Download CHAPTER-4_RESPIRATORY SYSTEM and more Summaries Medicine in PDF only on Docsity!
CHAPTER 4: RESPIRATORY SYSTEM
🔹 I. Anatomy Overview
A. Upper Respiratory Tract
Nasal cavity, pharynx, larynx. Filters, warms, and humidifies inspired air. Common site for infections and obstruction.
B. Lower Respiratory Tract
Trachea → bronchi → bronchioles → alveoli. Right lung: 3 lobes, Left lung: 2 lobes. Alveoli: site of gas exchange; surrounded by pulmonary capillaries. Pleura: double membrane — visceral (covers lung), parietal (lines chest wall). Pleural space contains small amount of fluid for friction-free movement.
C. Radiographic Landmarks
Carina: at T4 – T5 level, bifurcation of trachea. Right main bronchus more vertical → foreign body aspiration more common. Diaphragm: right higher than left (due to liver).
🔹 II. Chest Radiography — Projections and Use
Projection Purpose / Findings PA Chest Standard view: shows lungs, heart, mediastinum; best for detecting air-space disease, effusions. Lateral Chest Confirms location of lesions, retrosternal or posterior effusion. AP Supine / Portable For patients who can’t stand; heart appears magnified. Lordotic View Evaluates lung apices for TB or masses. Decubitus Detects small pleural effusions or pneumothorax (air-fluid level shift). Expiration View For small pneumothoraces (air more visible as lung volume decreases).
🔹 IV. Classification of Respiratory Diseases
1. Congenital / Hereditary 2. Inflammatory / Infectious 3. Neoplastic 4. Traumatic 5. Occupational / Environmental
- Pleural Diseases 🔹 V. Major Pathologies
🧬 1. Congenital & Hereditary Disorders
Disorder Description Imaging Findings Cystic Fibrosis (CF) Autosomal recessive disease; affects exocrine glands → thick mucus obstructs bronchi. Hyperinflation, bronchial thickening, mucus plugging, recurrent pneumonia. Hyaline Membrane Disease (RDS) Seen in premature infants (lack of surfactant). Ground-glass lungs with air bronchograms.
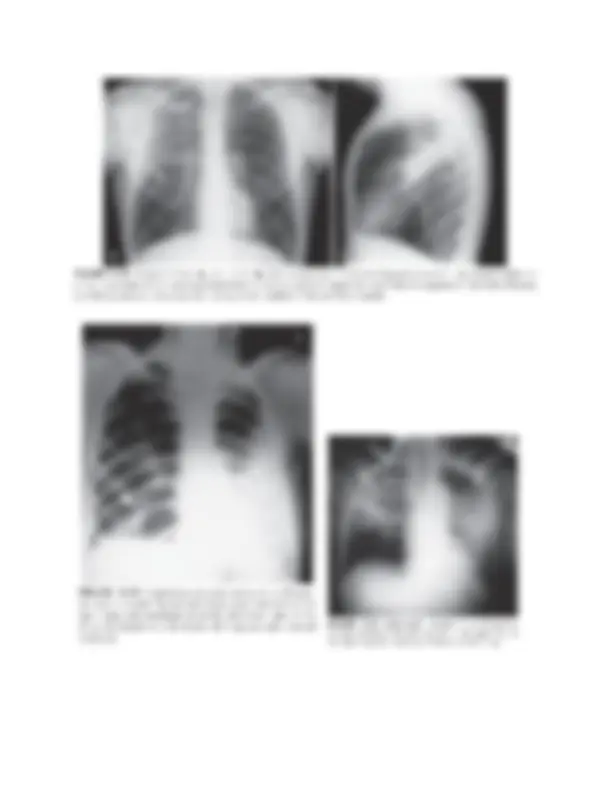
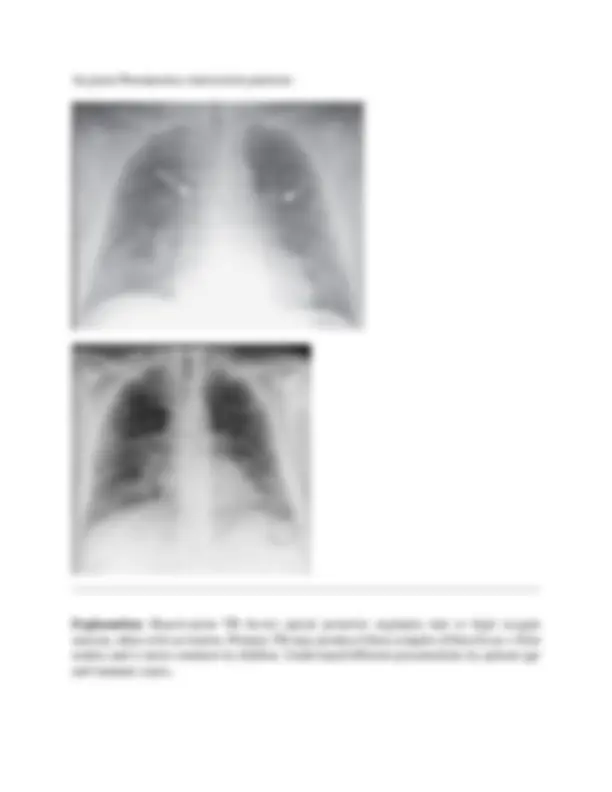
Cystic Fibrosis (CF)
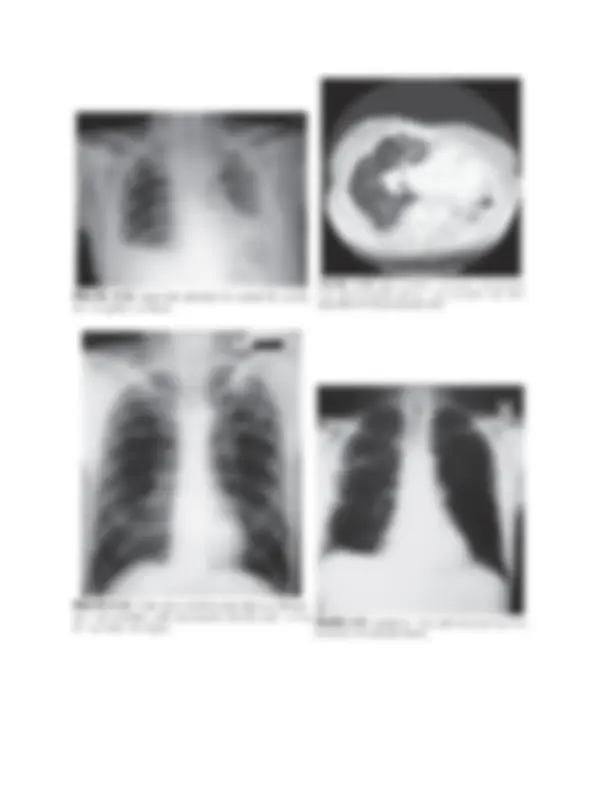
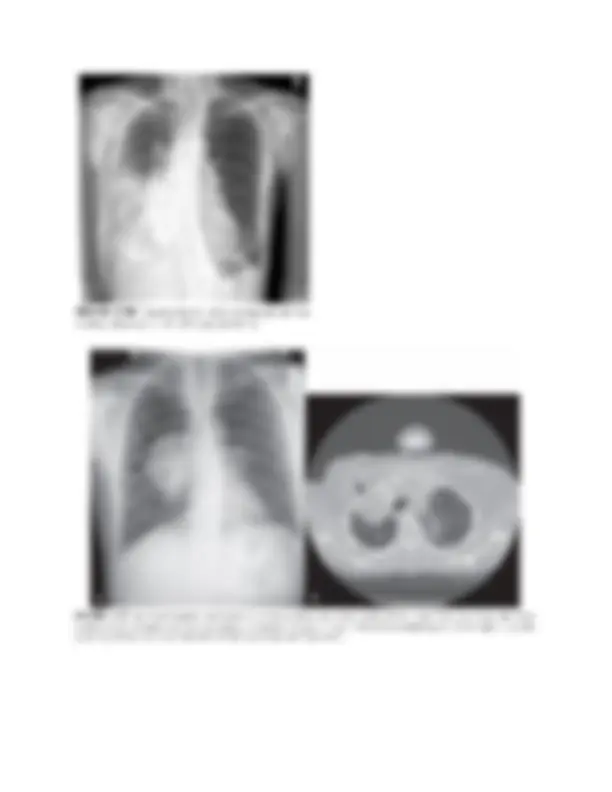
Disorder Cause / Mechanism Radiographic Appearance Pneumonia Infection → alveolar inflammation and consolidation. Patchy or lobar opacity, air bronchograms, loss of lung markings. Aspiration Pneumonia Inhalation of gastric contents → chemical inflammation. Segmental opacities, especially posterior segments of upper lobes or superior lower lobes. Bronchiectasis Chronic dilation of bronchi from infection. “Tram-track” lines or cystic spaces. Lung Abscess Localized pus collection from necrotic pneumonia. Round cavity with air–fluid level. Tuberculosis (TB) Mycobacterium tuberculosis. Primary: hilar/mediastinal lymphadenopathy; Secondary: apical cavitations, fibrosis. Chronic Obstructive Pulmonary Disease (COPD) Emphysema + chronic bronchitis; air trapping. Hyperinflated lungs, flattened diaphragm, elongated heart, ↓ vascular markings. Emphysema Alveolar wall destruction → large air spaces. “Barrel chest,” lucent lungs, bullae. Chronic Bronchitis Mucus hypersecretion and airway narrowing. Dirty chest, increased bronchovascular markings.
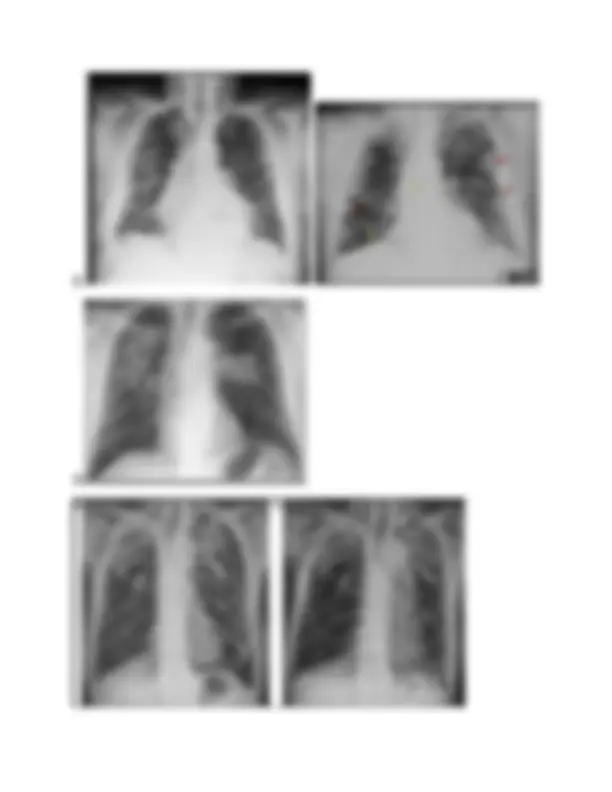
⚙️� 5. Occupational & Environmental Lung Diseases (Pneumoconioses)
**Disease Cause Imaging Findings
- Silicosis** Inhalation of silica dust. Multiple small nodules in upper lobes, calcified hilar nodes (“egg-shell” sign). 2. Asbestosis Inhalation of asbestos fibers. Pleural plaques, diffuse interstitial fibrosis, increased risk of mesothelioma. 3. Coal Worker’s Pneumoconiosis Carbon dust exposure. Diffuse reticulonodular pattern, especially upper lobes.