 decimal places, but because P cannot be actually equal to zero the convention is to emphasise this by putting P<0.001. Ignore all the other tests. Never quote something when you don’t know what it means and didn’t want it. SPSS often gives you more than you ask for.
We could also give an odds ratio for the table, this being a case control study. SPSS has this labelled “Risk” in Crosstabs:
Risk Estimate
95% Confidence Interval Value (^) Lower Upper Odds Ratio for case (1.00 / 2.00) .351^ .205^. For cohort sex = 1.00 (^) .556 .404. For cohort sex = 2.00 (^) 1.586 1.255 2. N of Valid Cases (^238)
The first row gives the odds ratio. As we don’t know what the second and third rows mean, we should ignore them. The odds ratio for being female given stroke is 0.35 (95% CI 0.21 to 0.60). As this is a case control study and stroke is a rare condition in the population we can use this as an estimate of the relative risk of stroke for women compared to men: 0.35 (95% CI 0.21 to 0.60).
Hence we have a big difference in sex between cases and controls but not in mean age.
Comparison of cholesterol and smoking history between cases and controls
We do analyses very similar to those for age and sex, so I won’t go through them in detail. We get:
Serum cholesterol (mmol/L) Number Mean Standard deviation Cases 85 6.33 1. Controls 84 5.53 0.
Sex Patient group Smoking history Never smoked
Has smoked
Total Chi-squared test with 1 d.f. Females Cases 9 (28.1%) 23 (71.9%) 32 (100%) Controls 59 (76.6%) 18 (23.4%) 77 (100%)
P < 0.
Males Cases 21 (30.4%) 48 (69.6%) 69 (100%) Controls 41 (69.5%) 18 (30.5%) 59 (100%)
P < 0.
Hence for men and for women separately there is a highly significant association between stroke and smoking. (In practice, we would not analyse the females and males separately, but would use a method called logistic regression, outside the scope of this course. This gives the relative risk of stroke for smokers, adjusted for sex, RR = 6.32, P < 0.001.)
Discussion
We have found clear associations between stroke and higher serum cholesterol, and between stroke and having smoked. Neither of these can be explained by differences in age or sex distribution between cases and controls.
Quite a lot of the serum cholesterol measurements are missing, and we would like to know why this is. Is there any systematic difference in what led them to be missing between the two groups? Such differences might produce spurious relationships. Also, we have a small number of missing observations for other variables in the analysis, which weakens it a little.
We cannot conclude from these data that high cholesterol causes stroke. It may be that having a stroke increases cholesterol, or that some factor that increase the risk of stroke also increases serum cholesterol. It is implausible that history of smoking is a result of stroke, but it is possible that some other factor both increases the risk of stroke and the risk of smoking. We would have to use other knowledge to shed light on these possibilities, which is beyond the scope of this report. We can say from the analysis neither sex nor age is a third variable which produces a non-causal relationship between stroke and either cholesterol or sex.
Conclusions
Stroke is associated with raised serum cholesterol and with a history of cigarette smoking. The mean serum cholesterol is estimated to be between 0.43 and 1.16 mmol/L higher in stroke patients, the risk of stroke for those with a history of smoking is between 3.7 and 11. times the risk for those who have never smoked. These associations do not appear to be explained by age or sex differences between stroke cases and people who have not had strokes.
Key points in writing statistical reports
- Do not put in chunks of unmodified SPSS output.
- Do not put in analyses you do not want or do not understand.
- Watch out for impossible values. Do not leave them in the analysis.
- Always be aware that there may be more than one explanation for a relationship.
Martin Bland 13 December 2005